


iron deficiency anemia is the most common type of nutritional anemia; it has been recognized as an important health problem in Palestine. This study was conducted to estimate the prevalence and to identify possible risk factors of iron deficiency anemia among kindergarten children living in the marginalized areas of the Gaza Strip and to evaluate the effectiveness of supplementing oral iron formula in the anemic children.
Methodsthe study included 735 (384 male and 351 female) kindergarten children. Data was collected by questionnaire interviews, anthropometric measurements, and complete blood count analysis. All iron deficient anemic children were treated using an oral iron formula (50mg ferrous carbonate+100mg vitamin C /5mL) and the complete blood count was reassessed after three months. A univariate analysis and a multiple logistic regression model were constructed; crude and adjusted odds ratios (OR), and 95% confidence intervals (95% CI) were calculated.
Resultsthe overall prevalence of iron deficiency anemia was 33.5% with no significant differences between boys and girls. Significantly different prevalences of iron deficiency anemia were reported between different governorates of the Gaza Strip. Governorate, low education level of the parents and smoking are significant risk factors for children developing anemia. Significantly lower complete blood count parameters, except for WBC, were reported in anemic children. The oral iron treatment significantly improved hemoglobin concentrations, and normalized the iron deficiency marker.
Conclusionsiron deficiency anemia is a serious health problem among children living in the marginalized areas of the Gaza Strip, which justifies the necessity for national intervention programs to improve the health status for the less fortunate development areas.
Anemia due to iron deficiency is the most common and widespread nutritional anemia in the world and significantly afflicts individuals of all ages and economic groups in both developing and developed countries. Iron deficiency and its associated anemia are more common among the very young, among those on poor diets, among people with intestinal parasitic diseases, and among women of childbearing age. The World Health Organization (WHO) estimates are staggering; almost one-third (more than 2 billion people) of the world’s population are anemic, most of which is due to iron deficiency.1,2
Although the prevalence of iron deficiency anemia (IDA) in industrialized countries has declined in recent decades, there has been little effect on in the global prevalence, which remains high and challenging. In developing countries, the WHO expects more troubling prevalences reporting that one in two pregnant women and about 40% of preschool children are likely to be anemic, many of them due to iron deficiency. This condition is intensified and exacerbated by parasites, malaria and other infectious diseases such as HIV and tuberculosis, especially in resource-poor and underdeveloped areas.3,4 In addition to nutritional and clinical factors, several studies associate socioeconomic factors, such as low parental education levels, low household incomes,5,6 and demographic factors including age, gender, and family size3,7 to the prevalence and worsening of anemia.
Poor pregnancy outcomes, maternal deaths, impaired physical and cognitive development, increased risk of morbidity in children and reduced work productivity in adults are major health concerns and clinical manifestations associated with anemia.8,10 As anemia worsens, multiple cardiovascular signs generally start to appear, beginning with tachycardia, palpitations, impaired ventricular performance, cardiomegaly, and sometimes cardiac arrhythmia and congestive heart failure. Furthermore, red blood cells of anemic subjects are more vulnerable to oxidation, concomitant to increased lipid peroxidation and diminished antioxidant defense and enzymes.11 On the national economical level, IDA lowers the work capacity, causing serious economic difficulties and obstacles to national development strategic plans.12-14
Treatment of iron deficiency is simple and inexpensive especially through the oral route, but may be hampered by some gastrointestinal inconveniences.15 Several compounds have been added to the standard iron formula in order to enhance iron absorption. Combinations of iron and vitamin C,16 vitamin A+zinc17 and taurine11 have been shown to be more effective in restoring hemoglobin levels than iron alone. We designed the present study to estimate the prevalence and possible risk factors of IDA among kindergarten children living in marginalized areas of the Gaza strip and to evaluate the effectiveness of supplementing oral iron formula to ameliorate anemia in these less fortunate IDA children.
