









Minimal residual disease is the most powerful predictor of outcome in acute leukemia and is useful in therapeutic stratification for acute lymphoblastic leukemia protocols. Nowadays, the most reliable methods for studying minimal residual disease in acute lymphoblastic leukemia are multiparametric flow cytometry and polymerase chain reaction. Both provide similar results at a minimal residual disease level of 0.01% of normal cells, that is, detection of one leukemic cell in up to 10,000 normal nucleated cells. Currently, therapeutic protocols establish the minimal residual disease threshold value at the most informative time points according to the appropriate methodology employed. The expertise of the laboratory in a cancer center or a cooperative group could be the most important factor in determining which method should be used. In Brazil, multiparametric flow cytometry laboratories are available in most leukemia treatment centers, but multiparametric flow cytometry processes must be standardized for minimal residual disease investigations in order to offer reliable and reproducible results that ensure quality in the clinical application of the method. The Minimal Residual Disease Working Group of the Brazilian Society of Bone Marrow Transplantation (SBTMO) was created with that aim. This paper presents recommendations for the detection of minimal residual disease in acute lymphoblastic leukemia based on the literature and expertise of the laboratories who participated in this consensus, including pre-analytical and analytical methods. This paper also recommends that both multiparametric flow cytometry and polymerase chain reaction are complementary methods, and so more laboratories with expertise in immunoglobulin/T cell receptor (Ig/TCR) gene assays are necessary in Brazil.
Minimal residual disease (MRD) is today considered the most powerful predictor of outcome in acute leukemias, including acute lymphoblastic leukemia (ALL). Although classical factors such as age, cytogenetic and molecular features, and leukocyte count are taken into account to establish the initial risk groups for therapeutic purposes, the evaluation of treatment response by MRD detection allows clinicians to identify relapse risk categories for ALL and stratify the chemotherapy according to well-established adult or pediatric therapeutic protocols.1–7 Results of MRD studies can also be used to select treatment intensity and duration, and estimate the optimal timing for hematopoietic stem cell transplantation (HSCT) in childhood ALL.8
Both multiparametric flow cytometry (MFC) and the amplification of immunoglobulin/T cell receptor (Ig/TCR) genes by polymerase chain reaction (PCR) have similar results in MRD detection with a level of 10−4 cells. However the best time points for detection are different between the two techniques.
Clinical significance of minimal residual disease levelsThe goals of MRD studies for clinical purposes are to establish: (i) the levels of MRD that are relevant to the therapeutic decision; (ii) the most informative time points during treatment; and (iii) the clinical relevance of information that each method provides at the different time points.
The cut-off value to define ALL MRD positivity is 0.01% or 10−4 cells, because this represents the limit of detection by immunophenotyping and molecular assays, although it is possible to achieve a higher sensitivity (better than 0.01%) by PCR techniques. Moreover, with the recent improvements in technology, this threshold can now be achieved by flow cytometry.8,9 Currently, therapeutic protocols establish a cut-off point at the most informative time to predict danger of relapse according to the appropriate methodology employed for MRD detection (Table 1).
Clinical significance of MRD, cut-off levels and time points of detection during induction therapy in acute lymphoblastic leukemia.
