


Diversity in Classical Hematology Research
More infoTo evaluate and estimate the cost of basic care in sickle cell disease (SCD) for patients under five years of age, within the scope of the Unified Health System (SUS) and to discuss the costs related to possible complications of the disease from the literature.
MethodsThe main management and conduct recommendations in the SCD up to five years of age, with healthy and baseline health status, were extracted from the Basic Guidelines of the Care Line in the SCD of the Ministry of Health. Systematic data regarding costs of medicines were extracted from the Medicine Market Regulation Chamber. The SUS Table of Procedures, Medicines and Orthotics, Prosthetics and Auxiliary Means of Movement Management System was the guide for the values of complementary exams, as well as for medical consultations. The values applied to calculate the vaccination schedule were extracted from the Pan American Health Organization, adopting the perspective of the SUS-paying costs.
ResultsThe total cost obtained for basic care of SCD in children up to five years of age, including the use of antibiotic prophylaxis, immunizations and the performance of transcranial Doppler ultrasound in the prevention and early detection of cerebrovascular accidents was, on average, $1020.96.
ConclusionThe cost-effectiveness of prophylaxis in SCD, up to five years of age, exceeds the expenses resulting from hospitalizations due to complications of the disease. The study of expenses associated with SCD could be used to establish public policies, improve prevention strategies and treat the symptoms and complications of the disease.
The first scientific report on Sickle Cell Disease (SCD) was written in 1910 by the American scientist James B. Herrick.1 The term SCD refers generically to a set of recessive genetic and hereditary alterations, resulting from a mutation in the gene that encodes the β-subunit of Hemoglobin (Hb). This mutation occurs in the sixth position of chromosome 11, responsible for the synthesis of Hb, with the substitution of Glutamate by Valine (Glu6Val, β S), leading to the production of an anomalous Hb - HbS, which determines the pathophysiology of SCD.2–4 In the homozygous form (HbSS), there is a formation of a pathological tetramera Hb (α2βS 2, HbS), constituting the most frequent and severe form of SCD, called Sickle Cell Anemia (SCA). The other types of SCD include the heterozygous double forms, such as Sβ-thalassemia, where there is an HbS mutation associated with thalassemia, to HbSC, HbSD or HbSO Arab. The phenotypic variability results from the levels of HbFetal (HbF) and the concomitant inheritance with α-thalassemia, which determines a better prognosis for SCD.3–5
The pathophysiological mechanisms related to SCD are complex and not completely understood. It is known that the presence of HbS alters the conformation of erythrocytes, which when deoxygenated, undergo reversible polymerization changing the flexible erythrocyte biconcavity, taking on a rigid and elongated shape, with a sickle appearance.5,6 It is described as a consequence of the presence of HbS and the decrease in oxygen affinity, changes in the morphology of the red blood cell membrane, with a reduced time in useful survival when compared to healthy erythrocytes (from 120 to 15 days), increased oxidative stress, free Hb and intra- and extravascular hemolysis, altered arginine metabolism, activation of the innate immune system and endothelial cell adhesion in vaso-occlusion, which may culminate in multiple organ failure and oxidative and inflammatory stress.2,4,6–9
Every year, approximately 300,000 children are born with SCA in the world and it is predicted that by 2050, this number could reach 400,000/year. SCD is considered a global and growing public health problem, in which approximately 7% of the world population has some Hb disorder, with SCA being the most frequent.2,7,8,10 In Brazil, free and early diagnosis is carried out through the National Neonatal Screening Program.11 In the healthcare service specialized in hemoglobinopathies, the introduction of antibiotic prophylaxis and the continuous use of folic acid is started. Prophylactic care represents the essence of treatment, especially in the first five years of life.11 This period of life was considered as having the highest mortality and severe complications of SCD, such as microinfarcts due to diffuse microvascular vaso-occlusion, acute chest syndrome (ACS), stroke, splenic sequestration, aplastic crisis and bacterial infections, which, together with the painful crisis, lead patients to hospital admissions, which may result in death.2,7–10
The Brazilian literature on aspects related to the costs of SCD was very limited and scarce and the complete calculation could be complex due to possible complications related to the disease. On the international scene, Kauf et al. (2009)12 and Bou-Maroun et al. (2018)13 described costs associated with SCD complications among children and adults. The objective of this study was to evaluate and estimate the cost of basic care in SCD for patients under five years of age, within the scope of the Unified Health System (SUS) and to discuss the costs related to possible complications of the disease from the literature.
