


The level of satisfaction of donors with the blood donation system is an important factor which influences their intent to return for future donation. A 25-item questionnaire on the satisfaction of blood donors has been recently proposed to assess the donor satisfaction with the service provided by a blood bank. The objective of this study was to present a proposal for application and interpretation of a BDSQ considering a sample of blood donors of a Brazilian blood bank.
MethodsA sample of 1019 blood donors at the Regional Hemotherapy Center of Franca, Brazil, answered the BDSQ. A top-box analysis was used to assess the associations between the variables characterizing the profiles of blood donors and their overall satisfaction with the service provided by the blood bank. We proposed the use of a performance-importance plot (PIP) for the interpretation of the 25 items of the BDSQ.
ResultsOlder donors are more likely to report lower overall satisfaction with the service provided by the blood bank. PIP allows us to classify the items of BDSQ into long- and short-term improvement opportunities as well as into motivational and hygiene factors. Motivational factors (i.e. attributes that promote overall satisfaction when present) tend to be associated with the treatment offered by the blood bank staff. Donors seem to give more importance to the interpersonal aspects than to the physical structure of the service and other aspects of convenience.
ConclusionsTop-box analysis and PIP proved to be efficient strategies to interpret the results of the BDSQ.
The whole blood donation rate (WBDR) is a usual indicator of the general availability of blood in a country. According to the World Health Organization, the WBDR (median) is 32.1 donations per 1000 people a year in high-income countries, 14.9 in upper middle-income countries, 7.8 in lower middle-income countries, and 4.6 in low-income countries.1 Based on the number of donations recorded in the whole country, the Brazilian Health Ministry estimated that the overall WBDR in 2017 was 18.1/1000 eligible population.2 In order to improve blood donations from eligible donors and thus avoid shortage of the blood supply, blood banks should develop effective recruitment and retention strategies for safe donors.
It is known that the blood donor experience has a high relevance in encouraging or discouraging people to donate again.3 In other words, an optimal management of blood donation helps eliminate barriers and promotes the repetition of donations, in addition to stimulating people to encourage others to donate. A recently published study showed that the donation experience can be investigated through different approaches, and the satisfaction with the donation process proved to be an important factor.4 In this way, blood services around the world have been investing heavily in the satisfaction of the donors.5
In the context of blood donors and blood banks, Trovão et al.6 defined satisfaction as being “positive perceptions or feelings that an individual forms or has about the blood bank services and its professional staff as a result of his or her involvement in the blood donation process”. One should note here that the concept of “satisfaction” does not equate to the definition of “self-satisfaction” as described by Tey et al.,7 to whom it means satisfaction with oneself for donating blood. A number of studies have8–10 argued that satisfaction is positively correlated with the intent to return for future donation. In addition, the monitoring of satisfaction can be a useful tool for quality improvement, given the known relations between satisfaction and perceived service quality.11,12
There are several studies in the literature proposing instruments to understand the satisfaction of donors with the blood donation facilities.13–16 Borges et al.17 introduced an 18-item questionnaire in Portuguese language, including three domains: accessibility/convenience, technical aspects and interpersonal aspects. The article by Trovão et al.6 present some important shortcomings of this instrument. The major flaw is that the questionnaire does not directly measure the satisfaction with the service, since the response categories range from “totally right” to “totally wrong” for statements such as “It's easy to get to the blood bank” and “The blood bank is a clean place”. Therefore, it is dubious if the questionnaire actually captures satisfaction or service quality from the blood donor's perspective. In addition, the instrument by Borges et al.17 has never been formally validated by psychometric testing.
In this way, Trovão et al.6 introduced a new instrument in Brazilian Portuguese language capable of assessing the satisfaction of blood donors regarding their stay in blood banks, namely, the Blood Donor Satisfaction Questionnaire (BDSQ). The 25-item BDSQ is a modification of the instrument by Borges et al.17 and considers the following premises: (a) it is self-administered so that no blood bank staff members are required to collect information or leave their routine work; (b) the items included in the instrument are not intended to generate an “overall measurement” of the donor satisfaction, but rather to allow for a better knowledge of the attributes of satisfaction so that blood donors can be better served; and (c) the items in the instrument should refer to quality attributes that can be appropriately modified whenever needed. The article by Trovão et al.6 included a content validation to assess the relevance of the items of BDSQ, including clarity, domain structure and comprehensiveness of the satisfaction measurement.
