

To assess the impact of the distance education course “Sickle Cell Disease: Primary Health Care Line” on knowledge acquisition of professional healthcare providers.
MethodsA cross-sectional study was conducted with a quantitative approach at the Educational and Support Center for Hemoglobinopathies (Cehmob-MG), state of Minas Gerais, Brazil, in 2016. One hundred and fifty-three out of 300 professional healthcare providers were invited to participate in the proposed distance course. Of the participating professional healthcare providers, 72 (47%) successfully concluded the course (Group A), whereas 81 (53%) did not complete their course assignments and did not meet the minimum requirements for regular attendance (Group B). Knowledge acquisition was assessed with the Knowledge of Sickle Cell Disease Instrument, DFConhecimento, applied using the web tool eSurv. Univariate analysis by Poisson regression was employed to assess the influence of sociodemographic variables on the DFConhecimento score and to select variables to compose the initial multivariate regression model (p-value<0.20). The analysis was performed in the statistical programming environment R.
ResultsThe average score was 9.76 for Group A and 6.54 for Group B. The two groups were considered statistically different (p-value<0.05) for all items with the proportion of correct items being greater in Group A. Professional healthcare providers who concluded the course had a significantly higher DFConhecimento score (45%) when compared to those who did not successfully conclude the course.
ConclusionParticipation in a distance education course on sickle cell disease had a positive impact on the acquisition of knowledge about the disease by professional healthcare providers.
Considered a public health problem, sickle cell disease is a hereditary condition of great importance globally and in Brazil. It predominantly affects the Black population and presents clinical manifestations within the first years of life with repercussions on morbidity and mortality.1,2 Despite technological and scientific advances to improve the prognosis of sickle cell disease, its management persists as a challenge for professional healthcare providers, since it involves complex aspects of diagnosis, treatment and prevention of complications.3–5
Studies point to insufficient knowledge of professional healthcare providers about important aspects of the quality of life of people with sickle cell disease, such as growth and developmental consultations, immunization, school performance, use of folic acid, prophylactic antibiotic therapy, complications due to vaso-occlusion, transfusions, prevalence of iron overload, strokes in children and screening of stroke risk using transcranial Doppler ultrasonography.2,6–9 In order to improve the quality of care provided to people with sickle cell disease and to reduce morbidity and mortality rates, there is a clear need to develop educational interventions to increase knowledge of professional healthcare providers about sickle cell disease.3,10–12
To that end, a distance education course entitled “Sickle Cell Disease: Primary Health Care Line” has been offered by the Educational and Support Center for Hemoglobinopathies (CEHMOB-MG) of the state of Minas Gerais since 2010. The purpose of the course is to build competence of professionals and to improve the quality of care for people with sickle cell disease.2,3
Distance education is considered an important tool in the dissemination of up-to-date knowledge and information, especially in emerging countries. Its educational resources allow interaction, shared experience, improvement of knowledge in different health areas and can affect a large number of professionals in different regions of the country. In addition, studies have demonstrated the effectiveness of this approach by educational interventions targeting professional healthcare providers.13–16 Despite the relevance of distance courses, no studies were found in the literature that investigate the impact of distance education on the management of sickle cell disease.
This study aims to evaluate the impact of the distance education course “Sickle Cell Disease: Primary Health Care Line” on knowledge acquisition by professional healthcare providers.
MethodsThis is a cross-sectional study with a quantitative approach carried out from April to June 2016 at the Educational and Support Center for Hemoglobinopathies (Cehmob-MG) in the state of Minas Gerais.