MethodsThis study was based on the Basic Guidelines of the Line of Care in SCD of the Ministry of Health (MH) (2015)2 and Portaria nº 822/200114 to calculate the costs of procedures, exams, medical appointments and basic medications in the treatment of children with SCD. The MH government guidelines and official documental analysis were complied with, as recommended by Bardin.15
The unit costs of the resources were obtained from public sources: the prices of the medicines were obtained from the public consultation page of the Medicine Market Regulation Chamber (CMED) and the values related to complementary imaging, laboratory and medical appointments were extracted from the SUS Unified Procedures Table, available in the Management Table of Procedures, Medicines, Orthoses, Prostheses and Special Materials (http://sigtap.datasus.gov.br/). This is a tool for consulting for all procedures that can be performed at a hospital and at an outpatient clinic that integrate the SUS Unified Procedures Table. The costs applied to calculate the vaccination schedule in the SCD were extracted from the Pan American Health Organization (PAHO). The cost perspective adopted was that of the SUS as the payer, that is, paid by the health system to service providers and reference centers for the treatment of SCD in the public network.
The CMED Price Database contains the maximum drug prices per active ingredient, for public purchases in the factory price (PF), maximum government sale price (PMVG) and maximum consumer price (PMC) categories. The PF is the maximum price allowed for sale to pharmacies, drugstores and public administration entities. The PMVG is the price ceiling for the purchase of medicines included in the list of products subject to Price Adequacy Coefficient (CAP) and of all medicines purchased by a court decision the PMC, which is the price to be charged by the retail drug trade, that is, pharmacies and drugstores.
The PF of the Medicines Price Table was used in the updated version (2022) and the Tax on Circulation of Goods and Services (ICMS) rate was not included. Thus, the unit price was calculated considering the PF of drugs routinely dispensed to patients with SCD. The costs were calculated as a product between the resources used and the unit value of each item, per patient and the costs of possible complications of the disease that would determine tertiary and/or quaternary care were excluded. The exchange rate of the dollar considered for the whole research was R$5,395, which was the average exchange rate in the year 2021.
The research for the theoretical basis of this article was performed in the Medical Literature Analysis and Retrieval System Online (MedLine/PubMed) database between January 2009 and June 2021, with the descriptors: sickle cell anemia AND costs AND cost analysis and its variations according to with Medical Matters Headers (MeSH).
This study was approved by the Research Ethics Committee of the Fundação Hemominas and was registered under number 3,489,059.7.
ResultsThe care related to children under five years of age with SCD, in a stable and basal state of health, according to the Basic Guidelines for the Healthcare Line of the Ministry of Health (2015),2 with its frequency and cost are described in Table 1.