| Reference | Therapeutic protocol | Cut-off level (%) | Method | Time point (induction therapy) | Outcome and therapy |
|---|---|---|---|---|---|
| Cavé H et al. 1998 | EORTC | >0.1 | IgTCR | end of induction | 16× higher relapse rate |
| Zhou J et al. 2007 | Dana-Farber | >0.1 | IgTCR | D30 | 10,5× higher relapse rate |
| Borowitz MJ et al. 2008 | COG | >0.01 | MFC | D29 | worst EFS |
| Flohr T et al. 2008 | AEIOP/BFM 2000 | ≥0.01 | IgTCR | D33 and D78 | high relapse rate |
| Campana D, 2009 | St Jude's | ≤0.01>1≥0.01>1 | MFC/PCR | D15D15D42D42 | low risk -less intensive therapyintensive inductionhigh-riskHSCT |
| Gaipa G et al. 2012 | AEIOP/BFM 2000 | ≤0.01 | MFCIgTCR | D15D33 and D78 | EFS91,6% (5 years) |
| Brüggemann M et al. 2012 | GMALL | <1,0×10−4 | MFC/IgTCR | D71,w16/w30/w52 | Treatment reductionhigh-risk |
| >1,0×10−4 reconversion | <1 year of treatment | HSCT or experimental therapies | |||
MRD, minimal residual disease; MFC, multiparametric flow cytometry; Ig, immunoglobulin; TCR, T-cell receptor; PCR, polymerase chain reaction; EFS, event free survival; HSCT, hematopoietic stem cell transplantation.
The identification of the disease relapse risk allows therapeutic stratification and better clinical management, including recognition of patients who require less intensive therapy and those eligible for HSCT at first remission.5,10
The level of MRD in pediatric patients prior to conditioning for allogeneic HSCT has a significant impact on post-transplant outcomes and it is the most important predictor of relapse after HSCT. Patients with high-level MRD at the time of transplant (>10−3 or 0.1% malignant cells) have significantly poorer outcomes than those who entered the transplantation with negative MRD (<10−3 cells).11 The Acute Lymphoblastic Leukemia Berlin-Frankfurt-Münster Stem Cell Transplantation Group (ALL-BFM-SCT) 2003 trial assessed MRD in the bone marrow (BM) at Days 30, 60, 90, 180, and 365 after HSCT and each time point with a MRD ≥10−4 leukemic cells was consistently correlated with shorter event free survival.12
Two techniques are available for post-transplant monitoring of disease remission: MRD detection and the characterization of post-transplant chimerism. The MRD detection techniques search for the malignant clone, while assessments of chimerism characterize the origin of post-transplant hematopoiesis.11 The sensitivity of investigations of chimerism vary greatly depending on the method used.13
Patients with a low MRD level after HSCT (<10−3), can convert mixed chimerism to complete chimerism by pre-emptive immunotherapy,11,14,15 which demonstrates the importance of MRD monitoring after HSCT. Although there is not a well-established management schedule for these cases, MRD status provides a real perspective of rational therapeutic intervention after HSCT to prevent recurrence of the disease.14
Methods of minimal residual disease detectionThe most reliable methods of evaluating MRD are MFC analysis with the identification of leukemia-associated immunophenotypes (LAIPs) and amplifying antigen-receptor (Ig/TCR) gene rearrangements and fusion transcripts by PCR. Both MFC and amplification of Ig/TCR genes by PCR provide similar results at a MRD level of 0.01%,5,16 and both MFC and PCR have advantages and disadvantages. MFC is a rapid method, useful in >95% of ALL cases and is more informative than PCR during the first phase of induction therapy, while PCR is preferable for studies after HSCT or at the end of therapy because of its high sensitivity in those moments.10,17 During the first 2–3 weeks of remission-induction therapy, BM specimens do not contain lymphoid progenitors, and so the detection of immature B-cells by MFC can be an indication of residual disease.17
The most important causes of discrepancy between MFC and PCR assays are: (i) samples containing a limited cell number for MFC assays; (ii) phenotype variations of regenerating precursor B-cells (PBC) in BM during therapy and related to age; (iii) drug induced antigenic modulation; (iv) quality of PCR clonal markers; (v) amplification of nonspecific DNA from dead cells; and (vi) oligoclonality and clonal evolution.6,18–20
The main disadvantages of Ig/TCR rearrangement investigations are: (i) they are labor intensive and time consuming; (ii) require extensive experience and knowledge concerning the different types of Ig/TCR gene rearrangements; (iii) real-time PCR technology is demanding because of the design and sensitivity of testing using specific probe-prime sets for individual PCR targets21; and (iv) there are subclones with distinct clonal Ig/TCR gene rearrangements that are undetected at diagnosis and that may become predominant during the course of the disease (oligoclonality).22 Because of these disadvantages, many laboratories try to use MFC for MRD detection,21 although new approaches of sequencing technologies are of great potential for facilitating molecular MRD studies in ALL and may well supplant the current method.23
ImmunophenotypingDetection of MRD by MFC consists of searching for LAIPs, also called aberrant phenotypes, that are absent in normal, reactive or regenerating BM and peripheral blood cells; this is useful to discriminate neoplastic cells from normal hematopoietic cells. LAIPs include the presence of cross-lineage antigen expression (e.g. expression of myeloid antigens in ALL cases), asynchronous patterns of expression of maturation markers (e.g. surface Ig expression on CD34+ cells) and abnormal levels of expression of individual markers (e.g. antigen overexpression or underexpression). LAIPs are identified in more than 95% of ALL cases.5,17 Thus, MFC can be used to monitor 90–95% of MRD in ALL cases during therapeutic management. Importantly MRD can be used with PB samples in patients with T cell ALL giving similar results to the use of MRD testing in BM. However in patients with B-lineage ALL, MRD is usually present at higher levels in BM than in PB;8 BM is preferable for MRD detection in this situation.
