

To demonstrate the proportion of anemia and its association with demographic and clinical characteristics in a representative sample of elderly people from São José dos Campos, São Paulo.
MethodsDemographic data and blood samples were collected from 398 over 65-year-old male and female individuals. Anemia was defined as hemoglobin concentration <12g/dL in women and <13g/dL in men. Anemic and non-anemic groups were compared using the chi-squared test and a multiple logistic regression model.
ResultsThe prevalence of anemia was 18.6% (20.8% in men and 17.6% in women). The percentages of anemia rose significantly across the age groups >75–80, >85–90 and >90–95 years (p-value=0.0251). There were no significant differences in gender, ethnic background, place of residence, years of schooling, income, comorbidities and use of medications. According to gender, the mean hemoglobin concentration and mean corpuscular volume were 11.5g/dL (range: 8.4–11.9g/dL) and 90.7fL (range: 63.0–111.7fL) for women and 11.9g/dL (range: 8.6–12.8g/dL) and 92.1fL (range: 59.8–100.1fL) for men. The great majority of anemia cases were mild with less than 6% having hemoglobin concentrations below 10.9g/dL. Mean corpuscular volume was lower than 80fL in six cases (8%), between 80 and 100fL in 65 cases (88%) and higher than 100fL in three cases (4%).
ConclusionA total of 18.6% of elderly people from São José dos Campos had mild anemia with the majority being normocytic. The percentages of anemia rose as the age increased demonstrating an association between age and anemia.
It has been demonstrated that anemia among older people is associated with a variety of adverse outcomes, including mortality.1,2 Estimates of the prevalence of anemia in elderly populations depend on demographic aspects, location and the health status of the individuals.3
In Brazil there are few studies in this field of research. To the best of our knowledge the prevalence of anemia was well documented in elderly individuals from only two urban regions located in the northeastern4 and southern regions.5
Considering the impact of anemia on the aged and the paucity of comparative data in Brazil, it seems that additional studies from different regions are needed. The population of São José dos Campos, the largest city in the Vale do Paraíba (State of São Paulo), is aging because of lower birth rates as demonstrated by the evolutionary analysis of its population pyramid.6 Therefore, the objectives of this study were to analyze the prevalence of anemia and its association with demographic characteristics in a sample of elderly people from São José dos Campos, southeastern Brazil.
MethodsThis study was carried out at the Centro de Hematologia do Vale (CHV) and the Hospital Pio XII in São José dos Campos. The study was approved by the Research Ethics Committee of the Universidade Paulista (# 481190) and all participants signed written consent forms. According to Brazilian Institute of Geography and Statistics (IBGE, 2010)7 the estimated numbers of elderly residents were 19,619 females and 17,810 males aged from 60 to 69 years and 14,416 females and 10,061 males older than 70 years. A sample size of 398 was calculated based on an estimated prevalence of anemia in older people of 20%, a 95% confidence interval and a sample error of 5%. The inclusion criteria of the study were over 65-year-old individuals, both males and females, who had not been transfused with red blood cells within the previous 12 weeks. A questionnaire was developed by the CHV regarding demographic and clinical aspects. People were invited to participate in the study through the local media including newspapers, television and social networks. One-day events were organized in central community meeting points of all six urban areas of São José dos Campos (north, east, center, southeast, south and west); in these places students, physicians and health professionals randomly applied the questionnaire to elderly local residents. In a second phase, the participants were invited to give blood samples in two clinical biochemistry laboratories in the Hospital Pio XII. Overall, 713 people were interviewed and 415 (58.2%) gave blood samples. The samples were obtained from the median cubital vein using an evacuated tube system. Volunteers who did not answer the questionnaire or from whom an inadequate blood sample was collected were excluded from the study. The final study sample included 398 elderly people interviewed between May 2012 and November 2013. The World Health Organization (WHO) criteria were used to define anemia (hemoglobin concentration <12g/dL in women and <13g/dL in men) and assess severity.8 Anemic and non-anemic groups were compared using the chi-squared test and a multiple logistic regression model; p-values of less than 0.05 were considered significant.