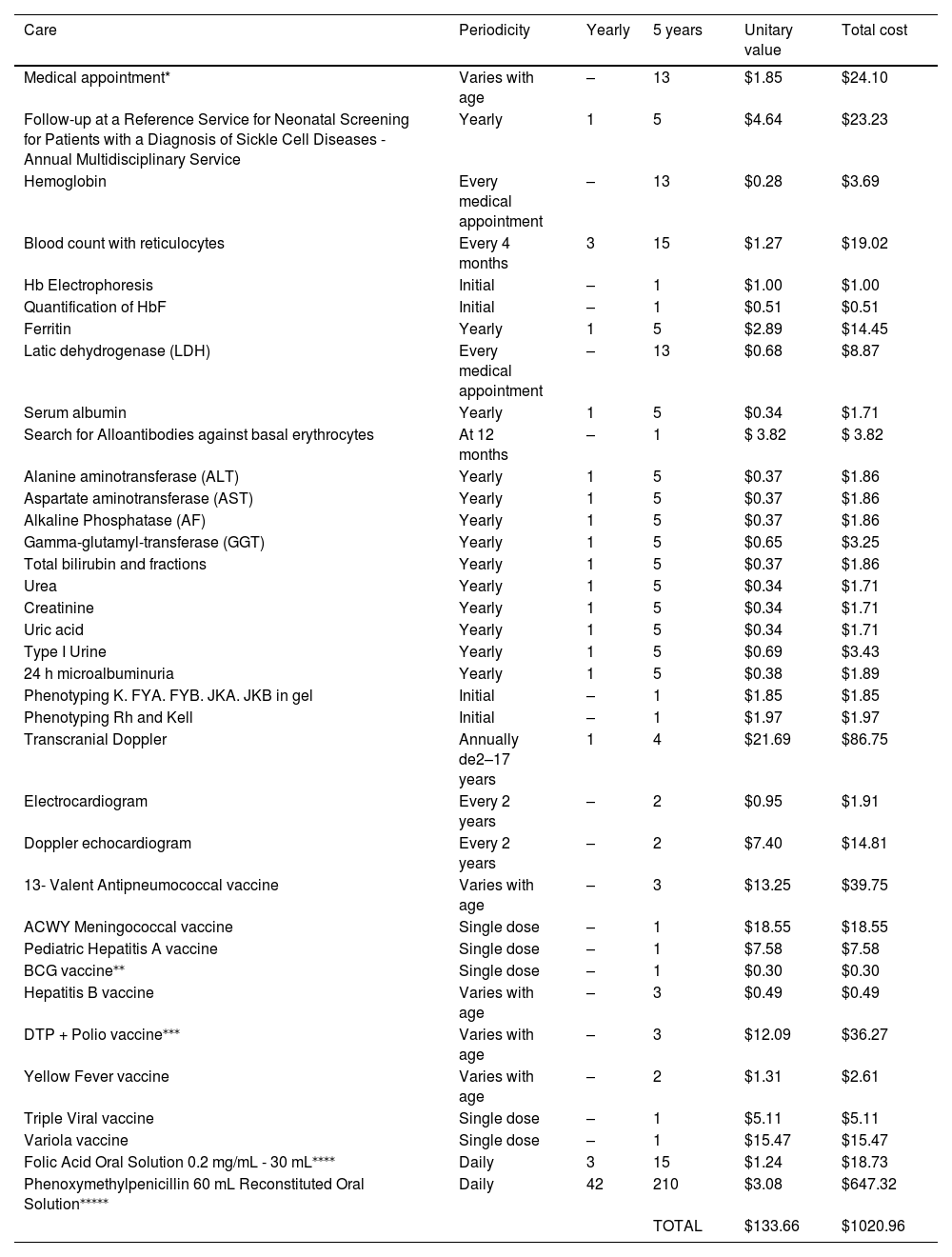
Basic handling and care costs for patients with SCD under five years of age.
| Care | Periodicity | Yearly | 5 years | Unitary value | Total cost |
|---|---|---|---|---|---|
| Medical appointment* | Varies with age | – | 13 | $1.85 | $24.10 |
| Follow-up at a Reference Service for Neonatal Screening for Patients with a Diagnosis of Sickle Cell Diseases - Annual Multidisciplinary Service | Yearly | 1 | 5 | $4.64 | $23.23 |
| Hemoglobin | Every medical appointment | – | 13 | $0.28 | $3.69 |
| Blood count with reticulocytes | Every 4 months | 3 | 15 | $1.27 | $19.02 |
| Hb Electrophoresis | Initial | – | 1 | $1.00 | $1.00 |
| Quantification of HbF | Initial | – | 1 | $0.51 | $0.51 |
| Ferritin | Yearly | 1 | 5 | $2.89 | $14.45 |
| Latic dehydrogenase (LDH) | Every medical appointment | – | 13 | $0.68 | $8.87 |
| Serum albumin | Yearly | 1 | 5 | $0.34 | $1.71 |
| Search for Alloantibodies against basal erythrocytes | At 12 months | – | 1 | $ 3.82 | $ 3.82 |
| Alanine aminotransferase (ALT) | Yearly | 1 | 5 | $0.37 | $1.86 |
| Aspartate aminotransferase (AST) | Yearly | 1 | 5 | $0.37 | $1.86 |
| Alkaline Phosphatase (AF) | Yearly | 1 | 5 | $0.37 | $1.86 |
| Gamma-glutamyl-transferase (GGT) | Yearly | 1 | 5 | $0.65 | $3.25 |
| Total bilirubin and fractions | Yearly | 1 | 5 | $0.37 | $1.86 |
| Urea | Yearly | 1 | 5 | $0.34 | $1.71 |
| Creatinine | Yearly | 1 | 5 | $0.34 | $1.71 |
| Uric acid | Yearly | 1 | 5 | $0.34 | $1.71 |
| Type I Urine | Yearly | 1 | 5 | $0.69 | $3.43 |
| 24 h microalbuminuria | Yearly | 1 | 5 | $0.38 | $1.89 |
| Phenotyping K. FYA. FYB. JKA. JKB in gel | Initial | – | 1 | $1.85 | $1.85 |
| Phenotyping Rh and Kell | Initial | – | 1 | $1.97 | $1.97 |
| Transcranial Doppler | Annually de2–17 years | 1 | 4 | $21.69 | $86.75 |
| Electrocardiogram | Every 2 years | – | 2 | $0.95 | $1.91 |
| Doppler echocardiogram | Every 2 years | – | 2 | $7.40 | $14.81 |
| 13- Valent Antipneumococcal vaccine | Varies with age | – | 3 | $13.25 | $39.75 |
| ACWY Meningococcal vaccine | Single dose | – | 1 | $18.55 | $18.55 |
| Pediatric Hepatitis A vaccine | Single dose | – | 1 | $7.58 | $7.58 |
| BCG vaccine⁎⁎ | Single dose | – | 1 | $0.30 | $0.30 |
| Hepatitis B vaccine | Varies with age | – | 3 | $0.49 | $0.49 |
| DTP + Polio vaccine⁎⁎⁎ | Varies with age | – | 3 | $12.09 | $36.27 |
| Yellow Fever vaccine | Varies with age | – | 2 | $1.31 | $2.61 |
| Triple Viral vaccine | Single dose | – | 1 | $5.11 | $5.11 |