The sensitivity of this method varies according to the number of MFC colors applied in MRD assays: 10−3 to 10−4 MRD cells with 3–4 colors and 10−4 to 10−5 with >6 colors.9 New ways of sample preparation such as bulk lysis24,25 and improvements in analysis strategies can also contribute to increase MFC sensitivity.9 Although these improvements can be achieved in MRD detection, several studies demonstrated that MRD monitoring by four-color MFC can still be clinically informative.3,26
The principal advantages of immunophenotyping are: (i) the possibility of evaluating the sample cellularity and the degree of hemodilution; (ii) the maturation of normal BM cells, including lymphoid recovery after immunosuppressive therapy; (iii) the speed of obtaining results; and (iv) its wide-ranging applicability.
The limitations of immunophenotyping in MRD studies are: (i) the low number of cells available; (ii) the similarity of the immunophenotype between normal precursor cells and leukemia cells hinders the identification of residual blast cells; (iii) the modulation of antigen expression during treatment18; (iv) the necessity of high expertise to perform MRD assays; and (v) the lack of inter-laboratorial standardization and quality control.
Immunophenotypic modulation, described in ALL patients,5,19,27 interferes in the ability to accurately determine MRD (Table 2). Some modulations of B cell antigen expressions induced by glucocorticoid therapy19 occur during the first 15 days of treatment and persist until Day 33 of induction therapy. They are characterized by down-modulation of CD10 and CD34 expression and up-modulation of CD19, CD20, CD45RA and CD11a, while the expression of CD58 is not significantly changed compared to levels at diagnosis, either in BM or in PB samples. At Day 78, after stopping glucocorticoid therapy, there is a reversion of CD10 and CD34 expression to initial levels and the CD58 expression stablizes.18,19,28 Significant changes in forward-angle light scatter (FSC) and side angle light scatter (SSC) signals associated with blast cells at diagnosis and at Day 15 are not observed.18
Common modulation of antigen expression during acute lymphoblastic leukemia treatment.
