






The rapid increase in the aged population has resulted in a growing number of cases of chronic diseases. This increase is an important demographic change that low- and middle-income countries have to face and poses a new challenge to health services. One of the first steps to formulate public policies is to understand the reality of each country's aging population. This study describes the prevalence of anemia, hypertension and diabetes and the overall health status in pre-elderly and elderly subjects enrolled in two primary health care clinics, Eldorado and Piraporinha, in the city of Diadema, São Paulo.
MethodA cross-sectional study was conducted with 373 participants. Clinical data were collected from patient charts and the degree of disability and common mental disorders, as well as demographic data were obtained by interviews.
ResultsThe prevalence of anemia was approximately 11% and hypertension was 70% and 81% in Eldorado and Piraporinha, respectively. The frequency of diabetes was 52% in Eldorado and 30% in Piraporinha. The subjects of both health care clinics reported having difficulties in some of their daily physical and instrumental activities, with physical symptoms and emotional disorders.
ConclusionAnemia, hypertension and diabetes are prevalent in the studied population, and patients showed degrees of dependency and impaired health status.
Increases in the proportion of older people are a universal phenomenon. The forecast for this older population (>65 year old) for 2100, across the globe, is more than triple the current number.1 This demographic change is a consequence of socioeconomic growth and increasing prosperity, resulting in a higher average life expectancy.2 However, this aging of the population has an impact on health care systems, in part due to the increase in the number of people with chronic diseases.3
Life expectancy is higher in developed countries however the absolute number of older adults is concentrated in developing countries.4 In the past 50 years, Brazil, the fifth largest country in the world, has experienced a demographic revolution. According to the Brazilian census department, the Instituto Brasileira de Geografia e Estatística, the average life expectancy in Brazil had reached 73 years in 2009 (76.5 and 69 years for women and men, respectively).5 Nevertheless, the corresponding rate of socioeconomic growth and improvement in health care has not kept up with this rapid rate of aging of the Brazilian population.6 Thus, understanding the Brazilian reality of this aging population could help implement local health policies and interventions based on diversities.
The aim of this study was to evaluate the prevalence of anemia, hypertension and diabetes and to correlate these issues with the overall health status in pre-elderly (50–59 years) and elderly patients (age ≥60 years) enrolled in two primary care clinics.
MethodStudy designThis is a cross-sectional observational study carried out at two primary referral centers for elderly care, Eldorado and Piraporinha. Both clinics are in the city of Diadema, which along with other cities, belongs to the conurbation of São Paulo. The Eldorado clinic is located in the outskirts of the city and the Piraporinha clinic is located in a more privileged area, in the city center, conferring different geographic contexts to the clinics.
ParticipantsThis study included 373 participants with clinical data being collected between November 2012 and April 2013. All pre-elderly and elderly male and female individuals (50 years or older) of the two clinics were invited to participate in the study. Subjects who did not live in Diadema and individuals who refused to participate in the study were excluded from the study, as were those who were unable to answer the questions due to deafness, blindness, or with difficulties to understand. A simple random sampling method was used. In order to calculate the sample size, the elderly population of Diadema was considered to be approximately 4% of the total population,5 thus using a 95% confidence level and 5% sampling error, the minimum sample size required was 280 subjects.7 All the individuals who participated in the study provided informed written consent. The Ethics Committee of the Universidade Federal de São Paulo (Unifesp) approved the study protocol (#142.778).
Diagnosis of anemia, hypertension and diabetesDiagnoses of anemia, high blood pressure and diabetes mellitus were based on clinical charts, whenever available. The diagnoses for anemia and diabetes were based on the results from automated hematology and biochemistry analyzers, respectively. Anemia was defined according to World Health Organization criteria8 as a hemoglobin level <13g/dL in men or <12g/dL in women. The diagnosis of diabetes was defined based on the current American Diabetes Association (ADA) guidelines, which include a fasting plasma glucose level of ≥7.0mmol/L (126mg/dL).9 Hypertension was defined as a consistent (three or more readings by the physician during a medical appointment) systolic blood pressure (SBP) ≥140mmHg or a diastolic blood pressure (DBP) ≥90mmHg.10
ProcedureOne hundred and seven subjects agreed to complete the Brazilian Older Americans Resources And Services Multidimensional Functional Assessment Questionnaire (BOMFAQ)7,8 and the Self-Reporting Questionnaire (SRQ-20)9,10; both interviews were carried out in person by trained students. Demographic data regarding the number of years of schooling and income were also obtained. The BOMFAQ consists of 15 questions about activities of daily living (ADL), divided into two sub-scales; eight physical ADL (PADL), and seven instrumental ADL (IADL). The PADL included getting into and out of bed, eating, combing the hair, walking on flat surfaces, having a bath/shower, getting dressed, getting to the toilet in time and cutting toenails. The IADL included climbing stairs (one flight), taking medicines on time, walking close to home, shopping, preparing meals, getting off buses and cleaning the house.11 The subjects’ responses to the BOMFAQ were analyzed according to two criteria: with or without difficulty to complete the task.
