

The aim of this study was to examine the association between religiousness and blood donation among postgraduate students.
MethodsThe Portuguese-language version of the Duke University Religion Index was administered to a sample of 226 Brazilian students with ages ranging from 22 to 55 years. All study participants had completed undergraduate courses in health-related areas.
ResultsIn the present study, 23.5% of the students were regular donors. Organizational religiousness was found to be associated with attitudes related to blood donation. This study also shows evidence that regular blood donors have a higher intrinsic religiousness than subjects who donate only once and do not return.
ConclusionThis study shows that the attitudes concerning blood donation may have some association with religiosity.
In Brazil, blood donation has not been remunerated in any way since 1980.1 The implementation of an altruistic donation model brought the need for strategies to encourage the population to donate blood voluntarily and regularly. It has been suggested that an understanding of the characteristics of donor groups provides information for the development of effective recruitment and retention strategies.2,3 While about 5% of people in the United States donate blood each year,3 less than 2% of the Brazilian population do it regularly.4 In Brazil, it is estimated that only 40% of people return within one year after the first donation and 53% within two years.5 In addition, it is estimated that 30% never return to donate after the first donation.
Information about opinions, motivation and feelings of blood donors is important for the organization and administration of blood centers6 as well as to establish a profile of these individuals. This information can serve as a basis for the elaboration of projects that aim to educate, mobilize, attract and retain regular voluntary donors.
Published articles on the motivation and recruitment of blood donors have described that altruism/humanitarianism, sense of solidarity or duty, social pressure, replacement and reward, and possible personal or family benefits are the main reasons for donation.7–9 In addition, the study by Gonçalez et al.10 showed that altruism is the main motivator for blood donation in Brazil, although Oliveira et al.11 warned that many of the Brazilian blood donors could be motivated for reasons that are not exclusively altruistic, such as seeking tests. Pessi12 showed that attitudes and acts of altruism are indeed linked to religiosity. If people with religious ties contribute more actively to charitable practices, it is expected that there is some relationship between religiosity and attitudes concerning blood donation. In fact, Abohghasemi et al.13 showed that after altruism, religious beliefs are the most common positive motivation for blood donation among Iranians. In a Canadian study,14 it was found that 7.6% of the respondents reported that religious convictions motivated them to start donating blood. However, in the report on religiousness and blood donation in a large and nationally representative sample of young adults published by Gillum and Masters,15 religiousness was not associated with a history of blood donation in men, with the exception of higher donation rates among Catholic men aged 35–44 years old. In addition, a North American study,16 on investigating the relationship of sociodemographic and attitudinal factors with a history of blood donation among the general public, did not find a significant association between religious and spiritual salience and prior history of donation.
Thus, in order to bring more light on this issue, the purpose of the present study was to examine the association between religiousness and blood donation among Brazilian postgraduate students. The attitudes of postgraduate students of health-related areas toward blood donation can be of great importance as they are potentially ‘opinion leaders’ on social and public health topics, considering that their future activities will be focused on education and healthcare.
MethodsStudy population and data collectionThe present study included a convenient sample of Brazilian postgraduate students, with data being collected in classrooms during class time in 2012 and 2013 in the Ribeirão Preto Medical School of the Universidade de São Paulo (FMRP-USP). After a brief rapport-building period, the subjects were informed that they would be invited to answer a self-administered questionnaire to give information on gender, age, profession, social standards, and attitudes toward blood donation and religion. A total of 273 subjects agreed to participate in the study with about 3% declining to participate. The interviews were conducted during classes of Biostatistics, which are of interest to students of several postgraduate courses offered in the university campus. The researchers stayed in the classroom during the application of the questionnaire and clarified any doubts that came up. The questionnaire answers were anonymous. Forty-seven subjects were excluded from the study because they declared that they were not able to donate blood (body weight under 50kg or undeclared reasons). Thus, a final sample of 226 subjects was used in the data analysis. Ethical approval was obtained from the Research Ethics Committee of the Hospital das Clinicas of FMRP-USP.