MethodsThe present work was performed according to a quasi-experimental research design, which includes pre- and post-testing measurements within a treatment group, as well as comparisons between case and control groups for the variables studied.
Study areaThe Gaza Strip in Palestine is a narrow piece of land (365km2) along the East Mediterranean coast divided into five governorates: North, Gaza, Middle, Khan Yunis, and Rafah Governorates. It is considered one of the most populated areas in the world (4583 individuals/km2) with an estimated population of almost 1.7 million according to latest estimates of the Palestinian central bureau of statistics.18 Nine marginalized (less fortunate for development) areas representing the five governorates of the Gaza strip were involved in the present work. These marginalized areas were identified according to the criteria laid down by the Palestinian Medical Relief Society (PMRS). The studied population comprised all kindergarten children (4-5 years of age) living in the marginalized areas of the Gaza Strip. A total of 735 (384 male and 351 female) randomly selected children were included, they represented the 11 kindergartens located in the nine marginalized areas. A sample size of at least 398 children was calculated for a±5% precision level and a 95% confidence level. The sample size was determined based on the population of the marginalized area rather than the governorate population density.
All parts of the study were carried out in accordance to the ethical standards laid down in the 1964 and 1975 Declarations of Helsinki, and the modifications thereafter. All ethical considerations were kept, including respect for the subjects, legitimacy and confidentiality. A signed consent form was obtained from the parents or guardians providing their acceptance and full understanding of the study stages and intervention.
Study stagesThe study included three stages. The first stage was assigned to screening for IDA, the second stage was the intervention to correct anemia, and the last stage was the follow up and reevaluation of the treated children.
Part of the data was collected using a close-ended questionnaire, constructed in the Arabic language, and the data was collected through home visits and direct interviews with the parents or guardians. The questionnaire included major items about sociodemographic and general characteristics, as well as items about the health status and health complaints of the children as addressed by their parents or guardians.
Venous blood samples (2.5mL in K3-EDTA) were collected from the children, and a complete blood count (CBC) analysis was performed using a Cell Dyne 1700 electronic counter (Sequoia-Turner Corporation, Santa Clara, CA).
Diagnosis of iron deficiency anemiaIn the present work, and due to the limited financial and laboratory resources in the marginalized areas, IDA was considered in the microcytic (MCV<80fl) children using the Mentzer index MCV/RBC>1319,20 concomitant to reduced hemoglobin concentration<11g/dL for 4-year-old children, and<11.5g/dL for 5-year-old children.21 The prevalence of IDA was calculated by dividing the number of occurrences of IDA in the randomly selected children by the total number of children.
Replenishing the iron stores and correction of anemiaAll children considered as IDA were treated with oral iron supplements (Ferrolet syrup [50mg ferrous carbonate+100mg vitamin C /5mL]) for three months. The dose was calculated based on the child’s weight according to standard protocols.22
The iron treatment was under full supervision and guidance of pediatricians at the PMRS.
Post-treatment evaluationAll IDA children who had been treated with oral iron supplements were checked for the same parameters of CBC three months after start of the treatment.
Statistical analysisDescriptive, frequencies, central tendency, dispersion measurements, cross tabulation and statistical tests included independent and paired t-tests, chi-square, and correlations used to clarify relationships between the studied variables. The associations between anemia and the variables were tested using a simple univariate logistic regression and reported as crude odds ratios (OR) with 95% CI. Statistically predictive variables at the univariate analysis were included in the multiple logistic regression models to examine the risk factors that were potentially associated with anemia in the children living in marginalized areas. The results from the multiple logistic regressions are presented as adjusted odds ratio (aORs) with 95% CI. p-values were two sided and a p-value<0.05 was considered to indicate statistical significance. All analyses were performed using the IBM SPSS Statistical software (version 18, IBM Corporation, Somers, NY).