| B precursor cell ALL | T cell ALL |
|---|---|
| Induction therapy (until Day 33)Down-modulation of CD10 and CD34Up-modulation of CD19, CD20, CD45RA and CD11a | Induction therapyDown-modulation of TdT, CD99, CD34 and CD10 |
| At Day 78 of inductionReversion of CD10 and CD34 to initial expression |
Roshal et al. also described down-modulation of immaturity markers such as TdT, CD99, CD34 and CD10 in T-ALL cells during induction therapy. They did not observe intensity variations in CD2, CD3, CD4, CD5, CD7, and CD8, and CD45 showed a slight gain in mean fluorescence intensity compared to normal T cells.27
Furthermore immunophenotypic changes have been reported in relapsed acute leukemia by clonal selection or lineage switch.26 The changes in LAIPs can affect the accuracy of the flow cytometric detection of MRD rendering false negative results. The use of multiple marker combinations can minimize false negative results suggesting that this should be a strategy for MRD detection by immunological methods. Thus, the use of new markers for overexpressed or underexpressed PBC ALL compared to normal PBC including CD24, CD44, CD49f, CD69, CD72, CD73, CD79b, CD86, CD97, CD99, CD102, CD123, CD130, CD164, CD200, CD300a, CD304, BCL2, HSPB1, PBX1, CTNNA1, and ITGB7 is promising to improve sensitivity of immunophenotype MRD studies.29 In addition, some of these markers are associated to genetic abnormalities, and have been proved to be stable after treatment.29
Detection of minimal residual disease in acute lymphoblastic leukemia by multiparametric flow cytometry – a proposal of standardizationMFC and amplification of Ig/TCR genes by PCR have similar results at a MRD level greater than 0.01% cells6,30 but the introduction of MFC with six or more colors, the standardization of instrument settings and immunophenotyping protocols,24 the availability of a robust single multicolor antibody combination, and novel data analysis strategies,9 may contribute to improve the potential of MFC in the diagnosis of MRD.21 The type of laboratory expertise available to a cancer center or a cooperative group could be the most important factor in determining which method should be used.8
In Brazil, as in other countries, there are flow cytometry laboratories in most leukemia treatment centers, making this method more readily available.
The MRD Working Group of the SBTMO was created with the aim of standardizing MFC for MRD investigations and to offer reliable and reproducible results that ensure quality in clinical application and patient care.
MethodsInitially all members of the Working Group reviewed the literature data; they also evaluated 20 list-mode of normal and regenerating BM of adult and pediatric samples which were provided by eight participating centers and available online.
The proposals to standardize MFC presented in this article are based on reported data and relevant information collected from the expertise of the participating centers. They include: (i) protocols for sample preparation and staining, (ii) standardization of monoclonal antibodies (MoAbs) and respective fluorochromes, combined in four-color marker panels, (iii) standardization of MFC acquisition protocols and (iv) quality control issues.
According to the Brazilian Group of Flow Cytometry (GBCFLUX) data, most Brazilian MFC laboratories are today equipped with cytometers with three and four fluorescence sets. Recently, GBCFLUX published diagnostic panels for acute leukemia recommended to most Brazilian MFC laboratories.31
The next steps will be to train Working Group members to support the standardization process and evaluate reproducibility through online interchange of MFC data files to analyze MRD cases as a group. Data analysis is not the goal of this work and should be addressed in a future paper.
Minimal residual disease working group recommendationsGeneral recommendationsCell morphology should be assessed visually using conventional optical microscopy. Smears of samples collected in tubes containing ethylenediaminetetraacetic acid (EDTA) are also analyzed to estimate the hemodilution parameter. The smears are internal controls of the laboratory to verify the cellularity of the sample to be processed. Nonetheless, ethically, all samples must be processed, including hemodiluted samples. BM (1–2mL) or PB samples must be collected in K3 EDTA (7.5%) for both MFC and a complete blood count. The storage of samples should not exceed 24h after collection (Table 3).
Summary of technical proceedings.
| General recommendations |
| Cell morphology of corresponding sample |
| Evaluation of sample cellularity/hemodilution assessed by smears from ethylenediaminetetraacetic acid (EDTA) tube |
| Bone marrow (1–2mL) or peripheral blood samples must be collected in K3 EDTA 7.5% for both multiparametric flow cytometry and complete blood count |
| The incubation of samples should not exceed 24h after collection |
| Recommendation for sample preparation |
| Stain-and-then-lyse technique or bulky lysis and stain |
| Samples incubated for 15min at room temperature in the dark with fluorochrome conjugated monoclonal antibodies |
| Lyse of non-nucleated red cells with lysing solution |
| Centrifuge and wash twice with PBS or 0.2% PBS–BSA or 0.2% PBS+BSA plus 0.1% sodium azide |
| Re-suspend in 300–500μL of PBS for multiparametric flow cytometry acquisition and analysis |
| Intracellular staining must be performed after staining for cell surface membrane markers, utilizing permeabilizing solutions |
| Standard operational procedures |
| Daily cleaning and bead calibration procedures |
| Compensation must be done monthly or when required, according to the stability of flow cytometer parameters |
| Routine preventive maintenance must be performed at least every six months |
PBS: phosphate buffer solution; BSA: bovine serum albumin.