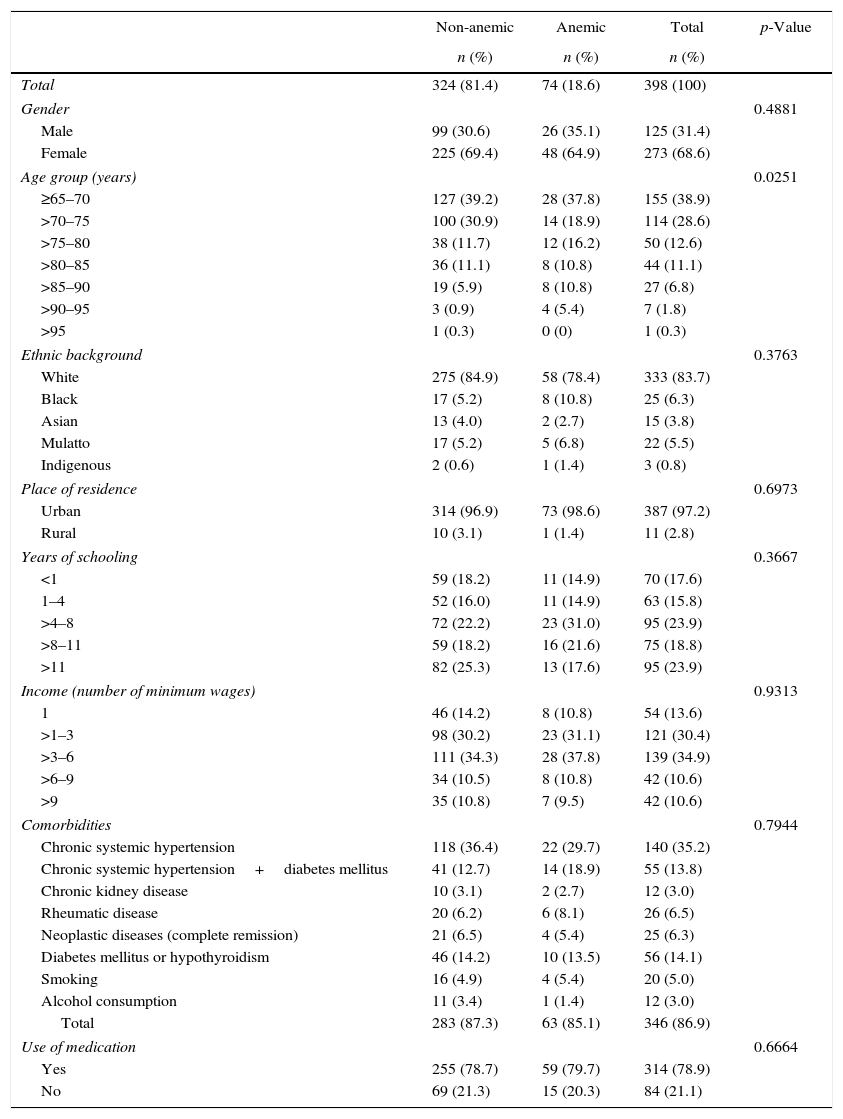
ResultsThe prevalence of anemia in this sample was 18.6% (20.8% in men and 17.6% in women). The percentages of anemia rose significantly across the age groups >75–80, >85–90 and >90–95 years (p-value=0.0251). No significant differences were observed for the other variables analyzed in this study (gender, ethnic background, place of residence, years of schooling, income, comorbidities and use of medications – Table 1).
Demographic and clinical characteristics of non-anemic and anemic individuals.
| Non-anemic | Anemic | Total | p-Value | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Total | 324 (81.4) | 74 (18.6) | 398 (100) | |
| Gender | 0.4881 | |||
| Male | 99 (30.6) | 26 (35.1) | 125 (31.4) | |
| Female | 225 (69.4) | 48 (64.9) | 273 (68.6) | |
| Age group (years) | 0.0251 | |||
| ≥65–70 | 127 (39.2) | 28 (37.8) | 155 (38.9) | |
| >70–75 | 100 (30.9) | 14 (18.9) | 114 (28.6) | |
| >75–80 | 38 (11.7) | 12 (16.2) | 50 (12.6) | |
| >80–85 | 36 (11.1) | 8 (10.8) | 44 (11.1) | |
| >85–90 | 19 (5.9) | 8 (10.8) | 27 (6.8) | |
| >90–95 | 3 (0.9) | 4 (5.4) | 7 (1.8) | |
| >95 | 1 (0.3) | 0 (0) | 1 (0.3) | |
| Ethnic background | 0.3763 | |||
| White | 275 (84.9) | 58 (78.4) | 333 (83.7) | |
| Black | 17 (5.2) | 8 (10.8) | 25 (6.3) | |
| Asian | 13 (4.0) | 2 (2.7) | 15 (3.8) | |
| Mulatto | 17 (5.2) | 5 (6.8) | 22 (5.5) | |
| Indigenous | 2 (0.6) | 1 (1.4) | 3 (0.8) | |
| Place of residence | 0.6973 | |||
| Urban | 314 (96.9) | 73 (98.6) | 387 (97.2) | |
| Rural | 10 (3.1) | 1 (1.4) | 11 (2.8) | |
| Years of schooling | 0.3667 | |||
| <1 | 59 (18.2) | 11 (14.9) | 70 (17.6) | |
| 1–4 | 52 (16.0) | 11 (14.9) | 63 (15.8) | |
| >4–8 | 72 (22.2) | 23 (31.0) | 95 (23.9) | |
| >8–11 | 59 (18.2) | 16 (21.6) | 75 (18.8) | |
| >11 | 82 (25.3) | 13 (17.6) | 95 (23.9) | |
| Income (number of minimum wages) | 0.9313 | |||
| 1 | 46 (14.2) | 8 (10.8) | 54 (13.6) | |