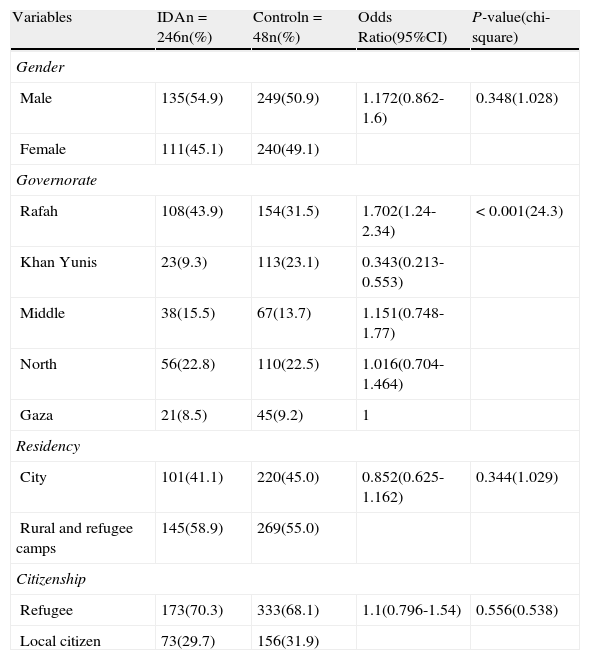
ResultsThe study was conducted on 735 children (384 male & 351 female) representing 11 kindergartens from nine marginalized areas of the five governorates of the Gaza strip. General characteristics of the study population are outlined in Table 1. The overall prevalence of IDA was 33.5% (246/735) with no significant difference (p-value=0.348) between boys 35.2% (135/384) and girls 31.6% (111/351). Significantly different prevalences of IDA were reported between different governorates, with the highest values reported in the Rafah (108/262; 41.2%) and Middle (38/105; 36.2%) Governorates. Also significantly higher prevalences (p-value=0.008) were reported among children residing in refugee camps (51/110; 46.4%) compared to rural (94/304; 30.9%) and urban (101/321; 31.5%) areas. Meanwhile, the citizenship status, citizen vs refugee, was not a significant risk factor for IDA (p-value=0.556; OR=1.1; 95% CI, 0.796-1.549).
General characteristics of the study population.
| Variables | IDAn=246n(%) | Controln=48n(%) | Odds Ratio(95%CI) | P-value(chi-square) |
| Gender | ||||
| Male | 135(54.9) | 249(50.9) | 1.172(0.862-1.6) | 0.348(1.028) |
| Female | 111(45.1) | 240(49.1) | ||
| Governorate | ||||
| Rafah | 108(43.9) | 154(31.5) | 1.702(1.24-2.34) | <0.001(24.3) |
| Khan Yunis | 23(9.3) | 113(23.1) | 0.343(0.213-0.553) | |
| Middle | 38(15.5) | 67(13.7) | 1.151(0.748-1.77) | |
| North | 56(22.8) | 110(22.5) | 1.016(0.704-1.464) | |
| Gaza | 21(8.5) | 45(9.2) | 1 | |
| Residency | ||||
| City | 101(41.1) | 220(45.0) | 0.852(0.625-1.162) | 0.344(1.029) |
| Rural and refugee camps | 145(58.9) | 269(55.0) | ||
| Citizenship | ||||
| Refugee | 173(70.3) | 333(68.1) | 1.1(0.796-1.54) | 0.556(0.538) |
| Local citizen | 73(29.7) | 156(31.9) | ||
IDA: iron deficiency anemia; 95% CI:95% confidence interval.
Some of the parents’ characteristics are presented in Table 2. The education of the father and mother were risk factors associated with children developing IDA [OR=0.624 (95% CI, 0.443-0.881) and OR=0.606 (95% CI, 0.424-0.866), respectively]. Parental smoking habit was a significant risk factor for IDA among children (OR=0.580; 95% CI, 0.425-0.790); the percentage of anemic children of smoking fathers (126/311; 40.5%) was significantly higher (p-value=0.001) than those of non-smoking fathers (120/424, 28.3%). While parents’ consanguinity was not found to be a risk factor for IDA (OR=0.798; 95% CI, 0.587-1.085), the percentage of anemic children of consanguineous parents (126/349, 36.1%) does not differ significantly (p-value=0.150) from those of non-consanguineous parents (120/266; 31.1%).