Statistical analysisAll statistical data analyses were performed using the Statistical Package for the Social Sciences (SPSS, version 21.0; IBM Corp., 2012). The Student's t-test, the chi-square test, and the Pearson correlation coefficient with a level of significance of 5% and a 95% confidence interval (95% CI) were used for data analysis. A two-tailed p-value <0.05 was considered statistically significant.
ResultsStudy populationThis report is based on 373 participants; 40% were pre-elderly subjects (50–59 years old) and 60% were women. There were no statistically significant differences in the clinical data (including age and gender) between the health care clinics (Table 1).
Clinical characteristics of subjects.
| Characteristic | Eldorado | Piraporinha | p-Valuea |
|---|---|---|---|
| Age (years) – mean (range) | 61 (50–93) | 62 (50–101) | 0.377 |
| Pre-elderly – n (%) | 40 (41.7) | 115 (41.5) | – |
| Elderly – n (%) | 56 (58.3) | 162 (58.5) | – |
| Gender – n (%) | |||
| Male | 36 (37.5) | 105 (37.9) | 0.943 |
| Female | 60 (62.5) | 172 (62.1) | |
| Peripheral blood parameters – mean (range) | |||
| Erythrocytes (×1012L) | 4.63 (2.41–5.8) | 4.63 (3.00–6.79 | 0.401 |
| Hematocrit (%) | 41.3 (27.2–51.1) | 41.1 (25.1–60.9) | 0.504 |
| Hemoglobin (g/dL) | 13.9 (9.2–17.8) | 13.7 (8.2–20.8) | 0.559 |
| Total leukocytes (×109/L) | 6.85 (2.6–11.9) | 6.1 (0.8–16.2) | 0.460 |
| Mean corpuscular volume | 89.4 (65.6–112.9) | 89.4 (59.6–101.4) | 0.702 |
| MCH (pg/cell) | 30.1 (20.3–38.2) | 30.3 (18.5–36.8) | 0.249 |
| MCHC (g/dL) | 33.6 (30.9–36.6) | 33.8 (13.0–39.5) | 0.461 |
| RDW (%) | 13.1 (10.7–27.0) | 12.8 (10.1–17.9) | 0.151 |
| Platelets (×109/L) | 228 (130–654) | 234 (81–454) | 0.316 |
| Fasting plasma glucose | 117.8 (67–376) | 106.14 (43–432) | 0.06 |
MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration; RDW: red cell distribution width.
The prevalence of anemia in the studied population was approximately 11% for men and women in both health care clinics with hemoglobin <10g/dL being found in approximately 2% of the subjects (Table 2).
Prevalence of anemia, diabetes and hypertension.
| Eldorado | Piraporinha | p-Valuea | |
|---|---|---|---|
| Anemia – n (%) | 11 (11.5) | 32 (11.6) | 0.9802 |
| Male:female ratio | 4:1 | 11:21 | 0.9050 |
| Hemoglobin – n (%) | |||
| ≥10g/dL | 94 (97.9) | 270 (97.5) | 0.8071 |
| <10g/dL | 2 (2.1) | 7 (2.5) | |
| Diabetes – n (%) | 25 (52.1) | 25 (30.5) | 0.0241 |
| Male:female ratio | 10:15 | 11:14 | 0.7 |
| Hypertension – n (%) | 45 (81.8) | 55 (69.6) | 0.16 |
| Male:female ratio | 14:31 | 23:32 | 0.37 |
Approximately 52% of the subjects had diabetes in the Eldorado health care clinic which was a significantly higher frequency when compared to Piraporinha, where nearly 30% of the subjects were diabetic (p-value=0.0241; Table 2).
The frequencies of hypertension were similar in both clinics (70% in Eldorado and 81% in Piraporinha) with no statistically significant difference between genders (Table 2).
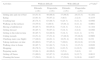
Hemoglobin values and ageThe Pearson correlation coefficient demonstrated that hemoglobin levels were inversely associated with age (Figure 1). In addition, hemoglobin values were significantly lower in the elderly when compared with the pre-elderly group (Figure 2).
Assessment of the degree of dependency and common mental disorders with age (years).")
 in pre-elderly and elderly groups (horizontal lines indicate medians).")
One hundred and seven subjects were assessed using both the BOMFAQ and the SRQ-20 instruments to evaluate the degree of disability and common mental disorders, respectively. Table 3 shows the sociodemographic data of the sample.