In the present study, we have presented a proposal for application and interpretation of BDSQ, considering a sample of people who donate blood in a Brazilian blood bank.
MethodsSettingsData collection was carried out at the Regional Hemotherapy Center of Franca, a city of approximately 300,000 inhabitants, located in the southern state of São Paulo. In 2017, 12,814 blood donations were made by donors who had visited this facility.
ProceduresAll the people who donated blood between January 2017 and April 2017 were invited to participate in this study. The only eligibility criterion was to have completed the blood donation, but illiterate and visually impaired people were not included as the questionnaire was developed to be self-administered. The BDSQ was anonymously filled out by the donors at the cafeteria in the blood center after the blood collection was over. Written informed consent was obtained from all patients.
This BDSQ also includes a question about the overall satisfaction with the service provided by the blood bank, followed by 25 items (see Table 1) to be scored based on a 5-point scale and whose response categories are ordered from “very satisfied” to “very dissatisfied”. The scales include emoticons to help express the perceptions about the satisfaction.6,18 It is important that the overall satisfaction scale is entered before the 25 items to avoid possible biases in the overall perception of satisfaction. The questionnaire also includes questions on general characteristics of the respondents, such as gender, age, number of previous donations, reason for current blood donation and time taken to get to the blood bank. The full version of the questionnaire is available from the original paper.6
The 25 items of the BDSQ.
| 1. Facility to reach the blood donation center |
| 2. Reception service provided by the staff |
| 3. Care provided by the professional in the pre-screening step (who measured my blood pressure before the interview) |
| 4. Time I had to wait to be called for interview (after pre-screening) |
| 5. Kindness of the interviewer before blood donation (pre-screening time) |
| 6. Comfort of the room where I have been waiting to be called to donate blood |
| 7. Cleaning of the room where I have been waiting to be called to collect blood |
| 8. Time I had to wait until being called to enter the blood collection room |
| 9. Kindness of the professional who collected my blood |
| 10. Safety the blood bank conveys to me regarding the material used for blood collection and tests |
| 11. Care I feel I am receiving during blood donation |
| 12. Hygiene of the blood collection room |
| 13. Attention the professional who collects blood has during the procedure |
| 14. Comfort of the blood collection room |
| 15. Cleaning of the cafeteria (where they serve the snack) |
| 16. Explanations the professionals give to me regarding everything I want to understand |
| 17. Snack offered after blood donation |
| 18. Number of professionals available to assist me |
| 19. Professional competence of the staff in the blood bank |
| 20. Service provided by the person working in the cafeteria |
| 21. The whole time I spent in the blood center, from the reception to the end of blood donation |
| 22. Availability of professionals to listen to me at any time |
| 23. Blood bank service hours dedicated to the blood donor |
| 24. Effort of the professionals to make me feel at ease |
| 25. Respect with which people treat me in the blood bank |
The study protocol was approved by the Human Research Ethics Committee of the Ribeirão Preto Medical School at the University of São Paulo, under protocol number 1.845.298.
