
Aplastic anemia (AA) is a rare disorder characterized by suppression of bone marrow function. It can develop as the result of congenital marrow disease and chemical exposure; however, most cases are idiopathic.1 Treatment with immunosuppressive therapy (IST) for patients who do not have an human leukocyte antigen (HLA)-compatible donor relies on the evidence that a deregulated immune system drives T lymphocytes to cytokine-mediated destruction of their own hematopoietic stem cells.1 The majority of these patients respond well to up-front administration of IST, including anti-thymocyte globulin (ATG) and cyclosporine (CsA), which is successful in around 80%.2 Unfortunately, ATG and CsA can lead to clonal disorders, in particular myelodysplastic syndrome (MDS) and paroxysmal nocturnal hemoglobinuria.3 On the other hand, high doses of cyclophosphamide (HDCY) have been administered as a sole immunosuppressive agent in severe aplastic anemia (SAA), principally in adults, with no late clonal disorders reported after up to ten years of follow up.4 However, late complications following HDCY, including lasting neutropenia and severe fungal infections have been reported mainly in adults, but no similar late complications have been reported for patients who received HDCY during childhood.
We report the first case of a boy with SAA treated successfully with HDCY who after 15 years developed MDS that rapidly evolved into acute myeloid leukemia (AML), and who was treated unsuccessfully with a hematopoietic stem cell transplant (HSCT).
Case reportA five-year-old boy was diagnosed in 1997 with SAA after a short clinical period of fatigue, anemic syndrome and mucocutaneous bleeding, and findings consistent with SAA in his complete blood count (Table 1).1 Bone marrow aspirate (BMA) and biopsy examinations showed a hypoplastic specimen without megakaryocytes, with less than 15% cellularity and no dysplastic changes; cytogenetic studies were not available in our center at diagnosis. A test for hypersensitivity of Fanconi anemia (FA) cells to diepoxybutane, the diepoxybutane (DEB) test, which helps early diagnosis of FA5 was not performed. The patient had no HLA-compatible donor and, at that time, therapy with ATG plus CS was not available in our country. The patient was part of a group of five children with SAA treated with HDCY under these circumstances; the results of that trial have been published.6 The treatment protocol consisted of cyclophosphamide (CY) at 50mg/kg/day administered intravenously (IV) over 1h on four consecutive days with a total dose of 200mg/kg, plus granulocyte colony stimulating factor (G-CSF) at 5¿g/kg/day, administered subcutaneously from Day +1 post-HDCY until an absolute neutrophil count (ANC) >1×109/L was reached. The patient achieved complete hematological remission, and remained free of transfusion requirements with no infections. No dysplastic or clonal hematological disorders developed over 15 years of follow-up. Fifteen years after HDCY, this patient presented with severe anemia and he was treated with packed red blood cell transfusions, folic acid (5mg/day) and danazol (200mg b.i.d.). Three months later, classical findings of myelodysplasia were documented in peripheral blood and bone marrow, including hypercellular bone marrow with a significant increase in the number of micromegakaryocytes and reticulin fibrosis Grade 3. Five months later, the MDS progressed to alpha-naphthyl butyrate esterase-positive acute myeloblastic leukemia (AML-M5). The bone marrow immunophenotype demonstrated cells with CD4, CD11b, CD16, CD36, CD56, CD64, and HLA-DR antigenic specificities.
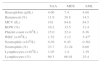
Complete blood count at diagnosis, during myelodysplasia and after progression to acute myeloid leukemia (AML) of a severe aplastic anemia patient treated with high-dose cyclophosphamide who suffered late clonal evolution after 15 years of follow-up.
| SAA | MDS | AML | |
|---|---|---|---|
| Hemoglobin (g/dL) | 4.00 | 7.4 | 4.88 |
| Hematocrit (%) | 11.9 | 20.8 | 14.5 |
| MCV (fL) | 101 | 84.6 | 84.5 |
| RDW (%) | 16.2 | 13.5 | 11.4 |
| Platelet count (×109/L) | 15.0 | 22.4 | 6.36 |
| WBC (×109/L) | 1.52 | 2.12 | 5.47a |
| Neutrophils (×109/L) | 0.36 | 0.45 | 0.361 |
| Neutrophils (%) | 23.7 | 21.24 | 6.60 |
| Lymphocytes (×109/L) | 1.05 | 1.4 | 1.39 |
| Lymphocytes (%) | 69.3 | 66.01 | 25.4 |
SAA: severe aplastic anemia; MDS: myelodysplastic syndrome; AML: acute myeloid leukemia; MCV: mean corpuscular volume; RDW: red cell distribution width; WBC: white blood cell count.
Important hematologic data at the time of myelodysplasia and after AML are shown in Table 1.
Standard AML chemotherapy was started, including cytarabine for seven days plus mitoxantrone for three days. It was decided to perform haploidentical stem cell transplantation fourteen days after the diagnosis of AML because of the persistence of blasts in the peripheral blood and due to the background and poor prognosis. A reduced-intensity conditioning (RIC) regimen was administered 45 days after the end of induction consisting of cyclophosphamide, fludarabine, and busulfan. Haploidentical HSCT was performed on Day +6 of conditioning using his mother as donor. He presented neutropenia and fever on the same day as the procedure, and antibiotics were administered with no improvement. Hematuria and melena developed requiring intensive transfusion support. Pneumonia unresponsive to treatment was followed by cardiopulmonary arrest and death two days after transplant.
DiscussionThe treatment of choice for SAA patients who have a matched sibling donor is HSCT with survival rates of up to 90%.1 Front-line matched unrelated donor appears to be a viable option in children, with similar overall survival and event-free survival to transplants with matched sibling donors. A matched unrelated donor HSCT after failure of IST has proved to be a very good rescue strategy.7 As in our case, most SAA patients lack a suitable donor and, in the absence of IST, mortality is 75%.8 Currently, a response rate of 44–80% with a three- to five-year survival rate ranging from 81 to 93% for SAA patients immunosuppressed with ATG plus CsA and granulocyte-colony stimulating factor (G-CSF) has been reported.2 AA patients, however, can have a partial response, fail to respond, relapse, or remain dependent of CsA. In order to circumvent these shortcomings, alternative IST, such as alemtuzumab, as well as promising agents, including eltrombopag, are currently being investigated.
Successful immunosuppressive treatment of SAA with ATG and CsA has been associated with late clonal disorders, including paroxysmal nocturnal hemoglobinuria and MDS.3 High dose cyclophosphamide has also been successfully administered in SAA, mostly in adults, with no such late clonal disorders reported after a decade of follow up.4 There is however, evidence for late complications following HDCY, including lasting neutropenia and severe fungal infections.4 These adverse long-term events have not been reported for patients who received HDCY during childhood. A recent study focusing on the outcomes of pediatric patients with AA found clonal evolution and disease progression to MDS in five patients out of 149 (3%) that had moderate AA.2 Our patient had a stable course with good quality of life for 15 years after successful treatment with HDCY; he then evolved to severe MDS shortly followed by AML, treated unsuccessfully with chemotherapy and followed by a matched related donor HSCT that was complicated by sepsis leading to death.
In conclusion, HDCY for children with SAA who do not have a suitable hematopoietic stem cell donor and no access to standard therapy with ATG plus CsA can lead to long-term hematopoietic regeneration. However, as this case exemplifies for the first time in this age group, late clonal evolution employing high doses of this powerful immunosuppressant agent can lead to MDS and AML.
We thank Sergio Lozano-Rodriguez, M.D. for his review of the manuscript.