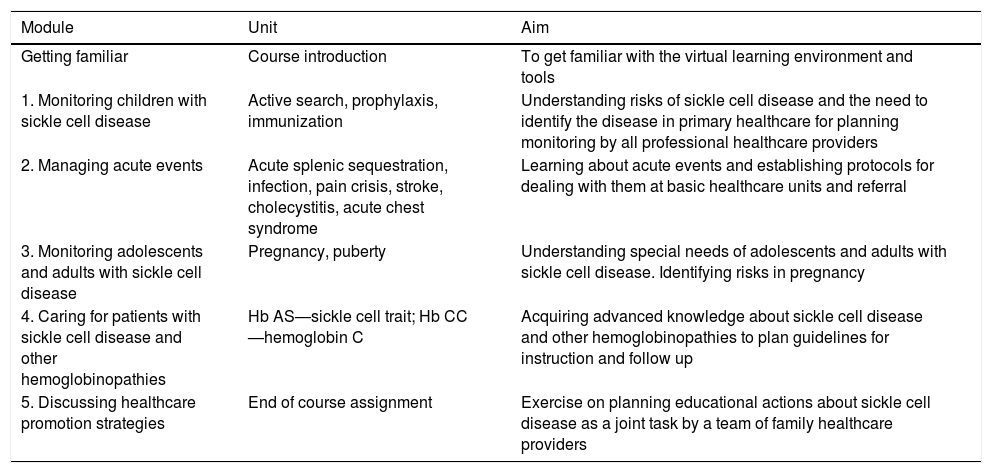
The distance education course “Sickle Cell Disease: Primary Health Care Line” aims at promoting an educational strategy to improve knowledge within a virtual learning environment. The course workload is 95h over three months with follow-up sessions managed by tutors with expertise in sickle cell disease. The course content is divided into modules dealing with topics related to health surveillance actions targeting children, adolescents and adults, management of acute events, sickle cell behavior and other hemoglobinopathies (Table 1). Content is developed through student engagement in case study analysis, discussion forums and group activities with debate and reflection on the provision of professional care, leading to knowledge construction and proposals to improve the quality of care for people with sickle cell disease.
Modules, units and aims of the distance course “Sickle Cell Disease: Primary Health Care Line”.
| Module | Unit | Aim |
|---|---|---|
| Getting familiar | Course introduction | To get familiar with the virtual learning environment and tools |
| 1. Monitoring children with sickle cell disease | Active search, prophylaxis, immunization | Understanding risks of sickle cell disease and the need to identify the disease in primary healthcare for planning monitoring by all professional healthcare providers |
| 2. Managing acute events | Acute splenic sequestration, infection, pain crisis, stroke, cholecystitis, acute chest syndrome | Learning about acute events and establishing protocols for dealing with them at basic healthcare units and referral |
| 3. Monitoring adolescents and adults with sickle cell disease | Pregnancy, puberty | Understanding special needs of adolescents and adults with sickle cell disease. Identifying risks in pregnancy |
| 4. Caring for patients with sickle cell disease and other hemoglobinopathies | Hb AS—sickle cell trait; Hb CC—hemoglobin C | Acquiring advanced knowledge about sickle cell disease and other hemoglobinopathies to plan guidelines for instruction and follow up |
| 5. Discussing healthcare promotion strategies | End of course assignment | Exercise on planning educational actions about sickle cell disease as a joint task by a team of family healthcare providers |
To recruit participants, local and regional authorities are contacted and alerted as to the relevance of building professional competence to deal with the disease. As a result, authorities delegate healthcare providers working with sickle cell disease (physicians, nurses, dentists, social assistants, psychologists, physical therapists, physical educators, dieticians and others) to take part in the course. Other professionals wishing to participate in the course are also welcome.
During the period from 2010 to 2016, 2446 professionals were selected to participate in the Cehmob distance education course. Of these, 1171 (48%) successfully concluded the course obtaining a minimum score of 70% for course work and attendance. The remaining 1275 (52%) did not obtain the minimum score or dropped out of the course.
The present study used a database of all professional healthcare providers for the selection of prospective participants. In April 2016, an invitation to participate in this study with a brief explanation of the research, and an informed consent form was sent by email to 300 randomly selected professionals among those enrolled in the course. As the study aimed to assess participants who successfully concluded the course as well as those who did not, 150 professionals were randomly selected from each group.