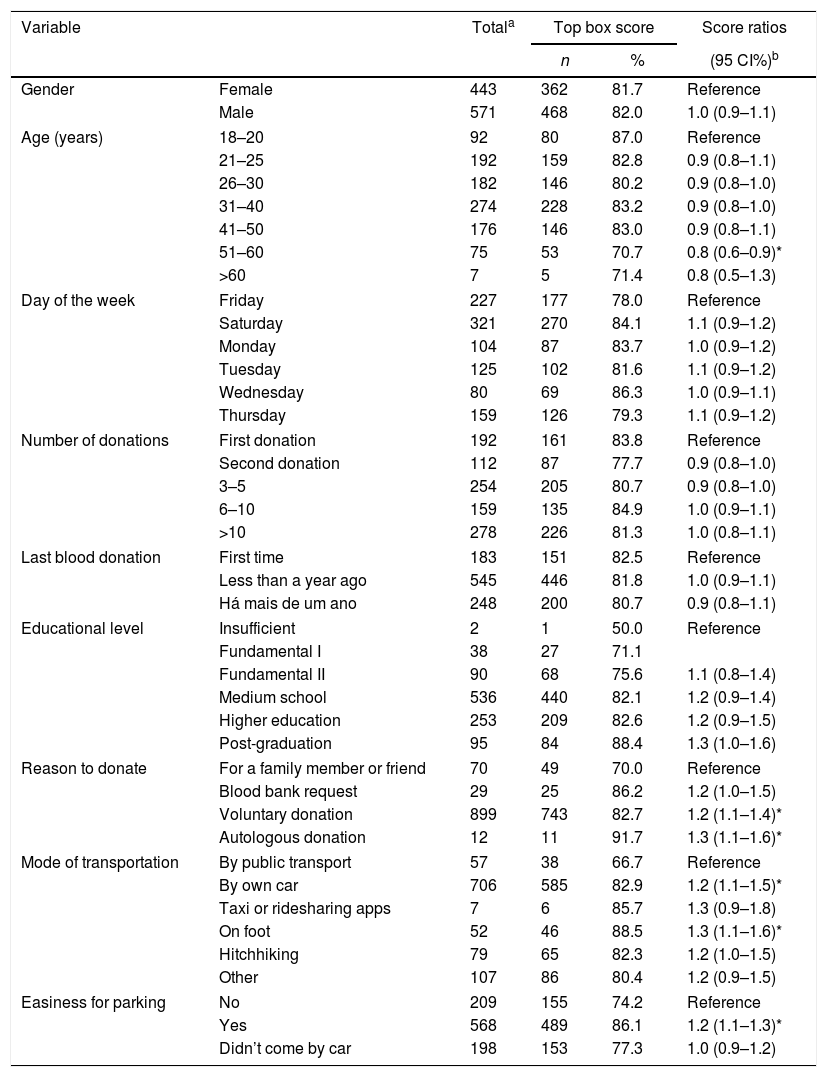
Statistical analysisThe top-box score is defined as the percentage of respondents who gave the highest (top) score on the question about overall satisfaction. A top-box analysis was used to assess the associations between variables that characterize the blood donor profile and a dummy variable equal to 1, if the donor had declared to be fully satisfied with the service provided by the blood bank, or 0 otherwise. Score ratios were obtained by comparing the top-box scores for the categories of each variable of interest, whereas the correspondent 95% confidence intervals (CI) were calculated similarly to that for prevalence ratios.19
A performance-importance plot (PIP) helped the interpretation of the 25 items of the BDSQ. PIP is a scatter plot between the performance of each item and the corresponding association with the overall satisfaction. The performance of each item was measured by using the arithmetic mean of the corresponding answers (considering 1=very satisfied, 2=satisfied, 3=neither satisfied nor dissatisfied, 4=dissatisfied, 5=very dissatisfied), with its importance being given by calculating the polychoric correlation coefficient between the corresponding item and overall satisfaction. Polychoric correlation was used because the scale items are ordinal variables.20 By using the mean values of correlation coefficients and performance measures as threshold values, the items of BDSQ are distributed into four quadrants, and their interpretation is described in Figure 1. The classification of the items as motivational and hygiene factors is based on the Herzberg's theory, which assessed job satisfaction.21,22 According to this theory, motivating factors (also called satisfiers) are elements that lead to satisfaction, whereas hygiene factors could prevent dissatisfaction. However, they could not serve as sources of satisfaction. In other words, hygiene factors do not motivate donors to be more satisfied, but they will make them feel dissatisfied if not present. As Herzberg has stated, the opposite of satisfaction is not dissatisfaction, but no satisfaction.23 Consequently, we understand that blood donors are satisfied by one set of factors and dissatisfied by another, meaning that PIP is a tool that helps us to identify these factors.
.")
All statistical analyses were conducted with R software, version 3.6.0.
ResultsThe refusal rate was approximately 20%, and the mean age of the 1019 participants included in the final sample was 33.5 years (standard deviation of 10.9). The top-box score was estimated at 81.8%. Table 2 shows the top-box analysis, where it is possible to observe that older donors are more likely to report lower overall satisfaction with the service provided by the blood bank. In addition, voluntary and autologous donors are more likely to be more satisfied than those who are donating blood at the request of a friend or family member. Public transport users also tend to report low satisfaction, as well as donors who had difficulty finding parking spaces. Donors who rely on public transport spent an average of 50minutes to reach the blood bank, whereas those who have a car spent only 17.7minutes.
