





The purpose of this study was to evaluate the clinical-epidemiological profile, associated risk factors and clinical outcomes of patients with acute myeloid leukemia (AML), identifying the main causes of morbidity and mortality and overall survival rate of patients at five years of follow-up.
MethodThis was a retrospective cohort study evaluating the prognosis and clinical outcomes of 222 patients diagnosed with AML at three large hematology centers in Ceará (northeastern Brazil) over a period of five years.
ResultsThe mean age at diagnosis was 44.1 ± 16 years, with a female prevalence of 1.3:1. No additional relevant risk factors associated with the development of AML were found, except for the well-established cytogenetic assessment. The overall 5-year survival rate was 39.4% (95%CI: 35.47 - 42.17). The main causes of death were disease progression (37.72%; n = 84) and sepsis (31.58%; n = 70).
ConclusionThe clinical outcomes in our sample of AML patients were similar to those of other reported groups. Disease progression and infection were the main causes of death. Access to diagnostic flow cytometry and karyotyping was greater in our sample than in the national average. As expected, overall survival differed significantly according to the risk, as determined by cytogenetic testing.
Leukemia, a hematological neoplasm characterized by a monoclonal hyperproliferative disorder of hematopoietic cells of bone marrow origin, is the 10th most prevalent neoplasm in Brazil,1 with a worldwide incidence of 249,000 cases per year.2 The incidence increases annually and may be as high as 10% of the population over 68 years of age.2 In Brazil, estimates indicate 5.67 cases (men) and 4.56 cases (women) per 100,000 people of the population.1 The gross mortality among Brazilians with leukemia is 9,196 deaths per year. Leukemias in general is the 9th cause of death among women in Brazil, with an average case survival rate estimated at 60%.1 The median age at diagnosis of acute myeloid leukemia (AML) is 65 years, with a male-to-female incidence of 1.2 to 1.6:1.2
Despite the adoption of genetic mutations as the main prognostic factor for the clinical outcome of AML patients, it is important to investigate other non-cytogenetic factors which can make patients refractory to treatment and facilitate relapse.3 Molecular biology studies have identified genes involved in carcinogenesis, the most prevalent of which are those encoding myeloid transcription factors (RUNX1 and CBFA/CBFB) and signal transduction proteins (FLT3), for example the PML-RARA fusion gene, NPM1, CEBPA and MLL.3 Some target therapies for these mutations are gaining ground in association with the traditional induction regimen or as an option in recurrent or refractory cases.3
Unfortunately, the vast majority of Brazilian centers linked to the Unified Health Care System (SUS) do not provide access to such resources. A recent study of eleven referral centers found that only 51.2% of the services performed immunophenotyping at diagnosis and 42.7% provided access to karyotyping (though without precise molecular data).4 Patients may die before or during treatment (12% of cases)5 due to the severity of the disease itself (25%), bleeding disorders, bacterial, fungal and viral infections and treatment complications.5 The patient status at diagnosis, age, comorbidities, remission after induction and even socioeconomic and cultural profiles may impact survival rates. Based on clinical assessments, only 40% of the patients over 65 years of age are started on chemotherapy.6
The estimated cure rate for AML is currently 40 to 60%.7 Using the cytogenetic classification, the cure is estimated at 69% for low-risk patients, 24% for intermediate risk (including patients with normal karyotypes) and 6.5% for high risk.7 Old age also impacts cure rates: after the age of 70, the overall estimate drops drastically to 10% or less.2
These are global estimates. Little information is available for Brazil3,4,8 especially for its northeastern region. Environmental and epigenetic factors that may interfere in the pathogenesis or prognosis of AML patients need to be further investigated. For example, the effects of hypertension, diabetes, dyslipidemia and lifestyle on the development of AML are not fully understood.
The purpose of this study was to evaluate the clinical-epidemiological profile, associated risk factors and clinical outcomes of patients with AML, identifying the main causes of morbidity and mortality and overall survival rate of patients with five years of follow-up.