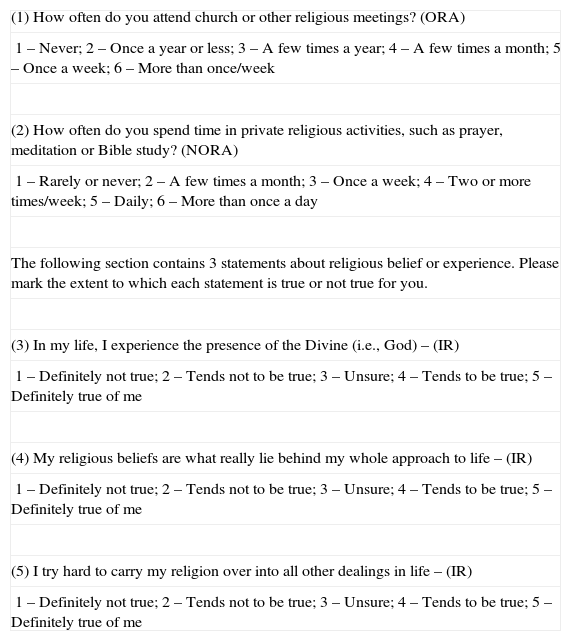
QuestionnaireThe scoring of the Duke University Religion (DUREL) index was employed as a measure of religiosity.17,18 The DUREL index includes a Likert-type scale to assess five items that capture the three dimensions of religiosity that most closely relate to health outcomes: organizational religiousness (ORA), non-organizational religiousness (NORA), and intrinsic religiousness (IR). The ORA and NORA dimensions of six-item subscales are obtained directly from the first two items of the DUREL index, with the IR subscale being obtained by summing the answers to the final three items (ranging from 3 to 15 points). IR is measured by God's presence as experienced in the lives of people, the relation between religious beliefs and approach to life, and the effort to live religion in all aspects of life (Table 1).18
Items of the Duke University Religion Index (DUREL).
| (1) How often do you attend church or other religious meetings? (ORA) |
| 1 – Never; 2 – Once a year or less; 3 – A few times a year; 4 – A few times a month; 5 – Once a week; 6 – More than once/week |
| (2) How often do you spend time in private religious activities, such as prayer, meditation or Bible study? (NORA) |
| 1 – Rarely or never; 2 – A few times a month; 3 – Once a week; 4 – Two or more times/week; 5 – Daily; 6 – More than once a day |
| The following section contains 3 statements about religious belief or experience. Please mark the extent to which each statement is true or not true for you. |
| (3) In my life, I experience the presence of the Divine (i.e., God) – (IR) |
| 1 – Definitely not true; 2 – Tends not to be true; 3 – Unsure; 4 – Tends to be true; 5 – Definitely true of me |
| (4) My religious beliefs are what really lie behind my whole approach to life – (IR) |
| 1 – Definitely not true; 2 – Tends not to be true; 3 – Unsure; 4 – Tends to be true; 5 – Definitely true of me |
| (5) I try hard to carry my religion over into all other dealings in life – (IR) |
| 1 – Definitely not true; 2 – Tends not to be true; 3 – Unsure; 4 – Tends to be true; 5 – Definitely true of me |
The DUREL index was translated into Portuguese by Moreira-Almeida et al.,19 and it was initially validated by Lucchetti et al.20 Taunay21 studied internal consistency, test–retest reliability and convergent-discriminant validity of the Portuguese-language version of DUREL (P-DUREL) by considering two different samples (university students and psychiatric outpatients). Posteriorly, Martinez et al.22 validated the P-DUREL in a sample of postgraduate students.
In this study the subjects were classified into four groups according to their attitudes toward blood donation. Group 1 was constituted by individuals who donated only once and intended to return to donate again; Group 2 was composed of regular blood donors; Group 3 was composed of individuals who had never donated blood, but wished to become donors; and Group 4 was composed of individuals who had never donated blood and did not intend to become donors, or by individuals who donated only once and did not intend to return to donate again. This classification was created by Almeida et al.,23 who studied the spiritual well-being between individuals who are not adept to blood donation and those who donate regularly.