Of the invitees, 153 (51%) accepted to participate in this study; 72 (47%) had successfully concluded the course (henceforth referred to as Group A) and 81 (53%) had not met the minimum requirements for course completion (Group B).
Participants were requested to answer a questionnaire applied using the web tool e-Surv. This questionnaire comprised three sections: (1) sociodemographic data: sex, education, city of residence, and professional category; (2) details of professional performance: type of health service in which the participant worked and the number of years working in healthcare services; and (3) the DFConhecimento instrument (Attachment 1). Thirteen multiple-choice questions were included about the disease covering: 1. Newborn screening program; 2. Sickle cell disease; 3. Sickle cell anemia genotype; 4. Sickle cell trait; 5. Clinical manifestations; 6. Acute events; 7. Conditions favoring red blood cell hemolysis; 8. Signs of sickle cell disease; 9. Medications; 10. Prophylaxis; 11. Adolescence; 12. Pregnancy; and 13. Prevention of leg ulcers.
The DFConhecimento instrument was constructed and validated by the study authors from May 2015 to April 2016 at the Universidade Federal de Minas Gerais (UFMG). Instrument content validation was carried out by 11 experts in instrument validation and in sickle cell disease that made up a panel of experts. The instrument presented an average content validity index of 0.88. Regarding the reliability analysis, the instrument presented satisfactory indexes. Cronbach's alpha presented a value of 0.818, indicating a high internal consistency. The intraclass correlation coefficient between the test and retest presented a value of 0.67 [95% confidence interval (95% CI): 0.55–0.76], indicating that the temporal reproducibility is acceptable. The instrument presents dimensions composed of items compatible with themes indicated as priorities for knowledge on sickle cell disease by the health professional (diagnosis, treatment and prevention of complications).17
The DFConhecimento instrument scores were calculated with 1 being assigned for correct answers and 0 for incorrect answers (range: 0–13). The qualitative variables—sex, education, training category, number of years working in healthcare services, type of health service and previous experience assisting patients with sickle cell disease—are summarized using absolute and relative frequencies. The scores obtained with the instrument are summarized as mean, median, standard deviation (SD) and interquartile range. The Fisher exact or chi-square tests were used to analyze the homogeneity of groups in relation to sex, education, professional category, professional performance and number of years working in healthcare services. A level of significance of 5% or more (p-value>0.05) indicated evidence of homogeneity.18
The chi-square test with a level of significance of 5% was adopted to compare the proportions of correct answers between Group A and Group B. The qualitative variables are presented using absolute and relative frequencies.18
The Poisson regression model was used to study the influence of factors—having completed the course, sex, academic training, training category, number of years working in healthcare, type of healthcare service and previous experience assisting patients with sickle cell disease.19 Univariate analysis allowed the selection of factors that potentially influenced the knowledge score with a level of significance equal to 25% being considered at this selection stage. Using the selected variables, univariate analysis employing a generalized linear Poisson model was employed to verify the direct influence of distance education on the scores of the professionals and confirmed whether other characteristic variables of the sample had a significant influence on their knowledge. Thus, multivariate Poisson regression models were fit with backward elimination being used to select the variables of the final model. A significance level of 5% was adopted for backward elimination.17 All analyses were performed using the statistical software R (R core team).
The project was approved by the Research Ethics Committee Involving Human Beings of the Universidade Federal de Minas Gerais (decision No. 1.717.975). The agreement of the subjects to participate in the study was recorded by means of the informed consent form available in the initial menu of the electronic questionnaire on the website e-Surv.