Some characteristics of the parents of the study population.
| Variables | IDAn(%) | Controln(%) | Odds Ratio(95%CI) | P-value(chi-square) |
| Father education | ||||
| University degree | 61(24.8) | 169(34.6) | 0.624(0.443-0.881) | 0.007(7.30) |
| Secondary school and below | 185(75.2) | 320(65.4) | ||
| Governorate | ||||
| University degree | 54(22.0) | 155(31.7) | 0.606(0.424-0.866) | 0.006(7.6) |
| Secondary school and below | 192(78.0) | 334(68.3) | ||
| Father smokinga | ||||
| Smoker | 126(51.2) | 185(37.8) | 0.580(0.425-0.790) | 0.001(12.0) |
| Non-smoker | 120(48.5) | 304(62.2) | ||
| Parents consanguinity | ||||
| Consanguineous | 126(51.0) | 223(45.6) | 0.798(0.587-1.085) | 0.150(2.07) |
| Non-Consanguineous | 120(48.8) | 266(54.4) | ||
IDA: iron deficiency anemia; 95% CI: 95% confidence interval
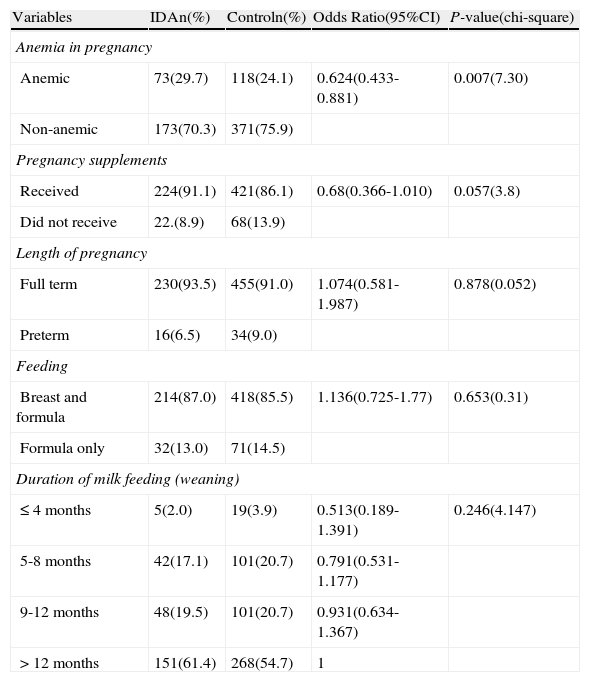
Either pregnancy, birth and lactation (Table 3), nor health (Table 4) characteristics of the children showed any significant association for developing IDA. However, there is a trend towards developing IDA with late weaning. IDA was more prevalent among children suffering from chronic or frequent diarrhea, and those suffering from parasitic infections, but these differences were not significant.
Pregnancy,birth and lactation characteristics.