Top box analysis.
| Variable | Totala | Top box score | Score ratios | ||
|---|---|---|---|---|---|
| n | % | (95 CI%)b | |||
| Gender | Female | 443 | 362 | 81.7 | Reference |
| Male | 571 | 468 | 82.0 | 1.0 (0.9–1.1) | |
| Age (years) | 18–20 | 92 | 80 | 87.0 | Reference |
| 21–25 | 192 | 159 | 82.8 | 0.9 (0.8–1.1) | |
| 26–30 | 182 | 146 | 80.2 | 0.9 (0.8–1.0) | |
| 31–40 | 274 | 228 | 83.2 | 0.9 (0.8–1.0) | |
| 41–50 | 176 | 146 | 83.0 | 0.9 (0.8–1.1) | |
| 51–60 | 75 | 53 | 70.7 | 0.8 (0.6–0.9)* | |
| >60 | 7 | 5 | 71.4 | 0.8 (0.5–1.3) | |
| Day of the week | Friday | 227 | 177 | 78.0 | Reference |
| Saturday | 321 | 270 | 84.1 | 1.1 (0.9–1.2) | |
| Monday | 104 | 87 | 83.7 | 1.0 (0.9–1.2) | |
| Tuesday | 125 | 102 | 81.6 | 1.1 (0.9–1.2) | |
| Wednesday | 80 | 69 | 86.3 | 1.0 (0.9–1.1) | |
| Thursday | 159 | 126 | 79.3 | 1.1 (0.9–1.2) | |
| Number of donations | First donation | 192 | 161 | 83.8 | Reference |
| Second donation | 112 | 87 | 77.7 | 0.9 (0.8–1.0) | |
| 3–5 | 254 | 205 | 80.7 | 0.9 (0.8–1.0) | |
| 6–10 | 159 | 135 | 84.9 | 1.0 (0.9–1.1) | |
| >10 | 278 | 226 | 81.3 | 1.0 (0.8–1.1) | |
| Last blood donation | First time | 183 | 151 | 82.5 | Reference |
| Less than a year ago | 545 | 446 | 81.8 | 1.0 (0.9–1.1) | |
| Há mais de um ano | 248 | 200 | 80.7 | 0.9 (0.8–1.1) | |
| Educational level | Insufficient | 2 | 1 | 50.0 | Reference |
| Fundamental I | 38 | 27 | 71.1 | ||
| Fundamental II | 90 | 68 | 75.6 | 1.1 (0.8–1.4) | |
| Medium school | 536 | 440 | 82.1 | 1.2 (0.9–1.4) | |
| Higher education | 253 | 209 | 82.6 | 1.2 (0.9–1.5) | |
| Post-graduation | 95 | 84 | 88.4 | 1.3 (1.0–1.6) | |
| Reason to donate | For a family member or friend | 70 | 49 | 70.0 | Reference |
| Blood bank request | 29 | 25 | 86.2 | 1.2 (1.0–1.5) | |
| Voluntary donation | 899 | 743 | 82.7 | 1.2 (1.1–1.4)* | |
| Autologous donation | 12 | 11 | 91.7 | 1.3 (1.1–1.6)* | |
| Mode of transportation | By public transport | 57 | 38 | 66.7 | Reference |
| By own car | 706 | 585 | 82.9 | 1.2 (1.1–1.5)* | |
| Taxi or ridesharing apps | 7 | 6 | 85.7 | 1.3 (0.9–1.8) | |
| On foot | 52 | 46 | 88.5 | 1.3 (1.1–1.6)* | |
| Hitchhiking | 79 | 65 | 82.3 | 1.2 (1.0–1.5) | |
| Other | 107 | 86 | 80.4 | 1.2 (0.9–1.5) | |
| Easiness for parking | No | 209 | 155 | 74.2 | Reference |
| Yes | 568 | 489 | 86.1 | 1.2 (1.1–1.3)* | |
| Didn’t come by car | 198 | 153 | 77.3 | 1.0 (0.9–1.2) | |
Figure 2 shows the PIP for the 25 items of the BDSQ. The green quadrant (low satisfaction, high importance) contains the following items:
- •
5. Kindness of the interviewer before blood donation,
- •
2. Reception service provided by the staff,
- •
21. The whole time the donor spent in the blood center, i.e. from reception to the end of blood donation, and
- •
18. Number of professionals available to assist the donor.
 for the 25 items of the BDSQ.")