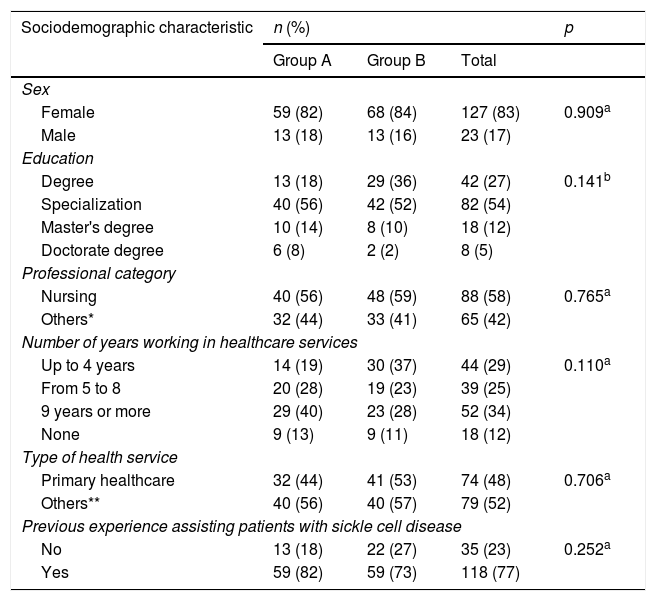
ResultsOf the participants of the study, 127 (83%) were female, 82 (54%) only studied to degree level, 88 (58%) were nurses, 52 (34%) had worked in healthcare services for more than nine years, 118 (77%) had previously provided care to sickle cell disease patients and 134 (90%) work in municipalities in the State of Minas Gerais (Table 2). The groups under study were considered homogeneous in all analyzed variables.
Sociodemographic characterization of the professionals who answered the DFConhecimento instrument stratified depending on course completion.
| Sociodemographic characteristic | n (%) | p | ||
|---|---|---|---|---|
| Group A | Group B | Total | ||
| Sex | ||||
| Female | 59 (82) | 68 (84) | 127 (83) | 0.909a |
| Male | 13 (18) | 13 (16) | 23 (17) | |
| Education | ||||
| Degree | 13 (18) | 29 (36) | 42 (27) | 0.141b |
| Specialization | 40 (56) | 42 (52) | 82 (54) | |
| Master's degree | 10 (14) | 8 (10) | 18 (12) | |
| Doctorate degree | 6 (8) | 2 (2) | 8 (5) | |
| Professional category | ||||
| Nursing | 40 (56) | 48 (59) | 88 (58) | 0.765a |
| Others* | 32 (44) | 33 (41) | 65 (42) | |
| Number of years working in healthcare services | ||||
| Up to 4 years | 14 (19) | 30 (37) | 44 (29) | 0.110a |
| From 5 to 8 | 20 (28) | 19 (23) | 39 (25) | |
| 9 years or more | 29 (40) | 23 (28) | 52 (34) | |
| None | 9 (13) | 9 (11) | 18 (12) | |
| Type of health service | ||||
| Primary healthcare | 32 (44) | 41 (53) | 74 (48) | 0.706a |
| Others** | 40 (56) | 40 (57) | 79 (52) | |
| Previous experience assisting patients with sickle cell disease | ||||
| No | 13 (18) | 22 (27) | 35 (23) | 0.252a |
| Yes | 59 (82) | 59 (73) | 118 (77) | |
Table 3 shows the descriptive statistics of the knowledge scores according to the situation of the professionals in relation to concluding the course. It can be observed that Group A had higher mean and median scores than Group B. Scores ranged from a minimum of 0 to a maximum of 13 points. The mean score was 9.76 (SD: 2.62) for Group A and 6.54 (SD: 3.22) for Group B.
