
A 33-year-old man, without medical history, presented with weakness, dyspnea and hemoptysis. Laboratory findings included hemoglobin 840 g/L, platelets 63×109/L, leukocytes 10.1 × 109/L; and elevated C-reactive protein, gamma-glutamyltranspeptidase, alkaline phosphatase, and lactate dehydrogenase. A manual cell count revealed left swift and 2 % erythroblasts. Full body PET-CT scan showed hypermetabolic lymph nodes and heterogeneous captation in bone (Figure 1A). Bone marrow aspirate was difficult with few sample obtained. Bone marrow smear showed aggregates of immature cells that were positive to periodic acid-Schiff suggesting metastatic infiltration (Figures 1B-C); and many osteoclasts (Figures 1D-F). Flow cytometry displayed an increase of CD45 negative population (18 %) that was also negative for HLADR, CD10, CD5, CD71, CD117, CD1a, CD15 and BerEp4. The patient worsened rapidly and deceased two days after the procedure. Necropsy showed metastatic ganglium and vertebral infiltration by epithelial proliferation positive to CK7, CK20 and CK19 and negative to TTF-1, GATA3, napsinA and mammaglobin.
. C. Cluster of metastatic cells PAS positive in bone marrow (Periodic Acid-Schiff staining x500). D-F: Different osteoclasts in bone marrow (May-Grünwald Giemsa x1000).")
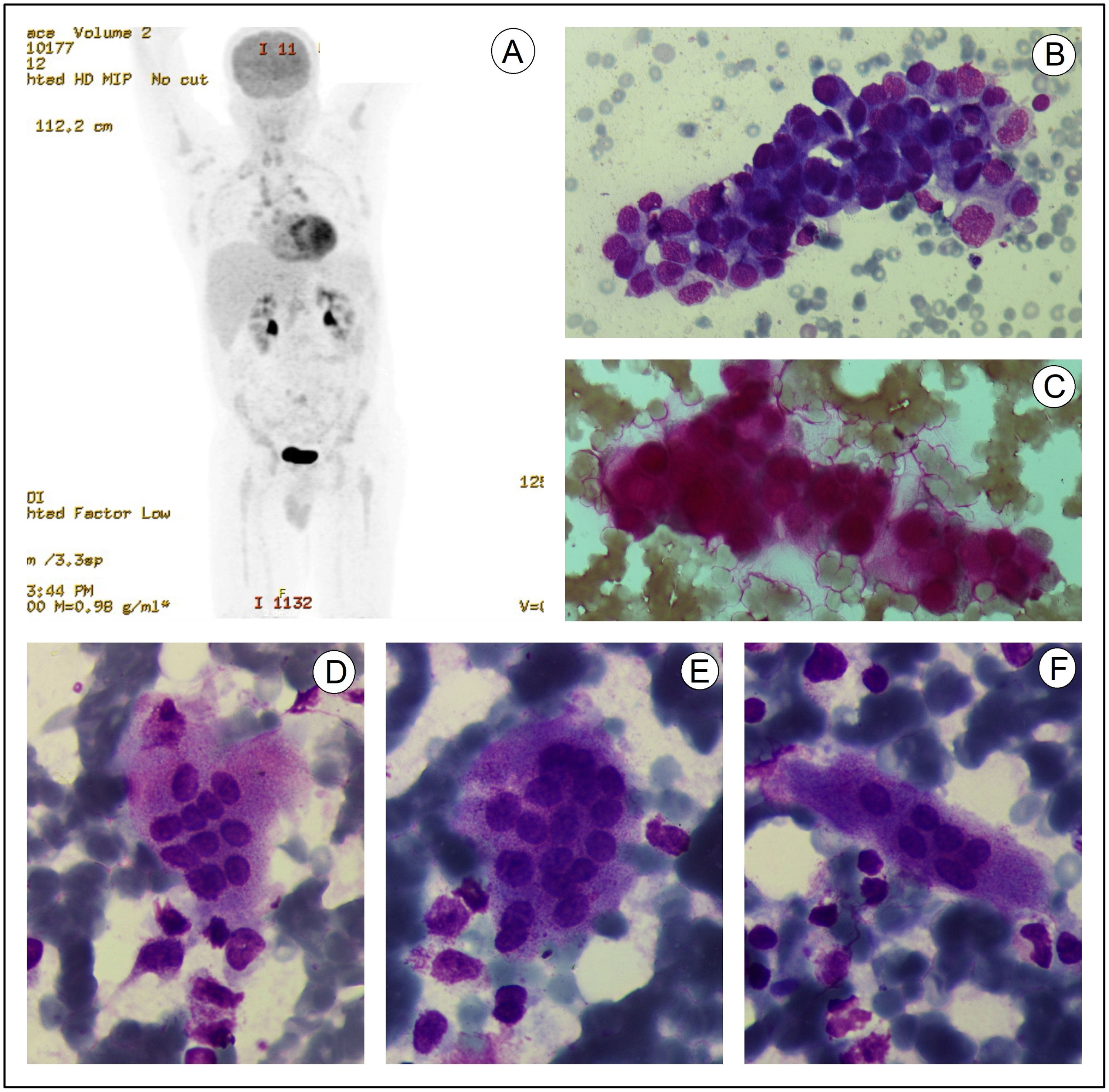
A: PET image showing supradiaphragmatic and infradiaphragmatic hypermetabolic lymph nodes and heterogeneous captation in bone. B: Bone marrow aspirate smear showing aggregates of medium-sized cells with scant and agranullar cytoplasm and nucleus with lax chromatin (May-Grünwald Giemsa x500). C. Cluster of metastatic cells PAS positive in bone marrow (Periodic Acid-Schiff staining x500). D-F: Different osteoclasts in bone marrow (May-Grünwald Giemsa x1000).
Osteoclasts are multinucleated cells that originates from monocytic lineage; and, in physiological conditions, they participate in bone remodelling, calcium homeostasis and osteoimmunity. In pathological conditions, like metastasis, osteoclasts play an active role. In addition, metastatic cells are able to perturb the bone microenvironment influencing in osteoclast formation and activity.1 For these reason the development of target-specific therapies like osteoclast inhibitors has accelerated in recent years.2
The visualization of osteoclasts in bone marrow smear is rare and they should not be confused with dysplastic megakaryocytes.
In the presence of leucoerythroblastic syndrome, performing a bone marrow aspirate is a quick test that can screen the presence of metastasis and may orientate the need to search for a primary tumor.