| Variola vaccine | Single dose | – | 1 | $15.47 | $15.47 |
| Folic Acid Oral Solution 0.2 mg/mL - 30 mL⁎⁎⁎⁎ | Daily | 3 | 15 | $1.24 | $18.73 |
| Phenoxymethylpenicillin 60 mL Reconstituted Oral Solution⁎⁎⁎⁎⁎ | Daily | 42 | 210 | $3.08 | $647.32 |
| TOTAL | $133.66 | $1020.96 |
The sum of the values for all procedures listed in Table 1 was $1020.96 (value obtained for the total cost of primary care for children under five years old with SCD, including prophylaxis against fulminant sepsis by encapsulates with a differentiated vaccination schedule and antibiotic therapy).
DiscussionHealthcare for people with chronic diseases must be continuous, coordinated, multidisciplinary and comprehensive, so that the demands triggered by the disease are minimized. Improving the survival and quality of life of these patients is based on general and preventive measures. The daily life of the child with SCD, from the establishment of the diagnosis, changes drastically, starting to be guided by the conditions and limitations of the disease and treatment, which can lead to a long journey, interspersed with fears, anxieties, uncertainties and frustrations. The Primary Healthcare (PHC) team, as well as the other services in the care network, must be guided by a continuous, integral and active follow-up of these children.16–18
The Family Health Strategy had a pivotal role in assisting people with SCD. Bonding patients and their families with the health team is essential to facilitate understanding of the disease, predict risk situations and avoid complications that require hospital admission, thus helping to adhere to basic therapeutic measures.19
SCD carriers are exposed to different circumstances that can determine a reduction in their quality of life. Continuing education of health professionals on the management of SCD and health learning activities for both patients and family members must be stimulated to increase the rates of adherence to the recommended therapy, reduce disease exacerbations and improve the quality of patients' lives.18
Also, in the context of PHC, the importance of monitoring growth and development, monitoring adherence to prophylactic antibiotic therapy and routine and special calendar vaccines are highlighted, including guidelines with an emphasis on personal care, the environment and other triggering factors of acute episodes.20 Simple measures taken at this level of the Healthcare Network help to reduce the need for more complex services and, therefore, the costs related to the pathology.