MethodsPatientsThis retrospective cohort study included 222 patients receiving chemotherapy treatment at three tertiary SUS hospitals (Hospital Geral de Fortaleza, n = 112; Hospital Universitário Walter Cantídio, n = 79, and; Hospital Cesar Cals n = 31) in Ceará, a state in northeastern Brazil, between January 2013 and December 2020, with 5 years of post-diagnosis follow-up. The chemotherapy protocols were the same at the three centers. Originally, information was retrieved from 273 medical records, but 51 were excluded due to duplication (n = 3) or unavailable/incomplete archive/clinical data (n = 48). The inclusion criteria were: patients of both sexes aged 18 years or over, diagnosis of AML on bone marrow aspiration showing the presence of blasts in a count equal to or over 20% of the cells represented with characteristics of myeloblasts9 and positive membrane surface staining for clusters of differentiation on immunophenotyping performed in flow cytometry.10 Pediatric patients and patients with other hematological diseases were excluded. Additionally, patients with acute promyelocytic leukemia with PML:RARA fusion were not excluded.
The study protocol was approved by the national clinical research platform (Plataforma Brasil, CAAE 44087220.0.1001.5052) and by the institutional review board. Following approval, the medical records were made available for analysis from May to July 2021. Data were collected by completing a questionnaire using the Google Forms platform. All patients or their legal representatives gave their written informed consent.
Clinical evaluation and outcomesThe hospitals participating in the study were requested to provide the medical records of patients diagnosed with the ICD codes C92, C92.0, C92.2, C92.4, C92.4, C92.5, C92.7 and C92.9. Information was collected on sex, date of birth, age at diagnosis and performance status at diagnosis according to the Eastern Cooperative Oncology Group (ECOG) performance scale (0 = fully active; 1 = restriction of physical activity, but able to work; 2 = able to perform self-care; 3 = limited self-care; 4 = completely unable, and; 5 = death).11
The presence of previous comorbidities was evaluated, including arterial hypertension (defined as systolic pressure ≥ 140 mmHg and/or diastolic pressure ≥ 90 mmHg), diabetes mellitus (defined as fasting blood glucose > 126 mg/dL or casual blood glucose ≥ 200 mg/dL), dyslipidemia (defined as LDL cholesterol ≥ 160 mg/dL or triglycerides ≥ 150 mg/dL or HDL ≤ 40 mg/dL in men and ≤ 50 mg/dL in women) and heart disease (defined as pre-chemotherapy echocardiography with an ejection fraction of ≤ 55%). The BMI was calculated by dividing weight (kg) by height (m) squared (overweight = BMI at 25 - 29.9 and obese = BMI ≥ 30).12
Information was also collected on smoking13 and alcohol14 consumption, family history of cancer (limited to first-degree relatives), previous radiotherapy or chemotherapy, personal history of hematologic diseases (myelodysplastic syndromes, chronic myeloid leukemia, chronic lymphocytic leukemia and myeloproliferative neoplasms) and occupational exposure. Non-melanoma skin cancer was not included.
The clinical history of the disease was recorded, starting with the initial symptoms (fever, weight loss, asthenia, hyporexia, bleeding, lymph node enlargement, hemorrhagic manifestations, infections and pain). The time from the onset of symptoms to diagnosis and from diagnosis to onset of treatment was documented, even for patients who died before initiating treatment. All diagnostic test results were recorded, including blood count, bone marrow aspiration, profile of immunophenotyping (according to the FAB classification: M0 = undifferentiated, M1 = minimal differentiation, M2 = poorly differentiated, M3 = promyelocytic, M4 = myelomonocytic, M5 = monocytic, M6 = erythrocytic, M7 = megakaryocytic and not applicable/not classified), karyotype with genetic alterations, categorized by risk (favorable, intermediate, unfavorable or high-risk) and molecular biology, when available.
Treatment response was evaluated, including remission after induction, refractoriness to chemotherapy, relapse during consolidations or after the end of the cycles, indication for and submission to bone marrow transplantation (BMT) (distinguishing between the presence and absence of compatible donors and whether they were evaluated) and the rescue schedule outcome. The main treatment regimen was the 7+3 protocol, or other options by azacitidine monotherapy, subcutaneous cytarabine or oral hydroxyurea as palliative therapy, the Pethema protocol15 and exclusive palliation.
The clinical outcome was documented, with the assessment of the disease status (disease in remission, active or cured) five years after diagnosis in patients without relapse. In addition, the presence or absence of relapse (including after BMT) and the time between the first remission and the first relapse were registered. Periodic blood count evaluations were performed and, if any change was observed, such as the presence of blasts, leukocytosis or cytopenias, the myelogram was used to document disease activity. Lab tests were performed 6 months, 1 year, 2 years and 5 years after diagnosis to identify the main causes of death (e.g., loss of response to treatment, infections, bleeding, chemotherapy toxicity, acute myocardial infarction and stroke).