Most laboratories of the MRD Working Group that use MFC prepare samples by the conventional stain-and-then-lyse technique or bulk lysis and stain.25 One laboratory uses mononuclear cells separated using the Ficoll-Hypaque method5 according to requirements of the specific treatment protocol.
For the conventional technique, fresh BM or PB samples contain 106 cells, 10–100μL white blood cells must be incubated for 15min at room temperature in the dark, with pre-titrated saturating amounts of four-color combinations of fluorochrome conjugated MoAb – fluorescein isothiocyanate (FITC); phycoerythrin (PE); peridinin-chlorophyll-protein (PerCP); peridinin-chlorophyll-protein cyanine 5.5 (PerCPCy5.5); allophycocyanin (APC) (Table 3). As an optional step, an additional aliquot containing an unstained sample may be processed in parallel as a negative control. Non-nucleated red cells can be lysed using FACS Lysing solution (Becton-Dickinson Biosciences -BDB™, San Jose, CA, USA) or Excellyse Easy (Exbio™, Vestec, Czech Republic), according to the manufacturer's instructions. The remaining cells are sequentially centrifuged (500g) for 5min, washed twice in phosphate buffered saline (PBS: pH 7.4) or PBS plus 0.2% bovine serum albumin (BSA: pH 7.4) or PBS plus 0.2% BSA plus 0.1% sodium azide: pH 7.4) and re-suspended in 300–500μL in PBS for MFC acquisition and analysis. Intracellular staining for CD3 and TdT is performed after staining for cell surface membrane markers using Fix&Perm solution (Invitrogen™, Camarillo, CA, USA or An Der Grub™, Vienna, Austria) or the Intra Stain kit (Dako™, Carpinteria, CA, USA) as per the instructions of the manufacturer. The recommended solutions have been tested, applied and selected for use in most of the laboratories of the Working Group.
Standard operational proceduresDaily cleaning and calibration of bead procedures are recommended and compensation should be done every month or when required according to stability of flow cytometer parameters. Flow cytometer performance must be checked every day or according to the manufacturer's recommendations to ensure that the evaluation of samples always uses the same parameters and enable an accurate analysis of the underexpression and overexpression of markers which is very important for MRD detection. Routine preventive maintenance must be performed periodically, that is, at least every six months (Table 3).
Fluorochrome selection for four-color panelsThe selection of the most appropriate combination of fluorochromes for four-color panels should allow simultaneous usage of backbone markers aimed at the identification of the cell populations of interest and additional antibody markers devoted to a more detailed characterization of the leukemic cell populations such as maturation markers, cross-lineage markers, and markers associated with molecular lesions. A combination of FITC, PE, PerCP or PECy5.5 and APC were selected based on the literature and the expertise of the Working Group.
