
A 51-year-old woman presented with lower back pain for one month. Her past medical history included breast carcinoma which was treated eighteen years ago with surgery and chemotherapy achieving complete remission. On admission, a full blood count showed a haemoglobin concentration of 95 g/L, a platelet count of 44 × 109/L and a leucocyte count of 18 × 109/L. Lactate dehydrogenase level was 1791 U/L (125–250). A peripheral blood smear showed erythroblasts (3/100 leukocytes) and left shift with no atypical cells.
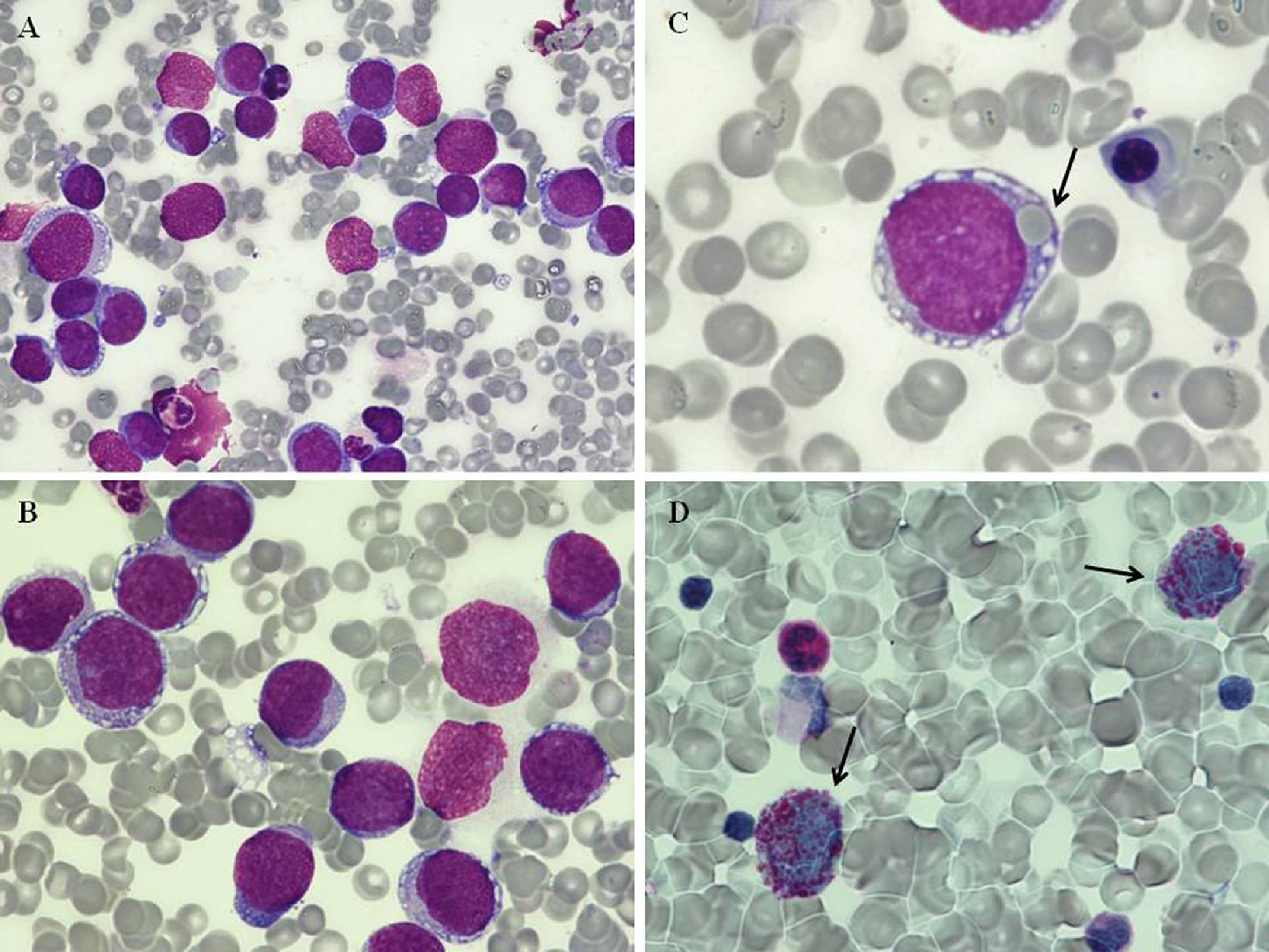
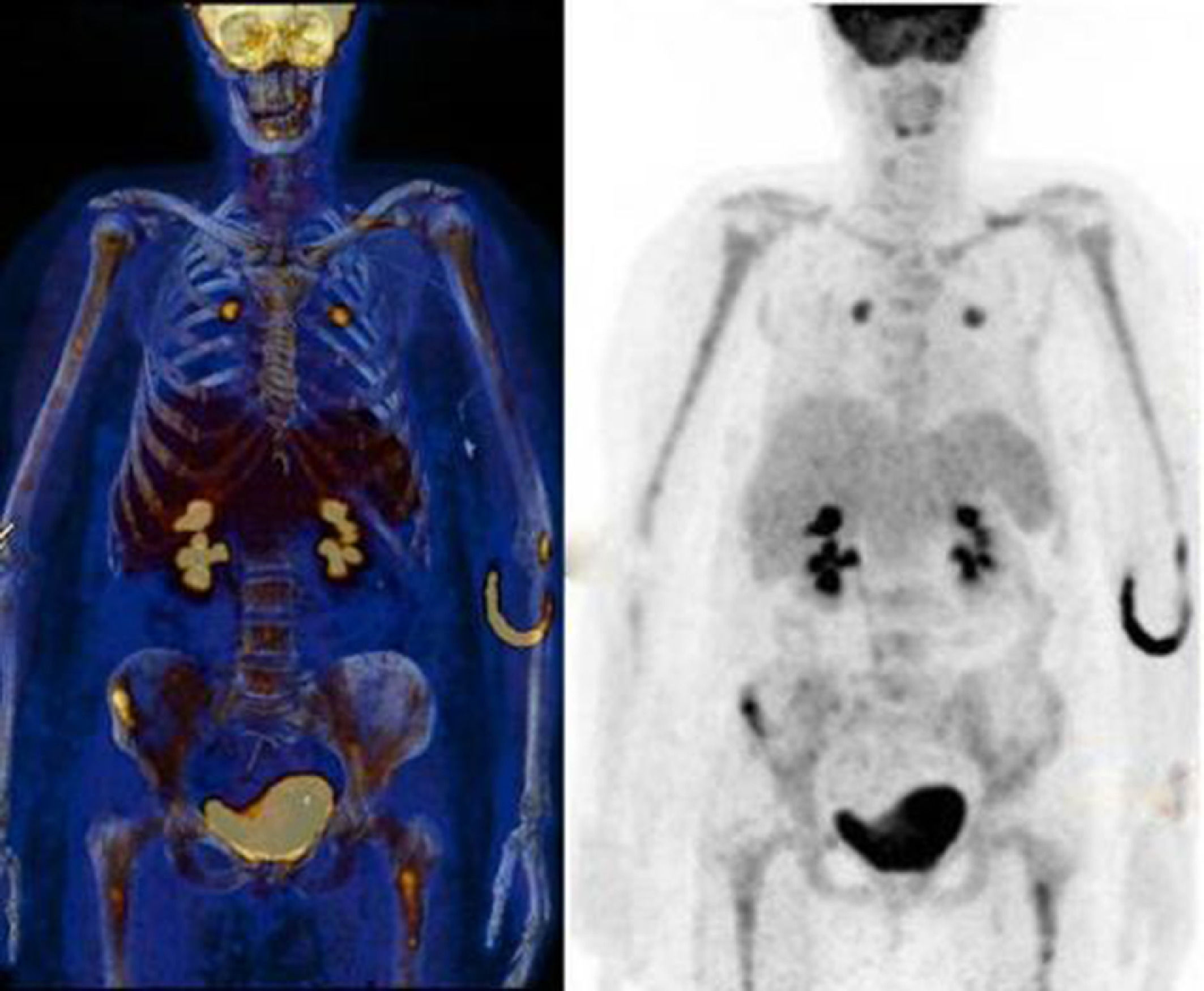
Due to bicytopenia, a bone marrow (BM) aspirate was performed revealing a diffuse infiltration by small to medium cells with blast-like cell appearance (Figure 1A and B). 5% of the abnormal cells showed erythrophagocytosis (Figure 1C). Cytochemical staining with Periodic Acid-Schiff (PAS) showed a prominent block-like cytoplasmic pattern in neoplastic cells (Figure 1D). Flow cytometric analysis showed strong expression of CD9 and CD56 with no expression of cyMPO, TdT, CD3, CD10, CD13, CD19, CD20, CD33, CD34, CD45, CD117 and HLADR. 18F-FDG-PET/CT revealed only a diffuse BM uptake with no evidence of a primary tumour (Figure 2). BM biopsy and immunohistochemistry were compatible with small cell undifferentiated carcinoma metastases (immunohistochemical staining was positive for CD56 but negative for CKAE1-AE3, CK7, CK20, TTF1, synaptophysin, oestrogen receptor, HER2, GATA-3, CD45 and CD20).
 Bone marrow aspirate smear showing diffuse infiltration by blast-like cells (May Grunwald Giemsa (MGG) stain, 60 ×, 100x). (C) Erythrophagocytosis by neoplastic cells (black arrows; MGG stain, 100 ×). (D) Block-like cytoplasmic pattern in neoplastic cells (black arrows; Periodic Acid-Schiff (PAS) stain, 100x).")
