
A 84-year-old man presented with weakness, weight loss and lumbar pain from two weeks. He had history of dislypemia and diabetes. Complete blood count showed: hemoglobin 119 g/L, leukocyte count 4.7 × 109/L and platelet count 257 × 109/L. Serum protein study: M-component of IgM nature 3.23 g/dL with IgG immunoparesis. Full body scan showed D8 and L1 vertebral crush.
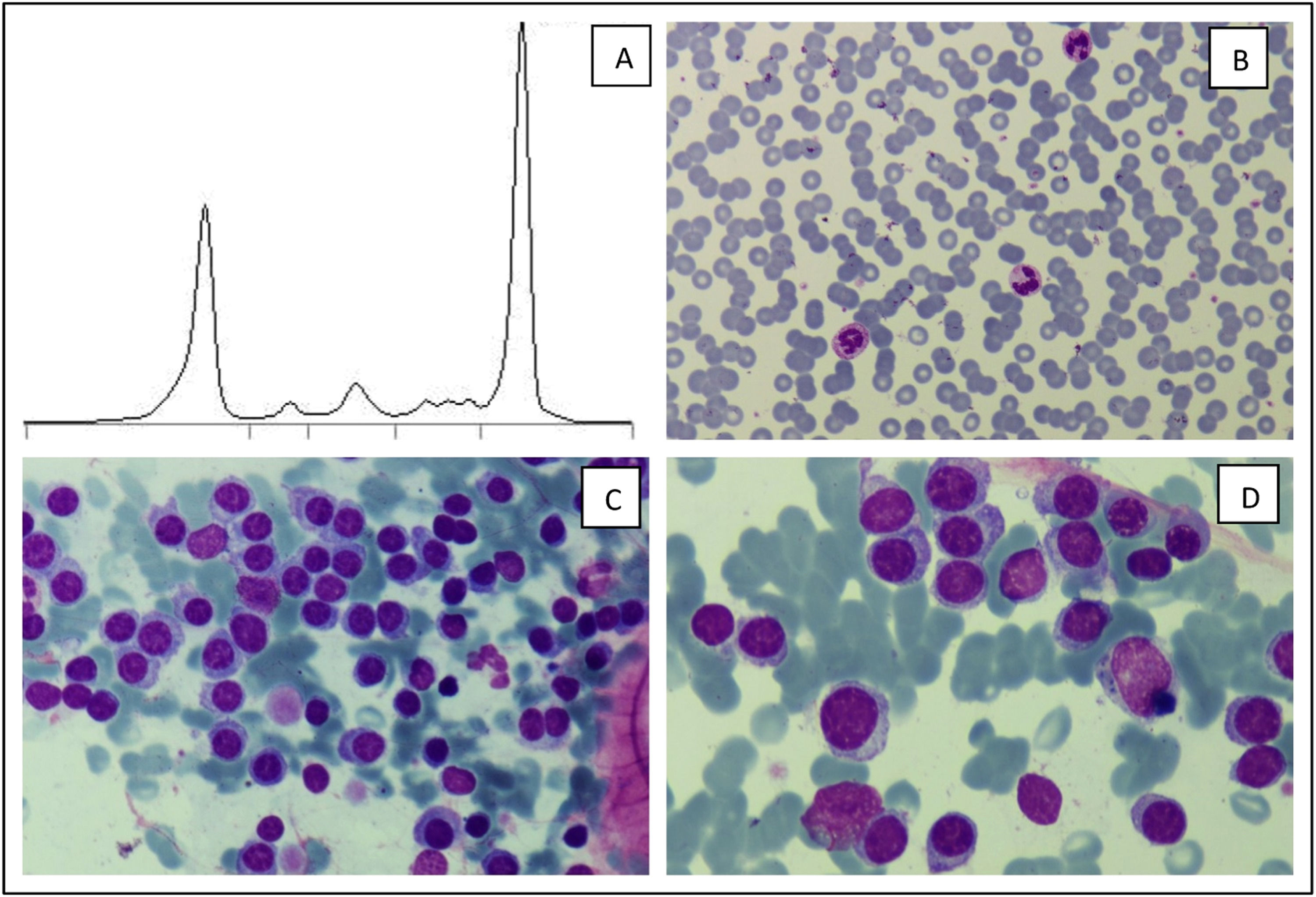
Bone marrow cytology showed a massive infiltration (87 %) by plasma cells with coarse cytoplasm nearly similar to lymphoplasmocytes (Figure 1). Flow cytometry confirmed clonality of plasma cells with phenotype: CD38++CD138+CD19-CD45-CD20+CD56-CD27+CD81+CD117-citKappa-citLambda+, and no lymphoid clonal population. FISH study displayed and t(11;14) and 1q gain. Mutation MYD88-LP by PCR was negative. Diagnosis of IgM multiple myeloma (MM) was made.
.")
IgM MM is uncommon (less than 0.5 % of all MM cases). IgM MM is characterized by the proliferation of clonal plasma cells that produce the IgM monoclonal component and, likely other MM types, symptoms of it. Sometimes clinical characteristics may overlap with other IgM related entities, Waldestrom Macroglobulinemia (MW) preferently, representing a challenge for clinicians. IgM MM is characterized by a proliferation of clonal plasma cells: CD38+, CD138+, CD20-, CD19- and usually CD56- and CD117-. In contrast MW clonal population is normally CD45+, CD19+, CD20+, CD22+, CD25+, CD27+, CD23-, CD5-, CD10-and CD138-. The presence of t(11;14) is shown in IgM MM but absent in WM. The presence of MYD88 mutation is usually absent in IgM MM; in contrast is very characteristic of WM. Since the treatment and prognosis of these two hematological disorders is very different, a correct diagnosis is mandatory.1,2