For the purpose of statistical analysis, clinical and demographic parameters were expressed as mean values ± standard deviation (continuous variables) or as frequencies and percentages (categorical variables). Median values and ranges were calculated for non-normally distributed continuous variables. Kaplan-Meier charts were used to show patient survival at 6 months, 1 year, 2 years and 5 years. The level of statistical significance was set at 5% (p < 0.05). All analyses were performed using the software IBM SPSS Statistics (IBM Corp., Armonk, NY, USA).
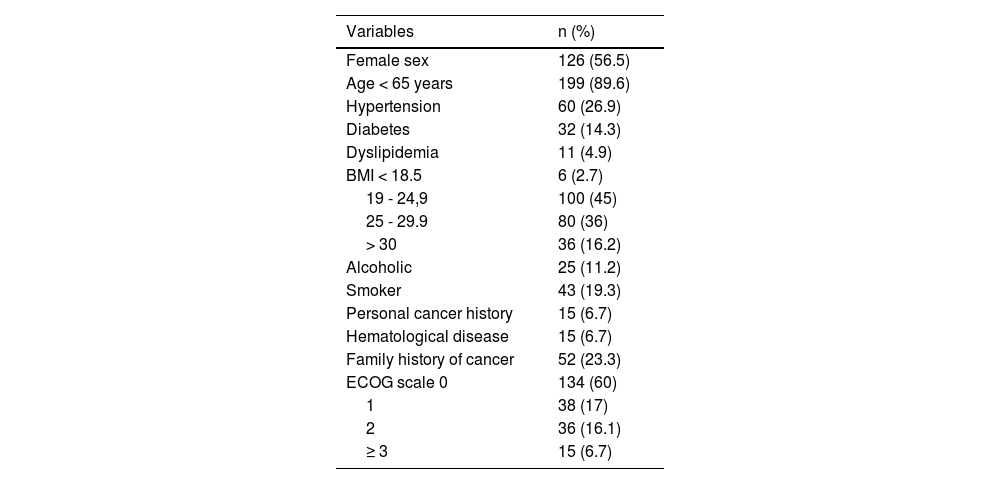
ResultsEpidemiological characteristicsThe female sex was slightly prevalent (56.5%) in our cohort of 222 patients. The mean age at diagnosis was 44.1 ± 16 years (range: 18 - 87). As for clinical status, most patients (60%) were classified on the ECOG scale as 0, while 17% were classified as 1 and 16.1%, as 2 (patients capable of going to an appointment alone). The minority (6.7%) were completely incapable. Many were overweight (36.0%) or obese (16.2%). Other comorbidities are shown in Table 1.
Statistical description of comorbidities in absolute values and percentages. BMI = body mass index (kg/m2). ECOG = Eastern Cooperative Oncology Group.
The most prevalent symptom was asthenia/adynamia (69.1%), followed by fever (51.9%), pain (39.8%), hemorrhagic manifestations such as petechiae, ecchymosis and bleeding from the gastrointestinal tract (46.5%) and dyspnea (24.5%). The mean values of the initial blood count were: hemoglobin 7.4 g/dL ± 2.1, white blood cells 41.245 ± 80.321/mm3 (of which 34.2 ± 32.2% were leukemic blast cells) and platelets 66.970 ± 84.101/mm3. Blasts accounted for 64% (median) on bone marrow aspiration. Almost all patients (94.1%; n = 209) had access to immunophenotyping by flow cytometry, but 20% (n = 44) did not have access to karyotyping, which is essential for cytogenetic risk stratification.
Karyotyping was performed for 177 patients, 22 of whom were without metaphase growth. The 155 cytogenetic results were divided into favorable (34.19%; n = 53), intermediate (52.25%; n = 81) and unfavorable (13.54%; n = 21) prognoses. The abnormality t(15;17) was observed in 14.4% (n = 27) and 34.2% (n = 53) normal karyotypes in patients with favorable and intermediate risk, respectively. Half of the patients (n = 111) had access to advanced molecular biology tests: PML-RARA fusion gene tests (n = 61), FLT3 mutation searches (n = 42), BCR-ABL (n = 27) and NPM1 (n = 20). Some patients had access to more than one type of test. Based on the results of the molecular biology tests, the patients were classified according to the WHO criteria into good (42.4%; n = 76), intermediate (41.9%; n = 75) and unfavorable (15.6%; n = 28) prognoses.