Statistical analysisThe association between the attitudes toward blood donation and several social standards was studied using logistic regression models. Gender and age were included in this analysis as possible confounding factors.
Regression models based on beta-binomial distribution24,25 were used to study the association between P-DUREL scores and attitudes toward blood donation, with adjustments by gender and age. An attempt was made to fit the data to models based on binomial and negative binomial distributions,26 but the model based on beta-binomial distribution gave a better fit than the others. In this study, the binomial and negative binomial distributions were inadequate to describe the over-dispersion of the P-DUREL scores, and consequently the beta-binomial distribution was used.
All regression models were fitted to data using Bayesian inference methods27 with non-informative prior distributions for all model parameters. Both Bayesian parameter estimates and associated 95% credible intervals (95% CIs) were obtained with the OpenBUGS software. Credible intervals are the Bayesian analogs of confidence intervals. Posterior summaries of interest were obtained from simulated samples of the respective joint posterior distributions using standard Markov Chain Monte Carlo (MCMC) methods and the Gibbs sampling algorithm.28
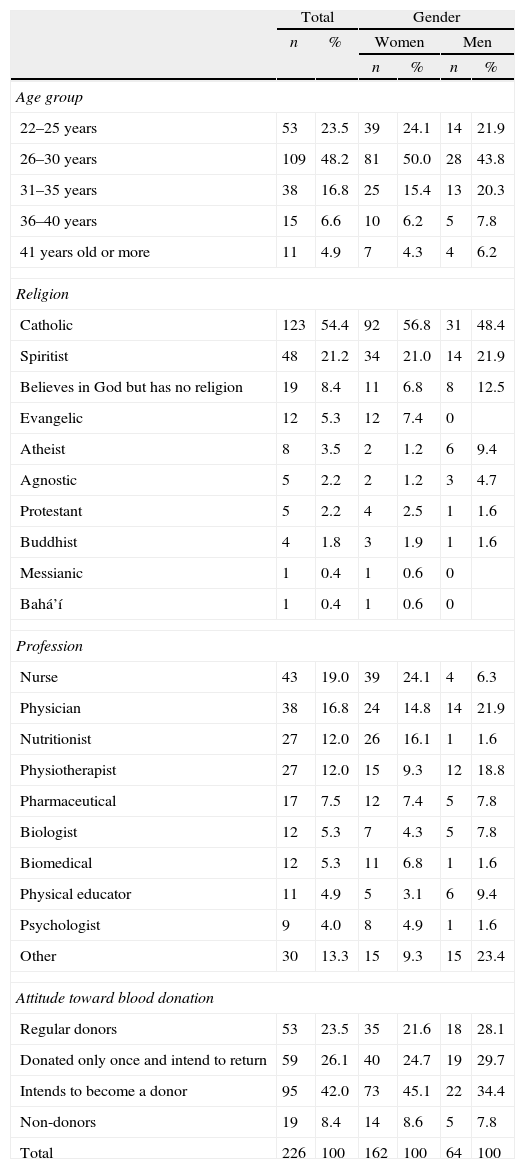
ResultsSeventy-two percent of the subjects who participated in the study were women with a mean age of 29.0 years (range: 22–52 years old) and twenty-eight percent were men with a mean age of 30.3 years (range: 23–55 years old). Table 2 shows the characteristics of the participants. The most common religious affiliations were Catholicism (54.4%), and Kardecist Spiritism (21.2%). Kardecist Spiritism is a religion with aspects of science and philosophy that originated in France in the 18th century and was popularized in Brazil in the mid-20th century. An inspection of the data in Table 2 suggests that women are more likely to have religious affiliations, considering that the frequency of atheists and agnostics is higher among men than among women (14.1% versus 2.4%, respectively).