| >1–3 | 98 (30.2) | 23 (31.1) | 121 (30.4) | |
| >3–6 | 111 (34.3) | 28 (37.8) | 139 (34.9) | |
| >6–9 | 34 (10.5) | 8 (10.8) | 42 (10.6) | |
| >9 | 35 (10.8) | 7 (9.5) | 42 (10.6) | |
| Comorbidities | 0.7944 | |||
| Chronic systemic hypertension | 118 (36.4) | 22 (29.7) | 140 (35.2) | |
| Chronic systemic hypertension+diabetes mellitus | 41 (12.7) | 14 (18.9) | 55 (13.8) | |
| Chronic kidney disease | 10 (3.1) | 2 (2.7) | 12 (3.0) | |
| Rheumatic disease | 20 (6.2) | 6 (8.1) | 26 (6.5) | |
| Neoplastic diseases (complete remission) | 21 (6.5) | 4 (5.4) | 25 (6.3) | |
| Diabetes mellitus or hypothyroidism | 46 (14.2) | 10 (13.5) | 56 (14.1) | |
| Smoking | 16 (4.9) | 4 (5.4) | 20 (5.0) | |
| Alcohol consumption | 11 (3.4) | 1 (1.4) | 12 (3.0) | |
| Total | 283 (87.3) | 63 (85.1) | 346 (86.9) | |
| Use of medication | 0.6664 | |||
| Yes | 255 (78.7) | 59 (79.7) | 314 (78.9) | |
| No | 69 (21.3) | 15 (20.3) | 84 (21.1) | |
Hemoglobin concentration and mean corpuscular volume (MCV) of the anemic group according to gender are shown in Table 2. Overall, the great majority of anemia cases were mild with less than 6% having hemoglobin concentrations below 10.9g/dL. The MCV was lower than 80fL in six cases (8%), between 80 and 100fL in 65 cases (88%) and higher than 100fL in three cases (4%).
Hemoglobin concentration (Hb) and mean corpuscular volume (MCV) according to gender for the anemic group.
| n | % | Hb (g/dL) | MCV (fL) | |
|---|---|---|---|---|
| Male | 26 | 20.8 | 11.9 (8.6–12.8) | 92.1 (59.8–100.1) |
| Female | 48 | 17.6 | 11.5 (8.4–11.9) | 90.7 (63.0–111.7) |
| Total | 74 | 18.6 | 11.6 (8.4–12.8) | 91.1 (59.8–111.7) |
Data are expressed as median and range.
This study has limitations. It was carried out based on cross-sectional data, and therefore, no cause–effect relationship could be established. This is only a descriptive study that reports the proportion and severity of anemia in general.