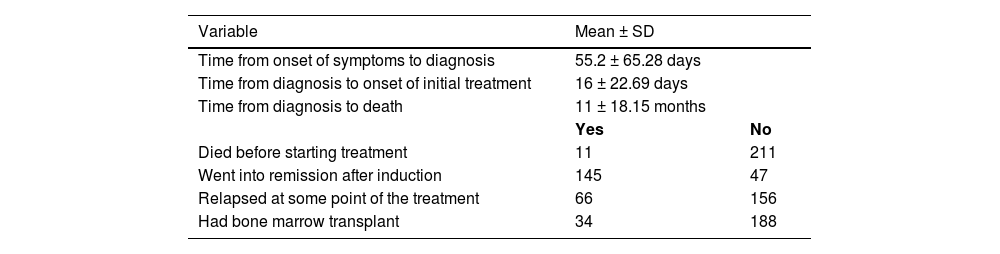
Access to treatmentThe mean time between the onset of symptoms and the diagnosis was 55.2 ± 65.3 days (median 30; range: 1 - 365). A few patients (4.9%; n = 11) died before initiating treatment, with a mean interval of 16 ± 22.7 days between the diagnosis and the onset of chemotherapy. After the induction protocol, 145 (68.7%) patients went into remission, 66 (29.7%) were refractory to treatment and 11 (4.95%) died. Despite being in remission at the time of the analysis, 29.7% (n = 66) were refractory to induction or relapsed and required rescue therapy at some point during the treatment. The BMT (considered a curative therapy) was performed in 34 individuals (15.3%). All patients were referred for BMT after the first remission.
Clinical outcomesThe 5-year median overall survival was 38.82 months (95%CI = 35.47 - 42.17). Furthermore, in 5 years, the overall survival rate was 39.4%; in 2 years it was 56.5%; 66.5% in one year, and; 74.9% in six months of follow-up. (Figure 1). No significant difference in survival was observed between the sexes (p = 0.3020), with 51.2% of women and 63% of men alive at 5 years. Eligibility for BMT was 40.2% for younger patients (< 65 years) and 27.03% for older patients (≥ 65 years) (Figure 2).
.")
 and older patients (≥ 65 years) with acute myeloid leukemia. (P-value” should have a hyphen in it).")
The median overall survival was 38.8 months.
The overall survival differed significantly according to the risk, as determined by cytogenetic testing (p = 0.003), with 46.11% survival of patients classified as favorable, 37.70% of patients classified as intermediate and 37.75% of patients classified as unfavorable. When patients with acute promyelocytic leukemia (APL) were excluded from the statistic, the values were 42.05% (favorable), 38.07% (intermediate) and 40.43% (unfavorable), with no significant difference (p = 0.216) (Figure 3).
 acute promyelocytic leukemia included in the cohort. (b) acute promyelocytic leukemia excluded from the cohort.")
Despite being in remission at the time of the analysis, 66 (29.7%) were refractory to induction or relapsed and required salvage therapy at some point during treatment. The initial response to the first cycle of chemotherapy had a positive effect on the final survival (59.10% who did not go into remission after induction died within 5 years). The main causes of death were progression of the underlying disease (37.72%), bacterial infections (32.58%), hemorrhage (8.80%) and thrombotic events, such as heart attack and strokes (5.36%) (Figure 4). For these patients, the time from diagnosis to death was 11.3 months, with a median of 6 months of treatment.
Discussion
The present investigation is one of the largest clinical-epidemiological and prognostic studies of AML patients with 5-year follow-up published so far. In it, we retrospectively analyzed the overall survival of 222 AML patients in northeastern Brazil. Additionally, given the large proportion of patients with access to prognostic stratification tests, cytogenetic risk was found to be a significant determinant of final clinical outcome. Finally, we identified the main causes of morbidity and mortality and analyzed the 5-year clinical outcomes.
