
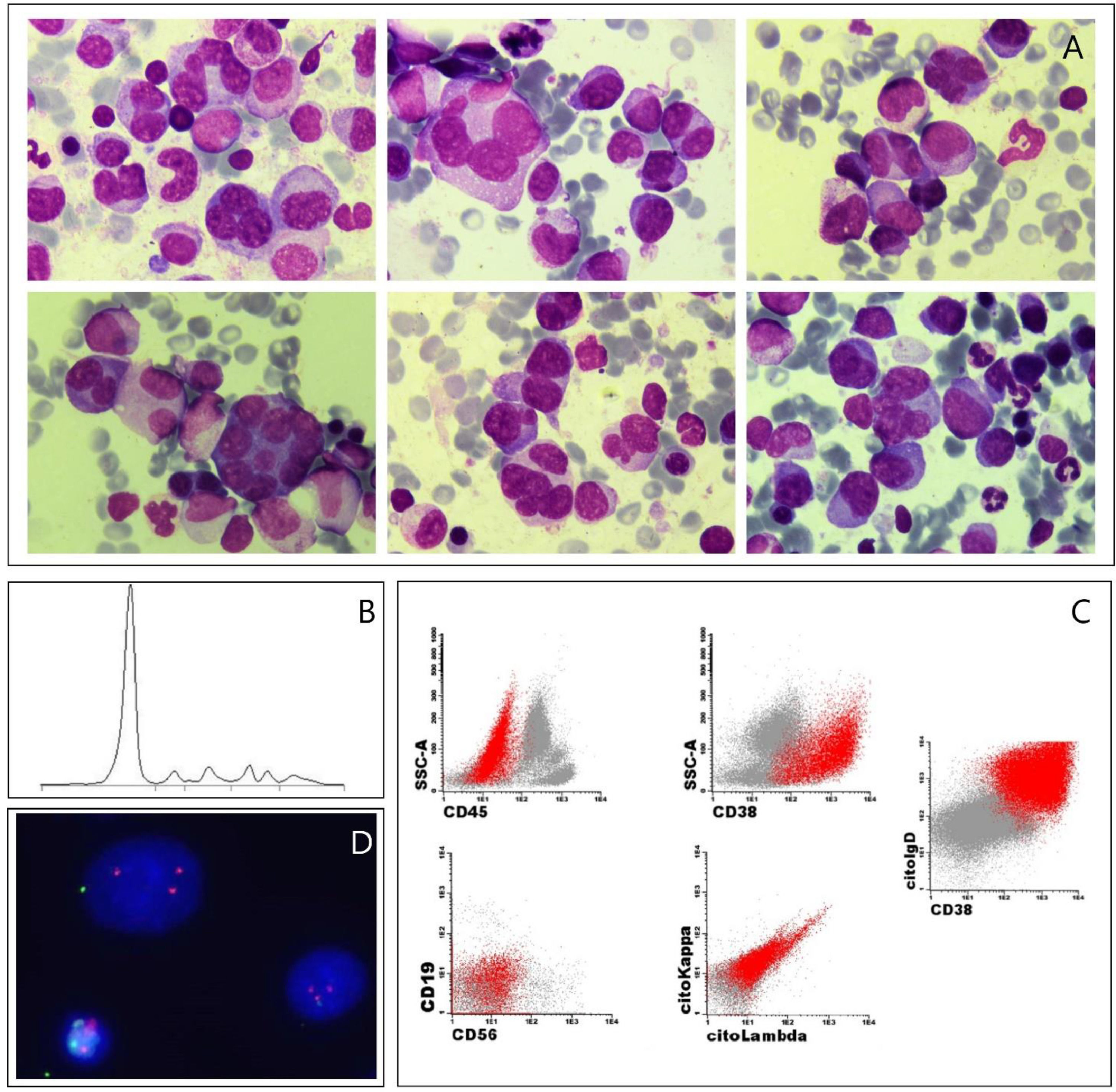
A 79-year-old woman was admitted to our hospital with weakness and weight loss. Physical examination was unremarkable. Blood count showed: hemoglobin 111g/L, MCV 88.2 fL, platelet 92 × 109/L, leukocytes 3.5 × 109/L (neutrophils 0.9 × 109/L). The peripheral blood smear was normal. Serum calcium and renal function were normal. The lactate dehydrogenase was 301 UI/L (normal: 0-250). Bone marrow smear showed a hypercellular marrow with an infiltration of 63% by atypical plasma cells with large nucleus showing frequently cleaved and multilobated nuclei (near similar lo megakaryocytes in size), some of them with one or more nucleoli, suggesting multiple myeloma (MM) (Figure 1A). Serum protein study (including IgD quantification and intracytoplasmic IgD flow cytometry) were requested. The serum protein study showed (Figure 1B): monoclonal component 0.2g/dL of IgD lambda nature, IgD 122 mg/dL (normal: 2-10 mg/dL) and immunoparesis. Multiparameter flow cytometry confirmed a 24% of plasma cells with aberrant phenotype: CD38 +high, CD138 +, CD19-, CD56-, CD27 +/-, CD81 +/-, CD20-, CD117-, cykappa-, cylambda-, cyIgD+ (Figure 1C). Karyotype: 46, XX, add(1)(p22)[5]/ 46,XX[15]. Fluorescence in situ hybridization (FISH): 1p deletion, 1q gain and monosomy 14 (Figure 1D). Computed tomography scan did not show lytic lesions. The diagnosis of MM IgD Lambda stage IA ISS2 was made. The patient initially has been treated with bortezomib, melphalan and prednisone schedule achieving a complete response but analytically relapsed at sixth month. Currently (45 months after diagnosis), she receiving fourth line therapy.
. B. Serum protein electrophoresis. C. Bone marrow flow cytometry study showing in red the clonal plasma cells phenotype. D. Interphase fluorescence in situ hybridization showing 1p deletion and 1q gain.")
A. Bone marrow smear showing atypical plasma cells: giant mutilobated, with cleaved nuclei and with evident nucleoli (May-Grünwald-Giemsa stain, x1000). B. Serum protein electrophoresis. C. Bone marrow flow cytometry study showing in red the clonal plasma cells phenotype. D. Interphase fluorescence in situ hybridization showing 1p deletion and 1q gain.
MM IgD is rare (1-2% of all MM). Owing to this, neither the serum IgD quantification nor the performance of intracytoplasmic IgD by flow cytometry are initially routinely done, even with MM suspicion. There is also greater difficulty detecting IgD monoclonal component, since M-spike is usually subtle or unrecognizable and IgD ratio synthesis rate is 10 times less than that of the rest of serum immunoglobulins and has a short half-life. IgD MM typically involves to younger patients with advanced stages, extramedullary disease, and associated amyloidosis at diagnosis. Unlike other MM, IgD MM has a lambda chain predominance and presents more often gain of 1q. IgD MM have been classically related to a worse prognosis with a median overall survival between 13 to 36 months, although the arrival of new treatments is putting it on questionable and further studies are needed to affirm it.1-3
Anaplastic MM (AMM) is a very uncommon morphological subtype of myeloma (2%) and it is associated with aggressive clinical course and poor prognosis. Some patients are diagnosed of AMM at disease onset but others develop anaplastic morphology during disease evolution.4 The pleomorphic morphology of AMM may resemble metastatic tumor cells.
This case is curious due to its morphology as well as the nature of the monoclonal component and its presentation in an early stage despite them.