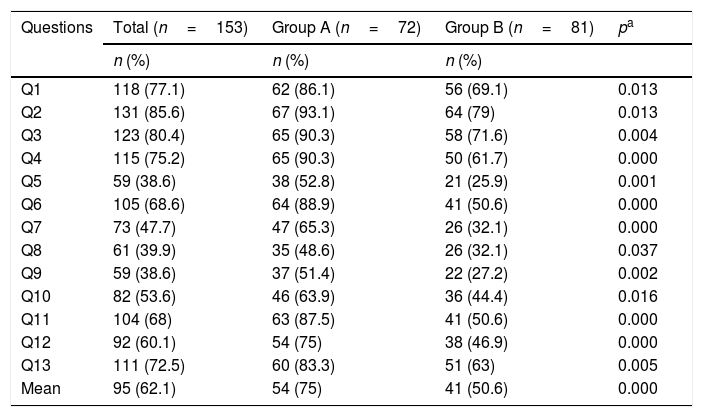
Table 4 presents a comparison of proportions of correct answers between Group A and Group B. There was a significant difference (p-value<0.05) for all the questions with the proportion of correct answers being significantly higher among those who completed the course.
Proportions of correct answers of professionals who answered the questionnaire and completed the course (Group A) and those that did not (Group B).
| Questions | Total (n=153) | Group A (n=72) | Group B (n=81) | pa |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Q1 | 118 (77.1) | 62 (86.1) | 56 (69.1) | 0.013 |
| Q2 | 131 (85.6) | 67 (93.1) | 64 (79) | 0.013 |
| Q3 | 123 (80.4) | 65 (90.3) | 58 (71.6) | 0.004 |
| Q4 | 115 (75.2) | 65 (90.3) | 50 (61.7) | 0.000 |
| Q5 | 59 (38.6) | 38 (52.8) | 21 (25.9) | 0.001 |
| Q6 | 105 (68.6) | 64 (88.9) | 41 (50.6) | 0.000 |
| Q7 | 73 (47.7) | 47 (65.3) | 26 (32.1) | 0.000 |
| Q8 | 61 (39.9) | 35 (48.6) | 26 (32.1) | 0.037 |
| Q9 | 59 (38.6) | 37 (51.4) | 22 (27.2) | 0.002 |
| Q10 | 82 (53.6) | 46 (63.9) | 36 (44.4) | 0.016 |
| Q11 | 104 (68) | 63 (87.5) | 41 (50.6) | 0.000 |
| Q12 | 92 (60.1) | 54 (75) | 38 (46.9) | 0.000 |
| Q13 | 111 (72.5) | 60 (83.3) | 51 (63) | 0.005 |
| Mean | 95 (62.1) | 54 (75) | 41 (50.6) | 0.000 |
The mean percentage of correct answers of subjects in Group A (75.0±2.6%) was higher than the results of Group B (50.6±3.2%).
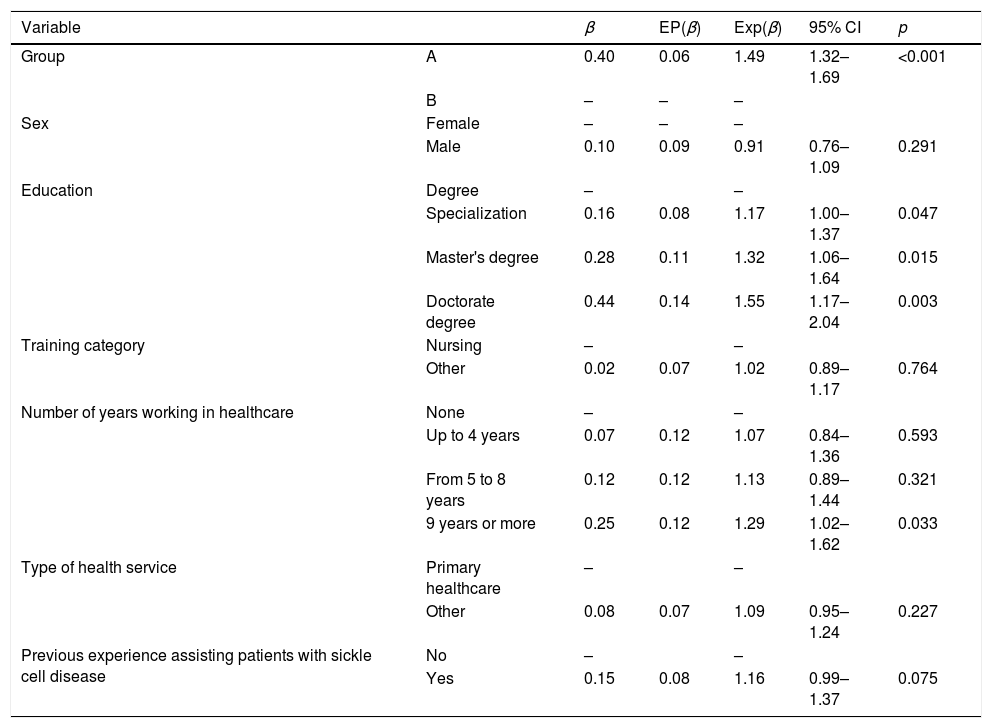
In the univariate analysis (Table 5), the following variables were selected: Group (A and B), academic training, health service type and previous experience assisting sickle cell disease patients; variables were considered possible significant influences when p-values were <0.25. A significant difference regarding the knowledge score (p-value<0.001) was observed between Group A (average score was 49% higher) and Group B. There was a significant difference (p-value<0.005) between training levels. On average, compared to participants with just a degree, those with a specialization presented 17% higher scores; with a master's degree or taking a master's degree had scores 32% higher; while those with a doctorate degree had scores 55% higher. There was a significant difference (p-value=0.033) in the number of years working in healthcare, since the knowledge score for professionals who had worked nine years or more was on average 29% higher than the score of those who had never worked in healthcare. There was no significant difference between mean scores when comparing variables such as gender, professional category, type of healthcare service and whether they had dealt with sickle cell disease patients previously.
Univariate analysis using the Poisson regression model.
| Variable | β | EP(β) | Exp(β) | 95% CI | p | |
|---|---|---|---|---|---|---|
| Group | A | 0.40 | 0.06 | 1.49 | 1.32–1.69 | <0.001 |
| B | – | – | – | |||
| Sex | Female | – | – | – | ||
| Male | 0.10 | 0.09 | 0.91 | 0.76–1.09 | 0.291 | |
| Education | Degree | – | – | |||
| Specialization | 0.16 | 0.08 | 1.17 | 1.00–1.37 | 0.047 | |
| Master's degree | 0.28 | 0.11 | 1.32 | 1.06–1.64 | 0.015 | |
| Doctorate degree | 0.44 | 0.14 | 1.55 | 1.17–2.04 | 0.003 | |
| Training category | Nursing | – | – | |||
| Other | 0.02 | 0.07 | 1.02 | 0.89–1.17 | 0.764 | |
| Number of years working in healthcare | None | – | – | |||
| Up to 4 years | 0.07 | 0.12 | 1.07 | 0.84–1.36 | 0.593 | |
| From 5 to 8 years | 0.12 | 0.12 | 1.13 | 0.89–1.44 | 0.321 | |
| 9 years or more | 0.25 | 0.12 | 1.29 | 1.02–1.62 | 0.033 | |
| Type of health service | Primary healthcare | – | – | |||
| Other | 0.08 | 0.07 | 1.09 | 0.95–1.24 | 0.227 | |
| Previous experience assisting patients with sickle cell disease | No | – | – | |||
| Yes | 0.15 | 0.08 | 1.16 | 0.99–1.37 | 0.075 |
95% CI: 95% confidence interval.