In this order of importance, these items are priority for quality improvement in the Regional Hemotherapy Center of Franca, which consequently improves donor recruitment and retention. They represent short-term improvement opportunities, that is, they are attributes that, if improved, increase the overall satisfaction.
The yellow quadrant (high satisfaction, high importance) identifies the motivational factors. These items produce positive effects and the blood bank requires efforts to maintain them. In order of importance, they are the following:
- •
25. Respect with which people treat the blood donor in the blood bank,
- •
9. Kindness of the professional who collected blood,
- •
19. Professional competence of the staff in the blood bank,
- •
24. Effort of the professionals to make the blood donor feel at ease,
- •
3. Care provided by the professional in the pre-screening step,
- •
20. Service provided by the person working in the cafeteria,
- •
13. Attention of the professionals during blood collection procedure, and
- •
16. Explanations the professionals give to the donor regarding everything he/she wants to know.
The blue quadrant in Figure 2 (high satisfaction, low importance) shows the hygiene factors, that is, the attributes that apparently are not associated with overall satisfaction but which may make the donors feel dissatisfied if the blood bank fails to maintain them. These items are the following:
- •
15. Cleaning of the cafeteria,
- •
17. Snack offered after blood donation,
- •
22. Availability of professionals to listen to the donor at any time,
- •
10. Safety the blood bank conveys to the donor regarding the material used for blood collection and tests,
- •
12. Hygiene of the blood collection room,
- •
11. Care the donor feels during blood donation,
- •
14. Comfort of the blood collection room, and
- •
7. Cleaning of the room where the donor waits to be called to collect blood.
The red quadrant (low satisfaction, low importance) describes the long-term improvement opportunities:
- •
4. Time the donor waits to be called for interview,
- •
6. Comfort of the room where the donor waits to be called to donate blood,
- •
8. Time the donor waits until being called to enter the blood collection room,
- •
1. Facility to reach the blood donation center, and
- •
23. Service hours dedicated to the blood donor.
Blood donation is voluntary and non-remunerated in Brazil and other countries, meaning that the provision of blood products depends entirely on the willingness of donors to give their blood.24 Thus, strategies to retain donors are essential for blood banks to ensure a safe blood supply as donor satisfaction is an important factor in recruitment and retention programs, being positively correlated with the intent to return.25 The study by Fardin et al.26 showed that service quality affects the perceived value and satisfaction of blood donors. In addition, communication and human skills of the professionals and their technical skills also increase the satisfaction of blood donors with the service. In this way, the BDSQ was developed as a useful instrument to assess the satisfaction of the blood donor, including aspects related to accessibility, convenience, technical aspects and interpersonal aspects.6 When BDSQ was used in the Regional Hemotherapy Center of Franca, it was possible to identify in the yellow quadrant (high satisfaction, high importance) items on the relationship between donor and staff members, whereas in the red quadrant (low satisfaction, low importance) items on convenience aspects (Figure 2). This suggests that blood donors have higher expectations on the good treatment offered by the professionals than on the physical structure of the service or other aspects. Melián-Alsola and Martín-Santana4 compared the “moment of trust”, known in the literature as a company's interaction with the clients, with the donor's experience in the donation chain. Therefore, the authors suggest that donors can have several attitudes regarding the blood donation process, which in turn can influence their degree of satisfaction and their future behavioral intentions about blood donation. In this sense, the application of BDSQ showed the importance of providing ongoing training to the staff members so that they can offer a welcoming reception to donors, including aspects of humanization and empathy.
The present article proposes that top-box analysis and PIP are objective tools to interpret the results of BDSQ. Borges et al.6 proposed the use of correspondence analysis to measure the degree of satisfaction with each item of the instrument presented in their article. However, the correspondence analysis should be applied by using analytical software and this can be a difficult task without statistical assistance. On the other hand, top-box analysis and PIP are simpler and can be performed without difficulty. We used polychoric correlation coefficients as measures of importance in the present article, but Pearson's or Spearman's coefficients can be used for reasonable approximations.