Characteristics of the 226 subjects who participated in the study.
| Total | Gender | |||||
| n | % | Women | Men | |||
| n | % | n | % | |||
| Age group | ||||||
| 22–25 years | 53 | 23.5 | 39 | 24.1 | 14 | 21.9 |
| 26–30 years | 109 | 48.2 | 81 | 50.0 | 28 | 43.8 |
| 31–35 years | 38 | 16.8 | 25 | 15.4 | 13 | 20.3 |
| 36–40 years | 15 | 6.6 | 10 | 6.2 | 5 | 7.8 |
| 41 years old or more | 11 | 4.9 | 7 | 4.3 | 4 | 6.2 |
| Religion | ||||||
| Catholic | 123 | 54.4 | 92 | 56.8 | 31 | 48.4 |
| Spiritist | 48 | 21.2 | 34 | 21.0 | 14 | 21.9 |
| Believes in God but has no religion | 19 | 8.4 | 11 | 6.8 | 8 | 12.5 |
| Evangelic | 12 | 5.3 | 12 | 7.4 | 0 | |
| Atheist | 8 | 3.5 | 2 | 1.2 | 6 | 9.4 |
| Agnostic | 5 | 2.2 | 2 | 1.2 | 3 | 4.7 |
| Protestant | 5 | 2.2 | 4 | 2.5 | 1 | 1.6 |
| Buddhist | 4 | 1.8 | 3 | 1.9 | 1 | 1.6 |
| Messianic | 1 | 0.4 | 1 | 0.6 | 0 | |
| Bahá’í | 1 | 0.4 | 1 | 0.6 | 0 | |
| Profession | ||||||
| Nurse | 43 | 19.0 | 39 | 24.1 | 4 | 6.3 |
| Physician | 38 | 16.8 | 24 | 14.8 | 14 | 21.9 |
| Nutritionist | 27 | 12.0 | 26 | 16.1 | 1 | 1.6 |
| Physiotherapist | 27 | 12.0 | 15 | 9.3 | 12 | 18.8 |
| Pharmaceutical | 17 | 7.5 | 12 | 7.4 | 5 | 7.8 |
| Biologist | 12 | 5.3 | 7 | 4.3 | 5 | 7.8 |
| Biomedical | 12 | 5.3 | 11 | 6.8 | 1 | 1.6 |
| Physical educator | 11 | 4.9 | 5 | 3.1 | 6 | 9.4 |
| Psychologist | 9 | 4.0 | 8 | 4.9 | 1 | 1.6 |
| Other | 30 | 13.3 | 15 | 9.3 | 15 | 23.4 |
| Attitude toward blood donation | ||||||
| Regular donors | 53 | 23.5 | 35 | 21.6 | 18 | 28.1 |
| Donated only once and intend to return | 59 | 26.1 | 40 | 24.7 | 19 | 29.7 |
| Intends to become a donor | 95 | 42.0 | 73 | 45.1 | 22 | 34.4 |
| Non-donors | 19 | 8.4 | 14 | 8.6 | 5 | 7.8 |
| Total | 226 | 100 | 162 | 100 | 64 | 100 |
All study participants had completed undergraduate courses in health-related areas. Table 2 shows that the most common professions were nurses (19.0%), followed by physicians, nutritionists, physiotherapists, pharmaceuticals, biologists, biophysicians, physical educators, and other professionals with frequencies of less than 10 representatives. A total of 21.6% of the women who participated in the study were regular blood donors, in comparison with 28.1% of the men.
Table 3 shows the students’ blood donation attitudes with regard to social standards. The regular donors participating in the study had a higher frequency of people in their homes who also donated blood (64% versus 40% of the students who intended to become donors and 32% in the non-donor group). The results in Table 3 also suggest that the frequency of close friends disapproving of people who refused to donate blood is higher among blood donors compared with students intending to become a donor. In addition, the presence of close friends who donated blood was more common among regular donors than among non-donors and students who intended to become a donor.