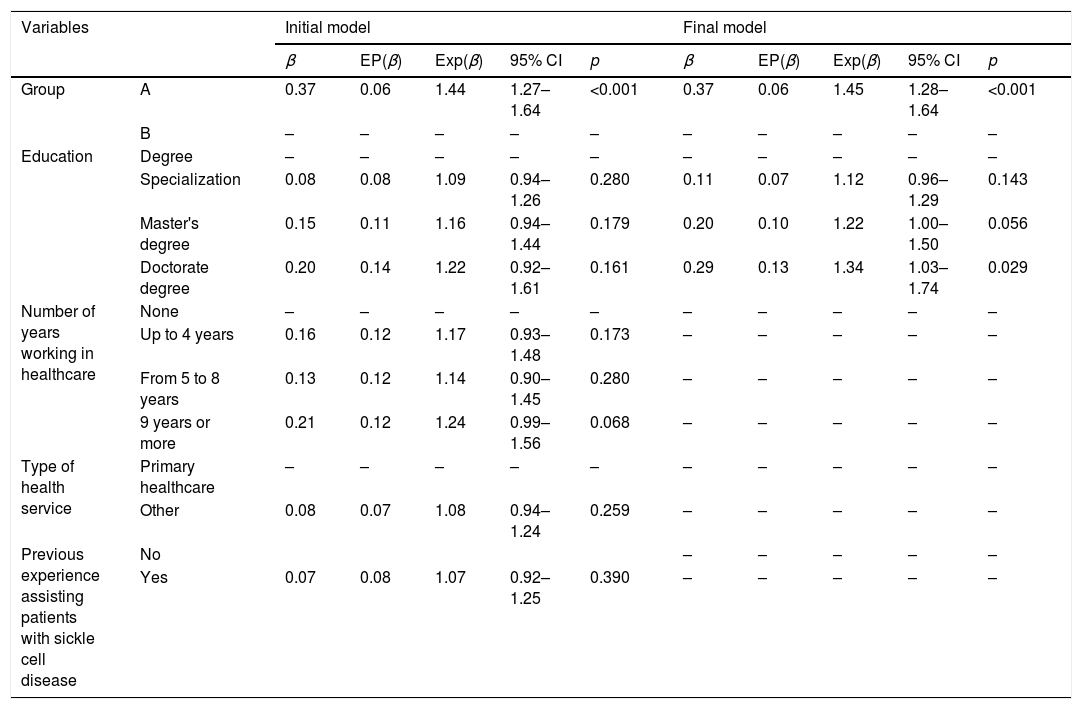
Table 6 presents the results of the Poisson regression model adjusted using the variables: group, academic training, health service type and previous assistance to patients with sickle cell disease (initial multivariate model). The final multivariate model was reached after step-by-step elimination of non-significant variables (p-value>0.05) from the initial model (Table 6). The analysis of the final model shows that Group A maintained a significant difference, presenting on average 45% (95% CI: 28–64%) higher scores than Group B, even when this comparison is adjusted by the level of training. There was also a significant difference (p-value=0.029) in the means of the knowledge score of professionals with different levels of academic training; those with a doctoral degree had, on average, 34% (95% CI: 3–73%) higher scores when compared to professionals just with graduation. For the levels of specialization and master's degree, no statistically significant differences were observed in the score in relation to the level of graduation.
Results of multivariate analysis (adjustment of the generalized linear Poisson model).
