
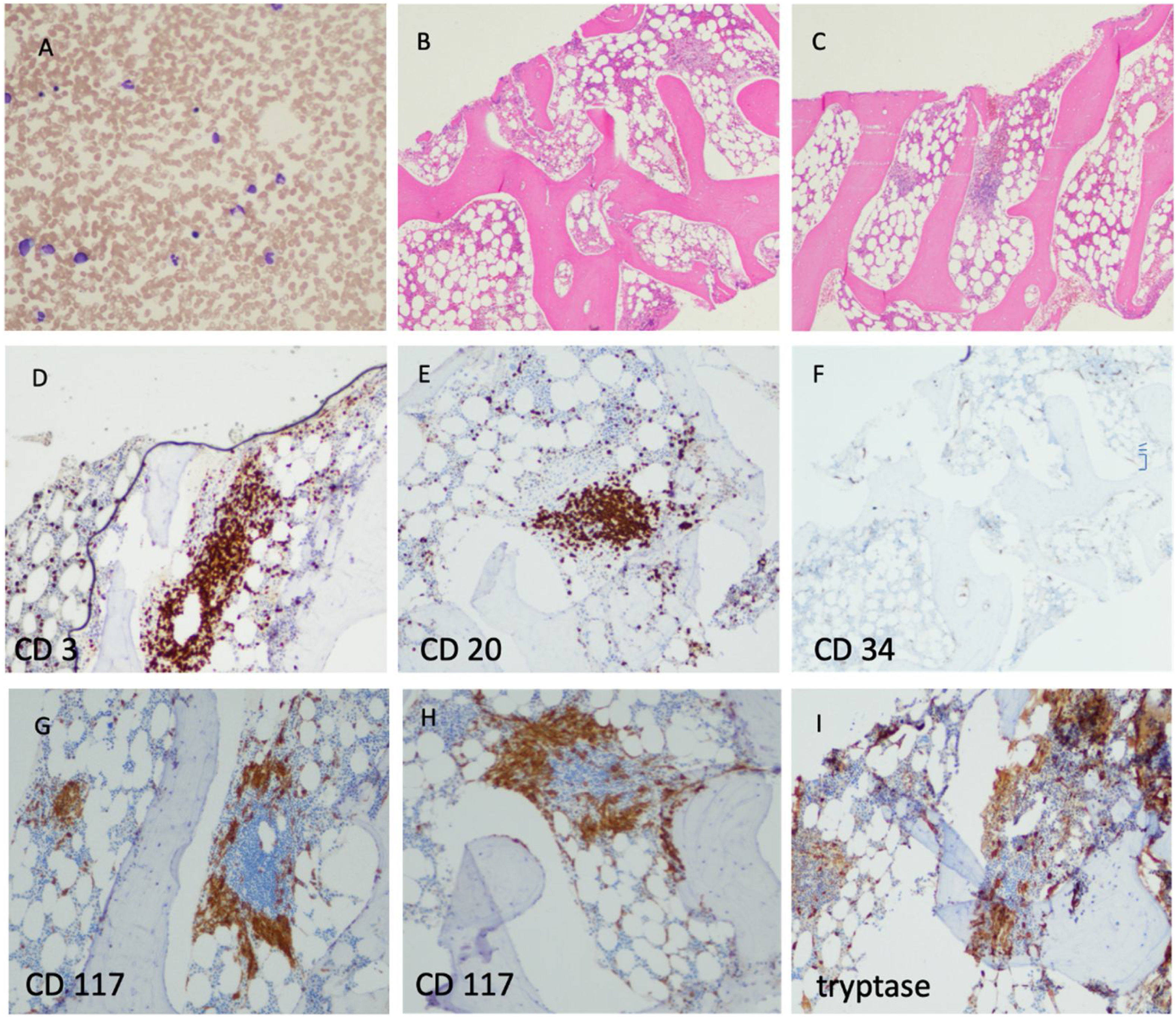
A 52-year-old female patient is described. The patient was referred to a dermatologist with a two-year history of lesions on her head and neck. She was noted to have red brown, non-scaly, slightly infiltrative papules with a positive Darier's sign, which was biopsy proven to be cutaneous mastocytosis. Further workup showed a markedly elevated serum tryptase levels (58.9 micrograms/L). She denied any abdominal pain, diarrhea, flushing, severe allergic reactions or any other systemic symptoms. In order to rule out systemic mastocytosis a bone marrow biopsy was requested. The CBC and the peripheral smear were unremarkable. A dilute bone marrow aspirate showed normal trilinear hematopoiesis and no evidence of increased myeloblasts or mast cells (Figure 1, panel A). A trephine biopsy showed nodular and paratrabecular mast cell lesions admixed with lymphocytes (Figure 1, panels B and C). Specifically both CD3+ T and CD20 + B-lymphocytes are admixed with the mast cell aggregates (Figure 1, panels D and E). CD34 showed no increase in myeloblasts (Figure 1, panel F). CD117 and tryptase confirmed large mast cell aggregates in the lesions seen on H&E (Figure 1, panels G–I). Quantitative PCR analysis identified the D816V mutation in the KIT gene and with no B or C symptoms the diagnosis of indolent systemic mastocytosis was reached.1 The patient is periodically monitored with imaging, CBCs and serum tryptase levels.

The authors declare no conflicts of interest.