Attitudes toward blood donation with regard to social standards. Significant differences between the frequencies of responses of regular donors and other groups are marked by asterisks.
| Regular donors | Donated only once and intend to return | Intends to become a donor | Non- donors | |||||
| n | % | n | % | n | % | n | % | |
| Are there blood donors at your home? | 34 | 64 | 29 | 49 | 38 | 40* | 6 | 32* |
| Do you have friends who talk to you about the importance of blood donation? | 39 | 74 | 39 | 66 | 72 | 76 | 13 | 68 |
| Have you ever felt obliged or pressured by people to donate blood? | 8 | 15 | 5 | 8 | 15 | 16 | 5 | 26 |
| Do you feel totally free to practice your beliefs and convictions? | 49 | 92 | 49 | 83 | 90 | 95 | 16 | 84 |
| Do you have close friends who disapprove about people's refusal to donate blood? | 21 | 40 | 16 | 27 | 22 | 23* | 7 | 37 |
| Are most of your close friends blood donors? | 25 | 47 | 24 | 41 | 21 | 22* | 4 | 21* |
| Have you ever felt obliged to donate blood when you found out about a person who needed a donation? | 21 | 40 | 12 | 20* | 27 | 28 | 6 | 32 |
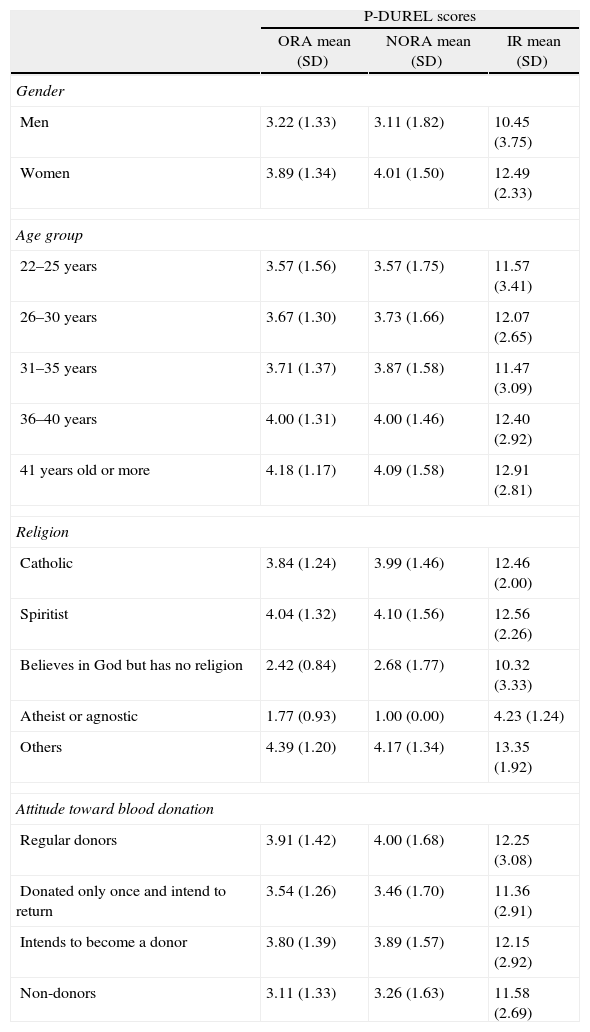
Table 4 lists the means and standard deviations for the ORA, NORA and IR dimensions of the P-DUREL, according to gender, age, religion, and attitude toward blood donation.
Descriptive statistics (mean and standard deviation – SD) for the three dimensions of religiosity (ORA, NORA and IR) measured by P-DUREL, according to gender, age, religion and attitude toward blood donation.