Immunophenotypic abnormalities of leukemic B cell populations are identified by the deviation from normal patterns of B-lymphoid development9. PBC or hematogones have morphologic and immunophenotypic similarities to neoplastic lymphoblasts. PBC may be present in large numbers in many situations as early as infancy, or in a variety of diseases both in childhood and in adult life, as in some autoimmune and congenital cytopenias, neoplasms and acquired immunodeficiency syndrome (AIDS).32 Hematogones also may be particularly prominent in regenerating BM following chemotherapy or HSCT (Figure 1).32–35 Particularly following ALL treatment, hematogones are often expanded in BM and can potentially be mistaken for residual disease. Some studies showed that the PBC population always expresses a continuous and complete maturation spectrum by four-color flow cytometry.36 In contrast, cases of PBC ALL frequently show a different spectrum to normal B-lineage maturation. These differences include: maturation arrest; overexpression, underexpression, and asynchronous expression of antigens observed in PBC and often the expression of myeloid-associated antigens.33,37
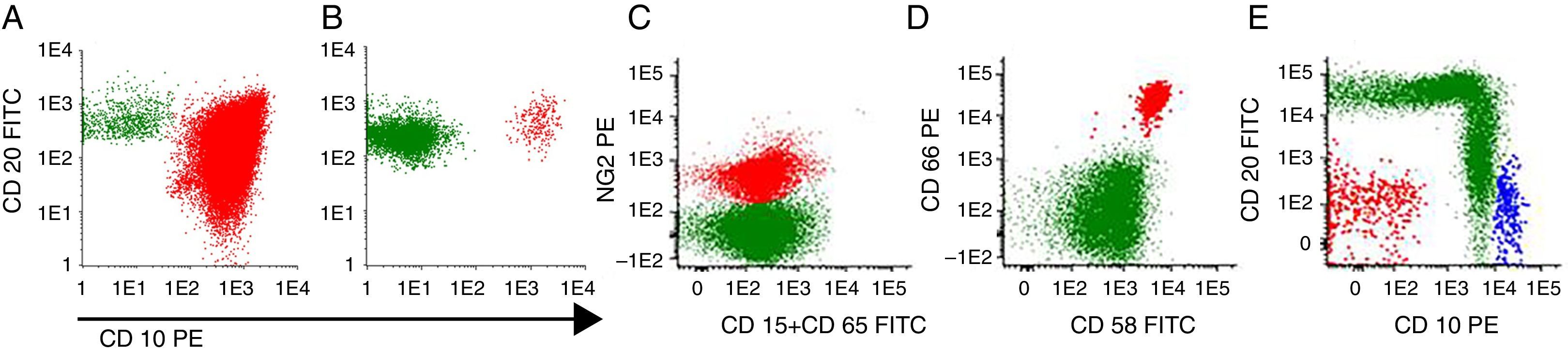
Minimal residual disease in precursor B-cell acute lymphoblastic leukemia using maturation tube: CD20FITC/CD10PE/CD19PerCP/CD34APC. (A) At diagnosis (77.6% of blast cells) and (B) the same patient on Day 15 of induction therapy with positive minimal residual disease (0.03%). (C) MLLAF4 precursor B-cell acute lymphoblastic leukemia with positive minimal residual disease (0.28%) on Day 40 after hematopoietic stem cell transplantation. (D and E) BCR-ABL positive precursor B-cell acute lymphoblastic leukemia with positive minimal residual disease (0.32%) before conditioning treatment for hematopoietic stem cell transplantation. Gate in CD 19+ cells. In green: mature B-cells (A–C), normal precursor and mature B-cells (D and E). In red: blast cells. In blue: normal CD 34+ precursor B-cells. Acquisition: 1,000,000 of total events. Method: bulk lysis.
According to this MRD Working Group consensus, residual B-cell ALL must be investigated in BM and identified by two backbone markers in a four-color MoAb panel, such as CD19 and CD34.
The mandatory panel for B-cell ALL MRD detection (Table 4) is addressed to identify deviations in the maturation pathway of B-cells and verify alterations in the antigen expression patterns: Tube 1: CD20FITC/CD10PE/CD19PerCP or PEcy5.5/CD34APC (Figure 1), Tube 2: CD45FITC/CD34PE/CD19PerCP or PEcy5.5/CD38APC and Tube 3: nTdTFITC/CD10PE/CD19PerCP or PEcy5.5/CD34APC.