| Variables | IDAn(%) | Controln(%) | Odds Ratio(95%CI) | P-value(chi-square) |
| Anemia in pregnancy | ||||
| Anemic | 73(29.7) | 118(24.1) | 0.624(0.433-0.881) | 0.007(7.30) |
| Non-anemic | 173(70.3) | 371(75.9) | ||
| Pregnancy supplements | ||||
| Received | 224(91.1) | 421(86.1) | 0.68(0.366-1.010) | 0.057(3.8) |
| Did not receive | 22.(8.9) | 68(13.9) | ||
| Length of pregnancy | ||||
| Full term | 230(93.5) | 455(91.0) | 1.074(0.581-1.987) | 0.878(0.052) |
| Preterm | 16(6.5) | 34(9.0) | ||
| Feeding | ||||
| Breast and formula | 214(87.0) | 418(85.5) | 1.136(0.725-1.77) | 0.653(0.31) |
| Formula only | 32(13.0) | 71(14.5) | ||
| Duration of milk feeding (weaning) | ||||
| ≤4months | 5(2.0) | 19(3.9) | 0.513(0.189-1.391) | 0.246(4.147) |
| 5-8 months | 42(17.1) | 101(20.7) | 0.791(0.531-1.177) | |
| 9-12 months | 48(19.5) | 101(20.7) | 0.931(0.634-1.367) | |
| >12months | 151(61.4) | 268(54.7) | 1 | |
IDA: iron deficiency anemia; 95% CI: 95% confidence interval.
Health characteristics of the children.
| Variables | IDAn=246n(%) | Controln=489n(%) | Odds Ratio(95%CI) | P-value(chi-square) |
| Child malnutritiona | 38(15.4) | 88(18.0) | 0.832(0.549-1.262) | 0.408(0.749) |
| Diarrhea (frequent or chronic) | 22(8.9) | 28(5.7) | 0.618(0.346-1.105) | 0.120(2.672) |
| Parasitic infections | 105(42.7) | 198(40.5) | 0.914(0.670-1.246) | 0.569(0.325) |
IDA: iron deficiency anemia; 95% CI: 95% confidence interval.
The anthropometric characteristics of the children revealed a lower weight and a shorter stature in the IDA group compared to normal controls (15.49±2.29 vs. 16.26±6.55kg and 103.61±5.42 vs. 105.01±5.14cm, respectively). Correlation coefficient analysis revealed a significant correlation between hemoglobin concentration and the child’s weight (p-value=0.039) and height (p-value=0.001) but not with age (p-value=0.06).
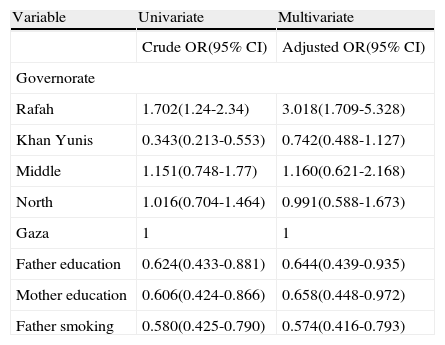
We performed a univariate statistical analysis to study the association between the various exposures, if any, with the anemic state (anemic versus non-anemic controls). In this unadjusted analysis, we calculated the crude ORs and their 95% CI, shown in Tables 1-4. In this analysis, the following factors: governorate, residency, parents’ education, and parental smoking showed significant associations with the anemic state. As a result, our multivariate analysis was adjusted to contain fewer potential risk factors. After adjustment of the potential confounding factors, we performed a multivariate statistical analysis in order to calculate the aOR and the 95% CI aiming to identify the possible risk factors associated to anemia in our cohort of Palestinian children living in the marginalized areas. The multiple logistic regression analysis for all cases and controls are presented in Table 5; this analysis highlighted governorate, parents’ education and parental smoking as potential risk factors for developing anemia in children living in the marginalized areas of the Gaza Strip.
Univariate (crude OR) multivariate (adjusted OR) analysis for risk factors associated with anemia.
| Variable | Univariate | Multivariate |
| Crude OR(95% CI) | Adjusted OR(95% CI) | |
| Governorate | ||
| Rafah | 1.702(1.24-2.34) | 3.018(1.709-5.328) |
| Khan Yunis | 0.343(0.213-0.553) | 0.742(0.488-1.127) |
| Middle | 1.151(0.748-1.77) | 1.160(0.621-2.168) |
| North | 1.016(0.704-1.464) | 0.991(0.588-1.673) |
| Gaza | 1 | 1 |
| Father education | 0.624(0.433-0.881) | 0.644(0.439-0.935) |
| Mother education | 0.606(0.424-0.866) | 0.658(0.448-0.972) |
| Father smoking | 0.580(0.425-0.790) | 0.574(0.416-0.793) |
OR: odds ratio; 95% CI: 95% confidence interval.