It should be noted that although one can interpret the top-box score as a global index of satisfaction, any composition of the 25 items included in the BDSQ is not recommended for this purpose. Longitudinal comparisons between indexes based on the items instead on the top-box score may be a bad idea for a number of reasons. First, if we use the same instrument over two or more successive periods, an increase in the resulting index may not mean that blood donors are getting more satisfied, since the potential causes of dissatisfaction may change over time. Second, a satisfaction survey that results in an overall percentage of satisfaction close to 100% is not showing that almost all blood donors are satisfied with the service, but indicating that the instrument is not able to capture all sources of non-conformities. Carr-Hill27 argued that human satisfaction is a complex concept related to a number of factors, and many applied health service researchers carry out satisfaction surveys without considering the complexity of the task. In addition, Williams28 claimed that people “may have a complex set of important and relevant beliefs which cannot be embodied in terms of expressions of satisfaction”, suggesting that studies should first be conducted to identify how patients perceive and evaluate the service. Therefore, it is reasonable to understand that no instrument can measure the blood donor's satisfaction in its entirety, and the use of BDSQ does not exclude the use of complementary strategies, such as suggestion and complaints boxes placed in strategic locations.
For application of BDSQ in a blood bank, the following recommendations can be made:
- 1.
A time period for application of the BDSQ should be specified (e.g. in a given year due to the possibility of some seasonal variation in view of events that may have an effect on the donor's satisfaction).
- 2.
In parallel to the use of BDSQ, it is important to make a suggestion and complaint box available to the donors so that they can provide, at the end of the blood donation, other positive and negative perceptions about the service provided.
- 3.
At the end of data collection, data should be tabulated to generate the PIP of the attributes of satisfaction and sources of non-conformities for policies aimed at improving the quality of the service provided.
- 4.
At this moment, focus groups with blood donors can provide new information on attributes of satisfaction from their perspective. The information from the focus groups and suggestion and complaint box should be used to propose new items that can be added to the BDSQ, but without producing a very extensive questionnaire.
- 5.
Items that appear systematically in the yellow quadrant of PIP (high satisfaction, high importance) in successive applications of BDSQ may be replaced with new items, provided that the blood bank has ongoing strategies for maintaining the quality of the corresponding attributes. It is also important to avoid that the number of items in the instrument does not increase, which would impairs its parsimony. However, it is important to remember that in successive data collections, any item in PIP can move from one quadrant to another, and thus, an item listed in the yellow quadrant should not be deleted without ensuring the continued quality of its offer.
- 6.
At the end of this cycle, once the instrument has been adapted, this process should be repeated.
Although in the present study we distributed printed questionnaires to the blood donors, the use of electronic resources, in particular tablets, is a more practical and low-cost way of collecting data. REDCap electronic data capture software,29 for example, avoids further delay and typo errors caused by manual data entry, in addition to allowing real-time monitoring of the blood donor's satisfaction.
As a potential limitation of the instrument, it is important to question whether the results are subject to a halo effect, that is, a positive perception of some aspect that the donor values would make all attributes equally satisfactory, even if there is poor conformity. In fact, it was observed that 31.2% of the donors rated all 25 items of the instrument as very satisfactory. In addition, and perhaps less apparent, a horn effect may also be present when a donor experiences an unpleasant event at an early stage of the donation process (e.g. difficulty finding parking spaces or bad impression of the reception) and then he/she has a negative view of the other items. The relatively short period of data collection (only four months) can also be a limitation because events that may have an effect on the donor's satisfaction are possibly subject to some seasonal variation, as already discussed. Since this was the first time that the BDSQ was experimentally used in a blood bank, we were not allowed to collect data over a longer period of time. Another limitation is that approximately 20% of the blood donors refused to participate in the survey. Many non-respondents were unwilling to participate because they reported they felt tired after the entire donation process and others reported they were in a hurry to return to their jobs or homes. However, we believe that this relatively high non-response rate is expected in the practical application of questionnaires on satisfaction after a non-remunerated blood donation.
Conflicts of interestThe authors declare no conflicts of interest.