| P-DUREL scores | |||
| ORA mean (SD) | NORA mean (SD) | IR mean (SD) | |
| Gender | |||
| Men | 3.22 (1.33) | 3.11 (1.82) | 10.45 (3.75) |
| Women | 3.89 (1.34) | 4.01 (1.50) | 12.49 (2.33) |
| Age group | |||
| 22–25 years | 3.57 (1.56) | 3.57 (1.75) | 11.57 (3.41) |
| 26–30 years | 3.67 (1.30) | 3.73 (1.66) | 12.07 (2.65) |
| 31–35 years | 3.71 (1.37) | 3.87 (1.58) | 11.47 (3.09) |
| 36–40 years | 4.00 (1.31) | 4.00 (1.46) | 12.40 (2.92) |
| 41 years old or more | 4.18 (1.17) | 4.09 (1.58) | 12.91 (2.81) |
| Religion | |||
| Catholic | 3.84 (1.24) | 3.99 (1.46) | 12.46 (2.00) |
| Spiritist | 4.04 (1.32) | 4.10 (1.56) | 12.56 (2.26) |
| Believes in God but has no religion | 2.42 (0.84) | 2.68 (1.77) | 10.32 (3.33) |
| Atheist or agnostic | 1.77 (0.93) | 1.00 (0.00) | 4.23 (1.24) |
| Others | 4.39 (1.20) | 4.17 (1.34) | 13.35 (1.92) |
| Attitude toward blood donation | |||
| Regular donors | 3.91 (1.42) | 4.00 (1.68) | 12.25 (3.08) |
| Donated only once and intend to return | 3.54 (1.26) | 3.46 (1.70) | 11.36 (2.91) |
| Intends to become a donor | 3.80 (1.39) | 3.89 (1.57) | 12.15 (2.92) |
| Non-donors | 3.11 (1.33) | 3.26 (1.63) | 11.58 (2.69) |
ORA: organizational religiousness; NORA: non-organizational religiousness; IR: intrinsic religiousness.
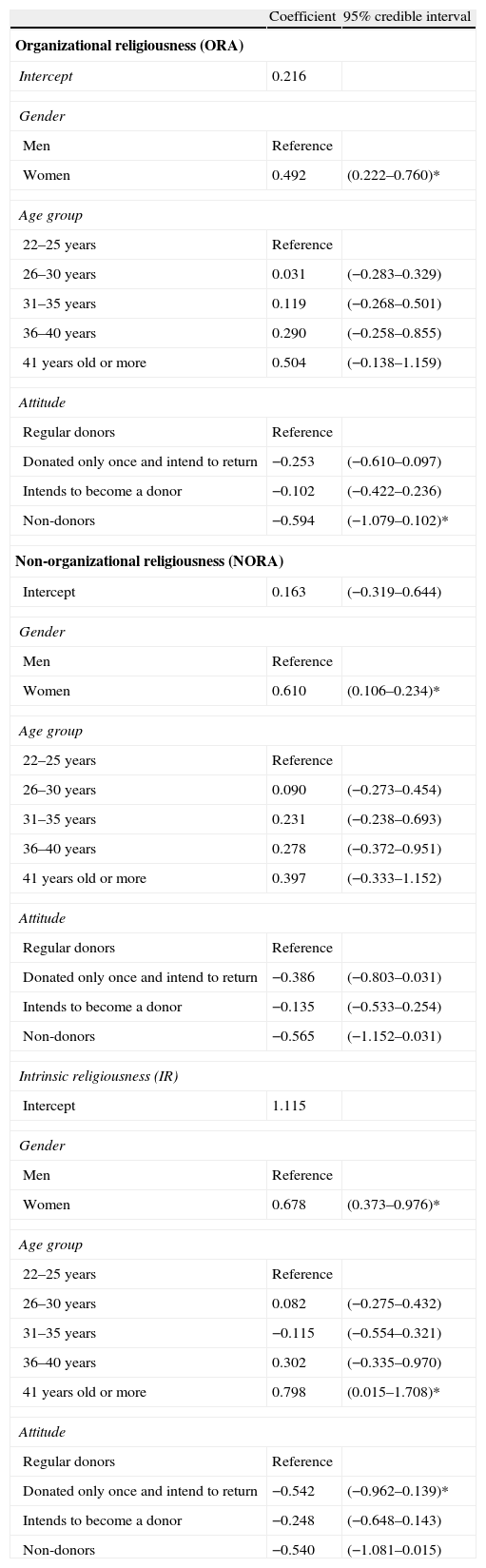
Table 5 shows the results of the beta-binomial regression analyses, including ORA, NORA and IR scores as dependent variables and gender, age group and blood donation attitude as independent variables. The coefficients shown in this table are measures of the effect of each covariate on the mean values of the dependent variable in a logit scale.25 Coefficients higher than zero are suggestive of a positive association, whereas coefficients of less than zero are suggestive of a negative association. Ninety-five percent credible intervals different from zero suggest significant associations. The intercept is a constant value, that is, the value of the link function when all the independent variables are equal to zero. Thus, the regression analysis suggests that women tend to have higher mean ORA, NORA and IR scores than men. Regular donors tend to have higher mean ORA scores than non-donors, and regular donors tend to have higher mean IR scores than students who donated only once and intend to return. In addition, students older than 40 years tend to have higher mean IR scores.