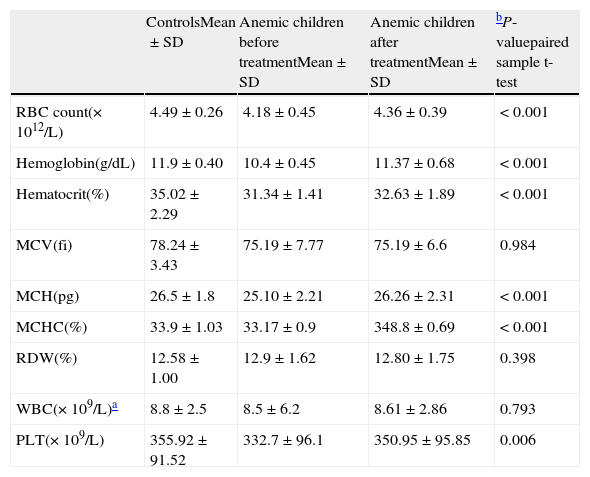
Hematological parameters (Table 6) revealed significantly lower CBC values, except for WBC, in IDA children compared to the non-anemic controls. The reduction in hemoglobin and hematocrit levels in the IDA cases were 12.6% and 10.5% compared to controls, but oral iron treatment significantly improved the situation and normalized the IDA markers. After iron treatment, hemoglobin (10.4±0.45 vs. 11.37±0.68g/dL) and hematocrit (31.34±1.41 vs. 32.63±1.89%) levels were 9.3% and 4.1% higher of the baseline values.
Hematological parameters of the study subjects
| ControlsMean±SD | Anemic children before treatmentMean±SD | Anemic children after treatmentMean±SD | bP-valuepaired sample t- test | |
| RBC count(×1012/L) | 4.49±0.26 | 4.18±0.45 | 4.36±0.39 | < 0.001 |
| Hemoglobin(g/dL) | 11.9±0.40 | 10.4±0.45 | 11.37±0.68 | < 0.001 |
| Hematocrit(%) | 35.02±2.29 | 31.34±1.41 | 32.63±1.89 | < 0.001 |
| MCV(fi) | 78.24±3.43 | 75.19±7.77 | 75.19±6.6 | 0.984 |
| MCH(pg) | 26.5±1.8 | 25.10±2.21 | 26.26±2.31 | < 0.001 |
| MCHC(%) | 33.9±1.03 | 33.17±0.9 | 348.8±0.69 | < 0.001 |
| RDW(%) | 12.58±1.00 | 12.9±1.62 | 12.80±1.75 | 0.398 |
| WBC(×109/L)a | 8.8±2.5 | 8.5±6.2 | 8.61±2.86 | 0.793 |
| PLT(×109/L) | 355.92±91.52 | 332.7±96.1 | 350.95±95.85 | 0.006 |
RBC: red blood cell;MCV: mean corpuscle volume;MCH: mean corpuscle;MCHC: mean corpuscular hemoglobin concentration;RDW: red cell distribution width;WBC, white blood cell;PLT: platelets;SD:standard deviation.
Nutritional deficiencies are very important to the overall health of humans, male and female of all ages, however in some age groups (infants, children, and women in childbearing age) these deficiencies can be critical and the growth and development will be extremely hindered by essential vitamins or nutrients scarcity. Iron deficiency (ID) and IDA are considered to be the most common and prevalent known nutritional disorder of mankind in the world today. Previous studies showed a considerable prevalence of iron deficiency anemia among Palestinians in the Gaza strip.11,23-25 ID and IDA not only constitute public health nutritional problems, but also their existence with other disorders could interfere with the laboratory and clinical diagnosis of the coexisting disorder.26
We designed the present study that included nine marginalized areas, distributed over the different governorates of Gaza Strip; these areas have attracted little attention from several local and international institutions. Since our target population was the children of the less fortunate marginalized areas, we considered the population in the area for the sampling process, and not the governorate size.