The overall prevalence of anemia in this series was 18.6% with a significant association being demonstrated between age and anemia. In a prospective population-based study of all over 64-year-old residents in Biella (Italy), anemia was found in 11.8% with the prevalence and incidence of anemia increasing with age.9 In a study performed in Germany, the prevalence of anemia of participants aged 65 or older was 4.3% again with the incidence increasing with age.10 A prospective study conducted in elderly Koreans demonstrated that the overall prevalence of anemia was 13.6% and a significant association was observed with age.11 Data from the United States population assessed in the Third National Health and Nutrition Examination Survey (NHANES III) identified anemia in 10.6% of people aged 65 years and older; anemia increased with age reaching the highest prevalence in the 85 years and older age group.12 On the other hand, data from low and middle-income countries are sparse. Bryce et al.13 surveyed 10,915 people aged 65 years and over in catchment areas in Cuba, Dominican Republic, Puerto Rico, Venezuela and Mexico and found anemia prevalence rates of 19.2%, 37.3%, 32.1%, 9.8% and 9.2% respectively; in all these countries anemia increased with age. In a population-based study performed among 392 free-living elderly in south Brazil, the overall prevalence of anemia was 12.8% and this increased with age.5 Moreover, a cross-sectional study carried out in Camaragibe (northeastern Brazil) involving 284 subjects aged 60 years and over showed that the prevalence of anemia was around 11%.4
Data regarding the proportion of anemia in men and women and the relationship between anemia and ethnic background have also been described.3,12 Although females predominated in this study, a higher occurrence of anemia was observed in older men confirming results previously reported3,10,12–14 but different to two studies performed in different regions of Brazil by Barbosa et al.4 and Sgnaolin et al.5 This study found no association with regard to ethnic background; the ethnic background of patients was to some extent biased due to the subjectivity of the question. This variable was studied according to the definition of each patient without any interference of the health professional who applied the questionnaire. Thus, some patients reported being white rather than mulatto but this phenomenon was not clearly observed for Black and Asian classifications.
As described before, the lack of association for the place of residence, years of schooling, income and anemia suggests that socioeconomic aspects did not play a role in the current sample.3,12,13
With regard to the cause of anemia, the data of this study suggest a high proportion of people with unexplained anemia.12,15 There are some reasons that support this hypothesis. Most people had mild and normocytic anemia (88%) in contrast to low proportions of both microcytic and macrocytic anemia. Moreover, blood smears from people with high MCVs showed a normal appearance of white cells. These findings suggest that the occurrence of anemia may not be associated with iron, folate or vitamin B12 deficiencies. In addition, considering the similar percentages of chronic systemic hypertension, diabetes mellitus, rheumatic diseases and kidney diseases between anemic and non-anemic groups, it is reasonable to believe that the anemia could not be attributed to chronic disease, inflammation or chronic kidney disease. Moreover, since the anemia in this series did not present with either low leukocyte or low platelet counts (data not shown), a concurrent association with myelodysplastic syndromes was not considered.14,16 In comparison, a revision of clinical, diagnostic and biological issues related to anemia and aging as reported by Carmel17 demonstrated a higher prevalence of mild normocytic anemia and smaller proportion of microcytic anemia; unexplained anemia accounted for 14–17% of the cases. Data from the NHANES III study3,12 indicated that most occurrences of anemia were mild and nutrient deficiency was observed in one-third, anemia of chronic disease was present in one-third and unexplained anemia was observed in one-third. The Italian study9 found a higher proportion of normocytic anemia and the underlying cause of mild anemia remained unexplained in 26.4% of the cases. A study performed in Germany10 showed that the majority of the anemia cases were mild with the following subtypes: microcytic anemia with iron deficiency (19%), anemia of chronic disease (25%) and unexplained anemia (44%). The study carried out in Camaragibe (northeastern Brazil)4 reported that the major characteristics of anemia were mild, with normochromia and normocytosis and a lower prevalence of microcytosis. In contrast, the occurrence of anemia in older people from southern Brazil was associated with microcytosis and hypochromia.5 Data from Cuba, Dominican Republic, Puerto Rico, Venezuela and Mexico demonstrated that most cases of anemia were associated with microcytosis and nutritional deficiency.13 Given that anemia is a multifactorial condition, a major problem with interpreting these reports is that they are extrapolated from local data from specific regions and thus most likely reflecting the characteristics of a particular population. To further investigate this matter, studies incorporating the measurement of serum biochemical markers such as iron, ferritin, folate, vitamin B12 and creatinine should be designed in this region.
ConclusionThis study demonstrates that 18.6% of a representative sample of community-dwelling elderly people from São José dos Campos, southeastern Brazil had mild anemia with the great majority being normocytic. The percentages of anemia rose across the highest age groups and an association between age and anemia was demonstrated. With regard to the prevalence of anemia in the elderly, this series was similar to Cuba but higher than developed countries and other regions of Brazil. Both the association between age and anemia and the substantial proportion of mild normocytic anemia of unexplained cause are similar to other studies.
Finally, considering the heterogeneity in the distribution of social and biological risk factors in Brazil, we believe that a national survey of the prevalence of anemia in the elderly may shed some light on this important issue. In addition, a long-term follow-up of the aged with mild and asymptomatic anemia may be important to establish whether anemia is a marker of a more severe underlying condition.
Conflicts of interestThe authors declare no conflicts of interest.