In general, the literature shows a predominance of the male sex, with 5.2 new cases per 100,000 men and 3.6 cases per 100,000 women.2 In our cohort, however, the female sex was slightly predominant. Moreover, the worldwide mean age at diagnosis is 68 years,2 while in our study, it was only 44.1 ± 16 years. This may be due to selection bias, the younger Brazilian demographics, and/or a possible lack of prioritization of referrals of senile patients to large centers. In support of our findings, another Brazilian study also reported a mean age of 44 years, suggesting a national trend.4
Interestingly, access to complementary prognostic assessments was greater than the national average. In a study including 354 patients referred to 11 large southern/southeastern Brazilian centers for BMT,7 access figures were 51.2% for immunophenotyping, 42.73% for cytogenetic testing and 72% for molecular analysis. In contrast, a large proportion of our patients had flow cytometry data and cytogenetic (80%) and molecular biology (50%) tests, all of which were covered by the SUS. As new targeted therapies are implemented, the establishment of the genetic and molecular profile of patients is increasingly important in treatment decisions.
The available test results made it possible to classify patients according to risk.16 Thus, risk was favorable in 76 (42.45%), intermediate in 75 (41.89%) and high in 28 (15.64%). Data from the National Cancer Institute in Rio de Janeiro (INCA) show a risk distribution of 25%, 50% and 25%, respectively, while the world average is 45%, 21% and 34%.7,17-19 However, the INCA data are nonspecific, covering all leukemias (with AML accounting for 40%).1 As expected, survival was higher in the favorable risk group (46.1%) than in the intermediate risk group (37.70%) and the unfavorable risk group (37.75%), although the last two groups displayed almost identical percentages. Data from other Brazilian centers show a five-fold difference in survival (55% x 11%) between favorable and unfavorable cytogenetic risk,4,8 reinforcing our findings and illustrating the importance of access to risk classification for the alignment of patient and family expectations, decision-making and referral for BMT.
Despite the large proportion of patients with intermediate and unfavorable cytogenetic risk, few patients in our cohort underwent BMT. The main reason for this was limited access to transplantation services, delayed consultations (some patients experienced relapse while awaiting complementary tests and donor preparation) and socioeconomic restrictions. Prognosis was also influenced by the unavailability of advanced medications, such as FLT3 inhibitors and IDH1/2, in the public health care system (SUS). Such medications would allow for the administration of a 3rd or 4th line of treatment and improve chances of BMT.
The initial response to treatment (i.e., remission after the induction chemotherapy protocol) was confirmed by < 5% bone marrow blasts, suggesting a better final outcome. The difference was not significant (p = 0.476), although 59.10% of the 75 patients with no remission after induction died.
Following disease progression, infections (some of which involved multidrug-resistant bacteria and fungi) were the main cause of death, accounting for one-third of the deaths. This reflects the vulnerability of patients during neutropenia and secondary to chemotherapy and the need for special measures of hygiene and awareness of the multidisciplinary team. Beds in reverse isolation, the use of high-efficiency particulate arrestance filters and personal protective equipment (gloves, masks, hats and aprons), the adoption of strict protocols for the management of febrile neutropenia and instructions concerning the rational use of antimicrobials to prevent bacterial resistance are essential to improve the survival of these patients. The chemotherapy protocols adopted at our local services are standardized and compliant with international guidelines, avoiding the comparison of inferiority of treatment and drugs.
Our study was limited by the absence of a multivariate analysis of risk factors (such as obesity), which could independently interfere with patient survival, and by the absence of a stratification of patients who died during induction or in complete remission (CR). Furthermore, as is often the case with retrospective studies, a number of patients were excluded from the cohort due to incomplete data. Before reaching tertiary centers, many patients die of the disease before they can receive treatment or even before an initial diagnosis is established. Finally, the lack of a control group in the study made it more difficult to draw conclusions regarding the impact of risk factors on the development of AML.
ConclusionThe clinical outcomes of our cohort of AML patients were similar to those reported for other groups. Disease progression and infection were the main causes of death. Patients had greater access to diagnostic cytometry and karyotyping than the national average. As expected, the overall survival differed significantly according to risk, as determined by cytogenetic testing. Further studies involving larger regional samples and a longer follow-up will allow for more meaningful conclusions regarding the prognosis of AML patients (Table 2).
Statistical description of the clinical course of acute myeloid leukemia during follow-up in our cohort of patients. SD = standard deviation. (The word “unknown” is missing the final “n”).
This research received no specific grant from funding agencies in the public, commercial or not-for-profit sectors.