At the screening stage, the presence of IDA was considered in microcytic (MCV<80fl) children through the Mentzer index MCV/RBC>1319,20,27 with accompanying reduced hemoglobin concentration.21 The low financial resources and the lack of availability of instruments in the area could be considered as a limitation of the study, justify the use of the Mentzer index for the determination of serum ferritin, deemed essential for this screening. Moreover, the politically restrictive environment in the Gaza strip negatively affects importing medical and laboratory equipment, kits and chemicals to perform laboratory investigations.
The overall prevalence of IDA was 33.5 % with significantly higher prevalences in the Rafah and Middle governorates. Citizenship was not found to be a determinant of IDA, prevalence of IDA was not significantly different between citizens and refugees, concomitant to the national nutritional assessment study performed by Abdeen et al.23 However, residing in refugee camps is a significant determinant for anemia in our study population. Our results are comparable to the results of Selmi & Al Hindi who reported significantly different prevalences of anemic children between the different regions of the Gaza Strip, Palestine.23,24
Although, the overall educational background of the children’s parents revealed a satisfactory level, low education was a significant risk factor associated with IDA in the children. Parents’ education has been considered important in reducing the risk of IDA, and a strong association may exist between a child’s health and the educational level of the parents.28-32 On the other hand, parents’ consanguinity was not found to be a risk factor for IDA in the subjects of the present work. While the study of Sirdah reported an association between anemia and parents’ consanguinity among adolescent males, no significant difference was observed among females.33
The anemic status significantly affected the anthropometric characteristics of the young children. The anemic children were found to have a lower mean weight and shorter stature. The effect of anemia during pregnancy on the anthropometric measurements of Saudi newborns was studied by Telatar et al.; the authors revealed a significant negative effect of anemia on neonatal anthropometric measurements.34 The same finding was also reported by Dakshayani, who showed significant decreases in the anthropometric measurements of newborns born to anemic mothers.35 On the other hand, Ayoya et al. considered short stature and stunting as predictors of child anemia.36
The hematological parameters of cases and normal controls indicated significant differences between the two groups in all the CBC values except for WBC; the mean hemoglobin concentration for cases was 12.6 % lower than that in the control group. A remarkable finding of the present work is the success of our intervention to correct the anemic status of the children. The mean values of hematological parameters of the anemic cases before and after treatment revealed statistically significant improvements in most hematological parameters. Bopche et al. reported in Indian children an increase of 10% in hemoglobin concentration after one month of treatment,37 however the mean hemoglobin baseline value of their children was much lower (8.53g/dL) than that of our study group (10.4g/dL). In another setting, in Guatemala city, an improvement of 1.8g/dL in hemoglobin concentration was achieved in infants and young children after 28 days of treatment with ferrous sulfate.38 The superiority of these studies over ours could be due to different factors that include the commitment of the parents and children to the treatment, the coexistence of parasitic infections in the children, compliance with iron therapy and the bioavailability of the iron formula used.15,22,39
ConclusionIDA is a serious health problem among the 4- to 5-year-old children living in the less fortunate for development areas of the Gaza strip. Different risk factors for IDA were identified which could be helpful in reducing the prevailing IDA and improving the general health of children. The study justifies the necessity for systematic screening and interventional treatment of anemic children. Other nutritional deficiencies and infectious disorders should be included in future small and large screening studies. The national and international health related organizations working in Palestine should start urgent programs to develop health related programs in these marginalized areas of the Gaza strip, Palestine.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank the Palestinian Medical Relief Society (PMRS) for supporting the present study.


www.publicationethics.org.
- Home
- All contents
- Publish your article
- About the journal
- Metrics