Fluorochrome conjugated antibody panels used for minimal residual disease detection in B precursor cell-acute lymphoblastic leukemia by multiparametric flow cytometry.
| Mandatory panel |
| Tube 1 – CD20FITC/CD10PE/CD19PerCP or PEcy5.5/CD34APC |
| Tube 2 – CD45FITC/CD34PE/CD19PerCP or PEcy5.5/CD38APC |
| Tube 3 – nTdTFITC/CD10PE/CD19Percp or PEcy5.5/CD34APC |
| Recommended tubesa |
| Tube 4 – CD81FITC/CD66cPE/CD19PerCP or PEcy5.5/CD34 APC |
| Tube 5 – CD45FITC/CD123PE/CD19PerCP or PEcy5.5/CD34APC |
| Tube 6 – CD15FITC and CD65FITC/NG2PE/CD45PerCP/CD19APC |
| Optional markersa |
| CD13 and/or CD33 PE, CD58FITC, CD9FITC/CD25PE, CD22PE |
n: nuclear staining.
Recommended tubes are intended to recognize: (i) markers that are frequently underexpressed in B cell ALL compared to normal B-cells such as CD81; (ii) cross-lineage markers such as CD15, CD65, CD66c, CD123; and (iii) markers associated with molecular lesions such as CD66c [in some cases presenting the breakpoint cluster region-Abelson murine leukemia (BCR-ABL) fusion protein] and NG2 (associated with 11q23 alterations); this latter one is often expressed concomitantly to CD15 and/or CD65 (Figure 1).
Optional markers are: CD9 and CD22 that are expressed in B normal cells and often underexpressed in their leukemic counterparts; CD58 that has been shown to be overexpressed in leukemic blasts when compared to their normal counterparts,28 CD13 and CD33 (myeloid markers) as cross-lineage markers and CD25 (interleukin 2 receptor) can also be associated with the presence of BCR-ABL positive PBC ALL. It must be emphasized that recommended and optional markers should be chosen according to their expression at diagnosis.
MRD detection of T-ALL in the PB or BM is theoretically easier as most stages of normal T lymphocyte maturation occur in the thymus. Therefore the presence of an immature T cell subset in the PB or BM should be considered aberrant. For the investigation of MRD in T-cell ALL, CD3 and CD7 are recommended as backbone markers (Table 5). Mandatory and recommended tubes are addressed to identify maturation stage of blast cells and include immaturity markers such as TdT, CD34, CD1a, and CD99 (Figure 2). Difficulties in MRD detection in T-ALL largely stem from the loss of immaturity markers on the abnormal blast population following induction chemotherapy. Optional markers for T-ALL MRD aim to recognize cross-lineage markers such as CD13 and CD33; a marker that is underexpressed or overexpressed in 81% of T-ALL cases such as CD44,29 and CD117, expressed in early T-ALL. These markers may be useful for MRD detection when they are expressed at diagnosis.
Fluorochrome conjugated antibody panels used for minimal residual disease detection in T cell-acute lymphoblastic leukemia by multiparametric flow cytometry.
| Mandatory panel |
| Tube 1 – cyCD3FITC/mCD3PE/CD45PerCP/CD7APC |
| Tube 2 – nTdTFITC/CD2PE/CD5PerCP/CD7APC |
| Recommended tube |
| Tube 3 – CD1aFITC/CD99PE/mCD3PerCP/CD7APC |
| Optional markersa |
| CD10PE, CD13PE, CD33PE, CD 34 PE, CD44PE, CD117PE |
cy: cytoplasmic staining; n: nuclear staining; m: membrane staining.