Estimating the cost of treating patients in specific therapeutic regimens is complex, but extremely important to support the development and implementation of public health policies. Therapeutic measures in SCD can impose a significant financial impact on the SUS, as they involve regular multidisciplinary appointments, genetic counseling, differentiated immunization regimen, prophylactic use of penicillin, periodic laboratory tests, biannual cardiopulmonary assessments, continuous use medications, blood transfusions,2 in addition to the regular annual screening for the early detection cerebrovascular disease between 2 and 17 years and, in cases of changes in cerebral blood flow velocity (CBFV), measured in reduced intervals,17 as well as the appropriate individualized and instituted therapeutic. Added to this, the epidemiology of SCD is high in incidence, especially in the population of African descent, who in Brazil, are people with greater social vulnerability.
The cost analysis in SCD is an instrument that enables the ideal planning to face this genetic pathology that is highly prevalent in the population. It was observed that the total cost of basic therapeutic measures recommended by the MH was $1020.96 per patient under five years of age, procedures with a low value, considering the budget allocated to health in Brazil, especially when compared to the costs of complications likely to occur if these primary measures are not offered to patients and/or followed by them. According to the Brazilian Federal Government's Transparency Portal,21 spending on the health sector in 2019 (pre-pandemic period) was $727,149,561.21. Considering this value and the epidemiology of the disease in the country (approximately 3000 live births annually), the basic costs of sickle cell patients up to five years of age do not have a significant impact on this budget.
The main objectives of such measures are to reduce the complications of the pathology and improve the quality of life of these individuals, as well as to reduce costs related to the disease. The costs of prophylactic measures against infections were shown to be lower, especially when compared to those related to the management of possible infectious complications. The vaccine and antibiotic prophylaxis recommended by the Brazilian Society of Pediatrics, through simple and low-cost measures, when instituted early, can change the course of the pathology and improve the quality of life of these patients. In Brazil, the total cost of such therapy was $666.05/per patient, adding the recommended vaccines and phenoxymethylpenicillin. It is noteworthy that the cost of this medication is the highest among the therapies recommended for sickle cell patients under five years of age. Despite this, the value is considered low, compared to the efficiency of prophylaxis, significantly impacting the reduction of SUS expenses with highly complex services.
Regarding studies on SCD, the literature in general addresses the costs associated with hospitalization within different complications, which raises and distorts the estimated cost of care for these patients, since the healthcare needed at the hospital level is generally more costly than comprehensive healthcare at primary and secondary levels of the health network.
On the international scene, Kauf et al. (2009)12 described an average monthly cost, related to SCD and its complications, of $471 per patient aged 0 to 9 years. In the 30 to 39 age group, the average monthly cost was the highest, reaching $1913. The characteristic of these costs, in the study, was the increase up to the age of 30 years and the decrease until the age of 64 years. In Bou-Maroun et al. (2018),13 patients with SCD cost $14,337 per hospital stay due to complications. Black patients accounted for the majority of admissions. Individuals between 16 and 20 years old accounted for 38.4% of admissions. The overall mortality associated with any hospital stay was 0.1%. The presence of congenital heart disease, sepsis, stroke or acute chest syndrome (ACS) increased the risk of patient death during pediatric hospitalizations, in addition to increasing its cost.
In Brazil, few studies have been published evaluating the financial and budgetary issues of the care line for chronic diseases. Lobo et al. (2022)22 studied the costs associated with the treatment of sickle cell disease (SCD) in low- and middle-income countries and reported that analgesics, antibiotics and housing were at the forefront of most expenses in SCD acute events. Hospitalization costs were higher among children, compared to adults.
The severity degrees of SCD are extremely variable, defined by several causal factors, which determine the complexity of the illness phenotypes. As a result, a significant variation in health costs was observed.23 Shah et al. (2020)24 developed an SCD severity score that considered factors, such as age, number of hospitalizations for a vaso-occlusive crisis in the last year, diagnosed target organ damage, present chronic pain and patient genotype. With these parameters, three classes of severity were stratified: Class I) demands less care for the health system; Class II) presents a chronic condition with some degree of damage to target organs, and; Class III) requires frequent hospitalizations.