Results from beta-binomial regression analysis with the ORA, NORA and IR scores as dependent variables. Credible intervals different from zero are marked by asterisks (similar to p-value <0.05).
| Coefficient | 95% credible interval | |
| Organizational religiousness (ORA) | ||
| Intercept | 0.216 | |
| Gender | ||
| Men | Reference | |
| Women | 0.492 | (0.222–0.760)* |
| Age group | ||
| 22–25 years | Reference | |
| 26–30 years | 0.031 | (−0.283–0.329) |
| 31–35 years | 0.119 | (−0.268–0.501) |
| 36–40 years | 0.290 | (−0.258–0.855) |
| 41 years old or more | 0.504 | (−0.138–1.159) |
| Attitude | ||
| Regular donors | Reference | |
| Donated only once and intend to return | −0.253 | (−0.610–0.097) |
| Intends to become a donor | −0.102 | (−0.422–0.236) |
| Non-donors | −0.594 | (−1.079–0.102)* |
| Non-organizational religiousness (NORA) | ||
| Intercept | 0.163 | (−0.319–0.644) |
| Gender | ||
| Men | Reference | |
| Women | 0.610 | (0.106–0.234)* |
| Age group | ||
| 22–25 years | Reference | |
| 26–30 years | 0.090 | (−0.273–0.454) |
| 31–35 years | 0.231 | (−0.238–0.693) |
| 36–40 years | 0.278 | (−0.372–0.951) |
| 41 years old or more | 0.397 | (−0.333–1.152) |
| Attitude | ||
| Regular donors | Reference | |
| Donated only once and intend to return | −0.386 | (−0.803–0.031) |
| Intends to become a donor | −0.135 | (−0.533–0.254) |
| Non-donors | −0.565 | (−1.152–0.031) |
| Intrinsic religiousness (IR) | ||
| Intercept | 1.115 | |
| Gender | ||
| Men | Reference | |
| Women | 0.678 | (0.373–0.976)* |
| Age group | ||
| 22–25 years | Reference | |
| 26–30 years | 0.082 | (−0.275–0.432) |
| 31–35 years | −0.115 | (−0.554–0.321) |
| 36–40 years | 0.302 | (−0.335–0.970) |
| 41 years old or more | 0.798 | (0.015–1.708)* |
| Attitude | ||
| Regular donors | Reference | |
| Donated only once and intend to return | −0.542 | (−0.962–0.139)* |
| Intends to become a donor | −0.248 | (−0.648–0.143) |
| Non-donors | −0.540 | (−1.081–0.015) |
While many authors have postulated that religiosity correlates strongly with participating in charitable actions, Otto and Bolle29 suggested that overall altruism is related to charity giving, but not to blood donation behavior. Thus, it is possible that the various aspects of altruism link differently to specific behaviors, and consequently, attitudinal factors toward blood donation involve a complex set of values, satisfaction with services, trust, fear and feelings. Although religiousness is an important feature of human behavior, there are few studies in the literature directly dealing with the possible relationship between religiousness and blood donation. Gillum and Masters15 state that they conducted the first report on religiousness and blood donation in a large, nationally representative sample of young adults. However, these authors did not find any direct connection between religiousness and history of blood donation. Unlike this important report, the present study finds that, in a specific group of university students, religiousness can be a factor that potentially influences the decision to donate blood.
