

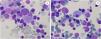

A 38-year-old woman, natural from Nigeria, known case of alpha-Thalassemia minor, S hemoglobin carrier, and chronic renal failure was remitted due decreasing hemoglobin level. She was in treatment with erythropoietin and endovenous iron. Laboratory tests showed: hemoglobin of 95 g/L, platelets of 130 × 109/L and white blood cells 4.1 × 109/L, reticulocytes 1.7%, lactate dehydrogenase 273 IU/L (slightly increased) and glomerular filtration 3 mL/min/1.73 m2. Bone marrow smear showed a hypercellular marrow with increased erythroid precursors without dysplastic changes and incidental Pseudo- Gaucher cells (PGC) (Figure 1 A-B, May-Grumwald-Giemsa x1000). Bone marrow biopsy did no evidence fibrosis nor infiltration.

PCG are histiocytes with round contour and cytoplasm resembling “onion layers”. By morphology PCG are indistinguishable from true Gaucher cells. PGC are found in cases with high cell turnover. The presence of PGC has been documented in different hematological diseases being most common chronic myeloid leukemia but also in myelodysplastic syndromes, myeloma and other lymphoproliferatives, myelofibrosis and major thalassemia.1,2