In children and young adults, hospitalizations resulting from cardiac complications, sepsis, stroke, acute chest syndrome (ACS) and multiple organ failure, in addition to the high cost to the system, are related to high in-hospital mortality rates.25 The knowledge of expenses associated with SCD can be used as an important tool to improve strategies for the prevention and treatment of symptoms and complications of the disease, resulting in better care and reduced costs and mortality.
Martins and Teixeira (2017)26 described the profile of hospitalizations for sickle cell disease and the calculation of costs in the state of Bahia and outlined the costs related to hospitalizations.
Estimating the cost of care is both relevant and a priority in ensuring the proper allocation of resources and reimbursements. Most studies on the cost of illness focused on a few aspects of care, such as hospitalizations and medical appointments, and no studies were found that examined healthcare expenditures exclusively for children under five years old. Another fact to be considered is that most studies were based on samples from North America, with large discrepancies between health systems, which makes a poor correlation with public health policies in Brazil.23
Considering that basic care in SCD proposed by the MH of Brazil has a budget of $1020.96, all expenses arising from the use of more complex drugs, procedures, hospitalizations and surgeries bring a greater burden to the public health system. In this sense, it is important to adopt the measures listed in the aforementioned guideline,2,17 especially those taken in the PHC, so that the natural history of SCD can be controlled and closely monitored. Neonatal Screening, which aims at the earliest possible diagnosis and antibiotic prophylaxis, minimizing mortality due to encapsulated germs in children with SCD in the age group in question, deserve special mention.
It has been observed that several actions and services provided in the Basic Guidelines of the Sickle Cell Disease Care Line occur inappropriately, mainly due to the structuring of the Care Network and the irregular availability of services in different regions of the country. A study performed in northeastern Brazil,27 a region with a high incidence of SCD, showed that 87.5% of patients did not regularly attend scheduled consultations and that most performed the recommended routine exams in an unsatisfactory manner, with blood count, ferritin and lactic dehydrogenase being inadequately periodically performed by 77%, 79.1% and 94.8% of patients, respectively. The transcranial doppler was performed in only 20.8% of the research participants. Failure to carry out such therapies as recommended incurs an increase in costs related to SCD, as it leads to greater complications that demand more specialized services and, consequently, more expensive than the follow-up described in our research.
The implementation of public health policies in Brazil instituted by the Federal Constitution of 1988 was partially conditioned by the process of small, chronic financing of SUS, which can be characterized by insufficient allocation of budgetary and financial resources, both to fully comply with the constitutional principles of universality, integrality and equity and for the comparative comparison with other countries that adopt public health systems similar to the Brazilian one.28
The international and national literature presents few articles correlating the costs of primary healthcare. Some articles show the high cost of hospitalization.22,26,29,30 The scope of our work focused on the study of the cost of basic actions and not on tertiary and quaternary care. The relevance of this research is the novelty and the creation of an instrument for consultation, helping health managers and professionals in the proper allocation of resources. The importance of training professionals in the Healthcare Network is vital in helping the early identification of possible complications, with the possibility of unburdening the public health service, strengthening prevention and support from a holistic view of the patient, as recommended by the World Health Organization (WHO).
ConclusionThe costs of managing Sickle Cell Disease in children under five years of age, according to the guidelines of the Brazilian Ministry of Health2 and recommended by Portaria 822/2001,14 are not high. The early diagnosis through neonatal screening, antibiotic prophylaxis, extended active immunization (vaccines), multidisciplinary follow-up and the Transcranial Doppler Protocol17 are examples of effective and already implemented public policies that have a positive impact on children's quality of life, with reduced morbidity and mortality, with costs considerably lower than spending on hospitalizations for complications of the disease. The study of the costs associated with the monitoring of SCD should be a tool used to improve and define strategies for the prevention and treatment of symptoms and complications of the disease, resulting in better care and better quality of life, with the optimization of the scarce resources available for health.
The effective practice of primary care for SCD is of paramount importance to children with the disease, in addition to being a feasible, viable and effective action in preventing complications, improving clinical conditions and increasing survival, reducing the incidence of vaso-occlusive crisis, stroke, sepsis and ACS. The importance of our article is to create a referenced database that can be used to plan new care guidelines and estimate the cost benefits of current and future therapies for SCD.