The major limitation of the present study lies in the characteristics of the subjects. The analyses were performed in a restricted population of individuals who had graduated in courses in health-related areas and they thus tend to be knowledgeable of the importance of blood donation. In addition, they were mostly women. All these factors complicate the extrapolation of the results to broader populations. Contact with the university environment, where the practice of blood donation is highly regarded is, per se, a factor that influences the decision to donate blood. In fact, the results in Table 2 show that 23.5% of the participants are regular donors, whereas less than 2% of the Brazilian population donates blood regularly.4 Despite these limitations, the results of the present study are potentially important for the following reasons. Firstly, there is a lack of studies of possible associations between religiousness and attitudes toward blood donation, mainly using validated instruments. Even the study by Gillum and Master,15 which highlighted the relationship between religiousness and blood donation, did not use a validated instrument to assess religiousness. In this aspect, the present study is thus innovative although the results are restricted to a group of people with particular characteristics. Secondly, the results show that religiousness is inserted in this context as an example of dimension that can stimulate blood donation among these individuals, even though they receive other stimuli from the environment in which they live. It is hoped that the future professional activities of these students will be directed to community healthcare and teaching to promote health. Thus, these subjects may play an important role in spreading the importance of donating blood in the community. Thus, the results of this article are useful to understand this process. Thirdly, the results of this study can encourage further investigations about the role of religiousness in the blood donation decision-making process in respect to other specific populations of interest or a broader population. Hence, these studies can help to develop effective interventions to improve the retention and recruitment of new blood donors. Another possible limitation of this study is that the statistical regression model did not include socioeconomic variables to minimize possible confounding effects. However, the study used a sample in which all subjects had completed a university degree and it is thus assumed that there is not great heterogeneity among them in terms of socioeconomic factors. This would reduce a possible confounding effect in relation to these variables.
Statistical analysis shows that regular donors have higher religiosity scores than non-donors, suggesting that this may be a predictor of attitudes about blood donation. The participation in religious organizations can encourage relationships with people who have values and attitudes that encourage blood donation, and the results in Table 3 suggest that regular donors have contact with people, socially or within their families, who also donate blood. This result is corroborated by Healy,30 who hypothesized that people involved in religious organizations are more likely to donate blood. Considering that participants in the present study have good access to health information, it is clear that knowledge is not sufficient to influence the attitude of the individual toward blood donation. In accordance with Renaud and Bouchard,31 individuals just assume a given behavior when they are inserted in a social network that encourages such a behavior. Thus, social networks and active participation within religious circles would be a remarkable aspect of the association between blood donation and organizational religiousness, an issue that deserves to be explored in more detail in further studies.
Non-organizational religiousness, expressed by private religious activities such as prayer, meditation, and reading of religious books, has been related to poorer physical health.32 However, this should not apply to the participants in this study because they are health professionals and have good access to information and health services. The present study shows that female students have higher non-organizational religiousness than male students, but this finding does not allow us to state that non-organizational religiousness is associated with blood donation. Sample means for NORA scores are higher for regular donors than for non-donors (Table 4), but there is no evidence that this may be extrapolated to a broad population (the corresponding credible intervals contain zero; Table 5). However, further studies using larger samples should be encouraged in order to verify whether this absence of evidence is a consequence of a possible low power for hypothesis testing.
The present study also evidenced a relationship between intrinsic religiousness (IR) and attitudes toward blood donation. In addition to the studies that reckoned that positive aspects of religiousness are conducive to maintaining mental health in medically ill patients,33 the findings of the present study reinforce the condition that religiousness is also intertwined with altruistic acts potentially beneficial to the health of the community. New studies should be encouraged to bring new insights in the understanding of the role played by the different dimensions of religiosity in the intention to donate blood, return for further donations, and to practice altruistic attitudes concerning the promotion of health.
Conflicts of interestThe authors declare no conflicts of interest.
This study was supported by Fundação de Apoio ao Ensino, Pesquisa e Assistência (FAEPA – HC-FMRP) and Conselho Nacional de Pesquisa (CNPq) (process 305942/2012-3).