(A-B) Bone marrow aspirate smear showing diffuse infiltration by blast-like cells (May Grunwald Giemsa (MGG) stain, 60 ×, 100x). (C) Erythrophagocytosis by neoplastic cells (black arrows; MGG stain, 100 ×). (D) Block-like cytoplasmic pattern in neoplastic cells (black arrows; Periodic Acid-Schiff (PAS) stain, 100x).

BM metastases of solid tumours are sometimes difficult to distinguish from acute leukaemia,1,2 especially in some malignant diseases such as rhabdomyosarcoma, neuroblastoma, neuroendocrine tumours and small cell carcinoma2 and also if cytopenias or other unusual phenomena such as erythrophagocytosis coexist. Erythrophagocytosis by neoplastic cells is rare in haematological malignancies and is mainly observed in leukaemias. However, erythrophagocytosis by solid tumour cells is extremely rare.3 CD9 and CD56 are expressed in various normal cells and tissues, as well as in several solid tumours and haematological malignancies. After excluding an haematological neoplasm, a CD56+/CD45- immunophenotype suggests the possibility of neuroblastoma, small cell carcinoma, rhabdomyosarcoma, Ewing's sarcoma or a different type of neuroendocrine tumour.2 Integration of clinical and laboratory data, including a careful examination of blood and bone marrow films along with flow cytometric analysis, are essential to confirm the diagnosis of a non-haematological neoplasm in cases that mimic an haematological disorder.
Financial disclosureThe authors declared that this study received no financial support.