| Variables | Initial model | Final model | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β | EP(β) | Exp(β) | 95% CI | p | β | EP(β) | Exp(β) | 95% CI | p | ||
| Group | A | 0.37 | 0.06 | 1.44 | 1.27–1.64 | <0.001 | 0.37 | 0.06 | 1.45 | 1.28–1.64 | <0.001 |
| B | – | – | – | – | – | – | – | – | – | – | |
| Education | Degree | – | – | – | – | – | – | – | – | – | – |
| Specialization | 0.08 | 0.08 | 1.09 | 0.94–1.26 | 0.280 | 0.11 | 0.07 | 1.12 | 0.96–1.29 | 0.143 | |
| Master's degree | 0.15 | 0.11 | 1.16 | 0.94–1.44 | 0.179 | 0.20 | 0.10 | 1.22 | 1.00–1.50 | 0.056 | |
| Doctorate degree | 0.20 | 0.14 | 1.22 | 0.92–1.61 | 0.161 | 0.29 | 0.13 | 1.34 | 1.03–1.74 | 0.029 | |
| Number of years working in healthcare | None | – | – | – | – | – | – | – | – | – | – |
| Up to 4 years | 0.16 | 0.12 | 1.17 | 0.93–1.48 | 0.173 | – | – | – | – | – | |
| From 5 to 8 years | 0.13 | 0.12 | 1.14 | 0.90–1.45 | 0.280 | – | – | – | – | – | |
| 9 years or more | 0.21 | 0.12 | 1.24 | 0.99–1.56 | 0.068 | – | – | – | – | – | |
| Type of health service | Primary healthcare | – | – | – | – | – | – | – | – | – | – |
| Other | 0.08 | 0.07 | 1.08 | 0.94–1.24 | 0.259 | – | – | – | – | – | |
| Previous experience assisting patients with sickle cell disease | No | – | – | – | – | – | |||||
| Yes | 0.07 | 0.08 | 1.07 | 0.92–1.25 | 0.390 | – | – | – | – | – | |
95% CI: 95% confidence interval.
The characteristics of the sample studied related to the variables of gender, professional category and specialization were similar to those observed in other studies with professional healthcare providers. In those, most of the professionals were female, with a nursing background and some level of specialization.16,20 A favorable aspect of this study, observed in the characterization of the sample, is related to the graduate and higher education groups, which were considered homogeneous in all the variables analyzed.
In the individual evaluation of the items of the DFConhecimento instrument, the proportion of correct answers for the whole instrument were on average 75% higher among the participants in Group A. This average was higher than that observed in a study carried out in the United States (65%) that investigated knowledge about sickle cell disease among physicians and nurses of emergency services who participated in a workshop that included ten lectures given by specialists in the area. The participants answered an electronic questionnaire of multiple-choice questions prepared by the authors of the study before the beginning of the lectures and after the event.7
The results of DFConhecimento, verified by the descriptive analysis of the scores and by the generalized linear Poisson model, showed that members of Group A had significantly more knowledge about the disease after the course compared to Group B. A similar result was obtained in a randomized study carried out in the northern part of the State of Minas Gerais, aimed at assessing an educational program about sickle cell disease that targeted community healthcare agents and nursing assistants working in primary healthcare. Participants in the study showed knowledge acquisition by improvements in their performance during the assessment (p-value<0.001).21 Studies verified a significant positive impact on knowledge of professional healthcare providers after being submitted to an intervention in other health domains using the method of distance education.14–16
The positive impact of the distance education course about sickle cell disease on the professionals who completed the study suggests that this educational strategy can be introduced in the context of all professional healthcare providers working in the healthcare network. Thus, it is important that this strategy includes content related to knowledge deficits of professional healthcare providers as described in the literature: content that addresses pathophysiological complications, transfusion, prevalence of iron overload, stroke in children, clinical manifestations as well as the management of sickle cell disease.2,7,9,10,12
The results obtained from the professionals in this study and reported in the literature show that a deficit of knowledge about sickle cell disease exists and persists despite the technical-scientific advances and the availability of guidelines with recommendations for professional practice. However, the positive impact on the knowledge about sickle cell disease of professionals after participating in educational interventions was confirmed in recent studies with North American, Brazilian and Mexican professionals with different educational levels using qualitative and quantitative methods of knowledge assessment.2,10,22–24
This study fills a gap highlighted in a previous study, which recommended including physicians and nurses in educational programs on sickle cell disease.21 Because this educational intervention seeks to improve the knowledge of professionals in respect to sickle cell disease using technology, its strong point is the viability of reproducing this study with more participants and with geographical expansion to represent a greater proportion of professionals.15,16,25
ConclusionDistance learning courses have a positive impact on the knowledge acquired by professional health providers about sickle cell disease. It is essential to include professionals who assist sickle cell disease patients in similar educational actions.
Conflicts of interestThe authors declare no conflicts of interest.