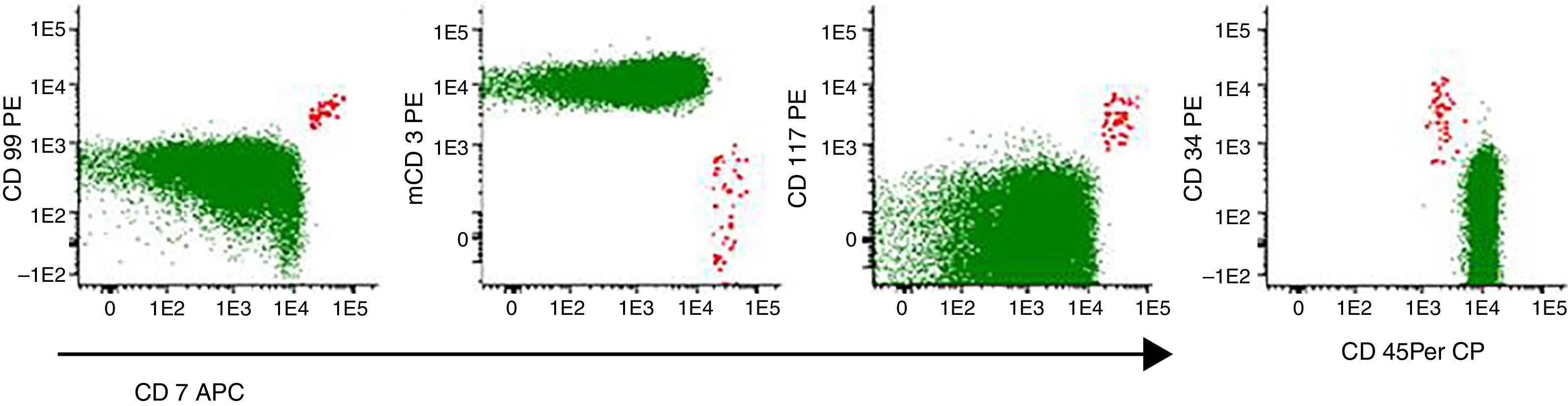
Minimal residual disease positive (0.01%) in early T-cell acute lymphoblastic leukemia without previous immunophenotyping. Evaluation before hematopoietic stem cell transplantation. Gate in CD7+ cells. In green: mature T cells. In red: blast cells. Acquisition: 1,000,000 of total events. Method: bulk lysis.
Data acquisition must be performed in sequence immediately after sample preparation is completed. For each sample aliquot, a minimum of 500,000 and maximum of 1,000,000 events must be acquired. Optionally, laboratories that perform bulk lysis are able to acquire 5,000,000 events. A criterion for quantifiable MRD positivity was established using a detection limit of absolute MRD cell counts of 10 cells or more in each tube.38
ConclusionMFC is a powerful method for MRD investigations of hematology malignancies, but it is fundamental to have good standardization of the pre-analytical, analytical and post-analytical processes. The MRD Working Group recommendations meet this requirement with the main goal being the patients’ safety and care. For this purpose, it also should be stressed that the MFC and PCR techniques are complementary, and so it is necessary that more molecular biology laboratories with expertise in Ig/TCR assays are available in Brazil.
Conflicts of interestThe authors declare no conflicts of interest.
The authors thank the colleagues who contributed to this work by sending data from their laboratories: Alex Freire Sandes (Divisão de Hematologia do Grupo Fleury, São Paulo, SP); Elizabeth Delbuono (GRAAC, São Paulo, SP); Leandro S Thiago (Instituto Nacional do Cancer, Rio de Janeiro, RJ); Maria Mirtes Sales (Laboratório de Citometria de Fluxo do Hospital das Clinicas, Faculdade de Medicina Universidade de São Paulo, SP).
The authors especially thank Dr Lucia Silla, president of SBTMO, Dr Nelson Hamerschlak coordinator of SBTMO working groups and Dr. Vergilio A Rensi Colturato, who conceived the group, for supporting the development of the group.
Adriana Seber, Ana Paula Alegretti, Ana Paula de Azambuja, Cintia G F Machado, Elaine Sobral da Costa, Elizabeth Xisto Souto, Irene G H Lorand-Metze, Maria Luiza Menezes Cortez, Mariester Malvezzi, Maura Rosane Valério Ikoma, Mihoko Yamamoto, Míriam Perlingeiro Beltrame, Norma Lucena-Silva, Nydia Strachman Bacal, Silvia Ines Alejandra Córdoba Pires Ferreira, Vergílio Antonio Rensi Colturato, Virginia Pires.