Sociodemographic characteristics.
| Eldorado n (%) | Piraporinha n (%) | p-Valuea | |
|---|---|---|---|
| Gender | |||
| Male | 5 (14.3) | 23 (31.9) | |
| Female | 30 (85.7) | 49 (68.1) | 0.05 |
| Education (years) | |||
| None | 4 (11.4) | 8 (11.1) | 0.3 |
| 1–3 | 25 (71.4) | 38 (52.8) | |
| 4–7 | 2 (5.7) | 10 (13.9) | |
| 8+ | 4 (11.5) | 16 (22.2) | |
| Monthly income (R$)b | |||
| 0–723 | 15 (44.1) | 21 (30) | 0.15 |
| 724–2172 | 19 (55.9) | 44 (62.9) | |
| 2173+ | 0 | 5 (7.1) | |
When the subjects were evaluated according to their level of independence, the subjects from the Eldorado health care clinic generally reported having more difficulties in two PADL and two IADL; walking on flat surfaces (44.1%), getting dressed (14.2%), getting off buses (40%) and cleaning the house (50%) (Table 4). Subjects from Eldorado also presented with more physical symptoms and emotional disorders when compared with Piraporinha subjects (Table 5).
Difficulty for perform 15 activities of daily life by group.
| Activities | Without difficult | With difficult | p-Valuea | ||
|---|---|---|---|---|---|
| Eldorado n (%) | Piraporinha n (%) | Eldorado n (%) | Piraporinha n (%) | ||
| Getting into and out of bed | 18 (51.4) | 48 (66.8) | 17 (48.6) | 24 (33.3) | 0.1282 |
| Eating | 32 (91.4) | 70 (97.2) | 3 (8.6) | 2 (2.8) | 0.3275 |
| Combing hair | 26 (74.3) | 63 (88.7) | 9 (25.7) | 8 (11.3) | 0.0566 |
| Walking on flat surfaces | 19 (55.9) | 6 (88.9) | 15 (44.1) | 8 (11.1) | 0.0001 |
| Having a bath/shower | 30 (85.7) | 69 (95.8) | 5 (14.3) | 3 (4.2) | 0.1104 |
| Getting dressed | 30 (85.7) | 70 (97.2) | 5 (14.3) | 2 (2.8) | 0.0366 |
| Getting to the toilet in time | 30 (85.7) | 64 (88.9) | 5 (14.3) | 8 (11.1) | 0.754 |
| Cutting toenails | 18 (51.4) | 37 (51.4) | 17 (48.6) | 35 (48.6) | 0.9969 |
| Climbing stairs (one flight) | 17 (48.6) | 44 (61.1) | 18 (51.4) | 28 (38.9) | 0.219 |
| Taking medicines on time | 28 (80.0) | 57 (85.1) | 7 (20.0) | 10 (14.9) | 0.5138 |
| Walking close to home | 30 (85.7) | 61 (84.7) | 5 (14.3) | 11 (15.3) | 0.8926 |
| Shopping | 26 (76.5) | 51 (89.5) | 8 (23.5) | 6 (10.5) | 0.0963 |
| Preparing meals | 32 (94.1) | 48 (96.0) | 2 (5.9) | 2 (4.0) | 1.0 |
| Getting off buses | 21 (60.0) | 62 (87.3) | 14 (40.0) | 9 (12.7) | 0.0013 |
| Cleaning the house | 17 (50.0) | 39 (81.3) | 17 (50.0) | 9 (18.8) | 0.0027 |
Results of the SRQ-20 questionnaire by group.
| Yes | No | p-Valuea | |||
|---|---|---|---|---|---|
| Eldorado n (%) | Piraporinha n (%) | Eldorado n (%) | Piraporinha n (%) | ||
| 1. Headaches | 12 (34.3) | 9 (12.5) | 23 (65.7) | 63 (87.5) | 0.0078 |
| 2. Poor appetite | 14 (40.0) | 13 (18.1) | 21 (60.0) | 59 (81.9) | 0.0142 |
| 3. Sleeping badly | 15 (42.9) | 29 (40.3) | 20 (57.1) | 43 (59.7) | 0.7992 |
| 4. Easily frightened | 17 (48.6) | 18 (25.0) | 18 (51.4) | 54 (75.0) | 0.0148 |
| 5. Hands shake | 9 (25.7) | 9 (12.5) | 26 (74.3) | 63 (87.5) | 0.0865 |
| 6. Feeling nervous, tense or worried | 26 (74.3) | 41 (56.9) | 9 (25.7) | 31 (43.1) | 0.082 |
| 7. Poor digestion | 12 (34.3) | 17 (23.6) | 23 (65.1) | 55 (76.4) | 0.2438 |
| 8. Trouble thinking clearly | 15 (42.9) | 8 (11.1) | 23 (57.14) | 64 (88.9) | 0.0002 |
| 9. Feeling unhappy | 24 (68.6) | 32 (44.4) | 11 (31.4) | 40 (55.6) | 0.0191 |
| 10. Crying more than usual | 12 (32.3) | 19 (26.4) | 23 (65.7) | 53 (73.6) | 0.3982 |
| 11. Difficulty in enjoying daily activities | 14 (40.0) | 21 (29.17) | 21 (60.0) | 51 (70.8) | 0.2625 |
| 12. Difficulty in making decisions | 14 (40.0) | 21 (38.9) | 21 (60.0) | 51 (70.8) | 0.9121 |
| 13. Daily suffering at work | 11 (31.4) | 15 (20.8) | 24 (68.6) | 57 (79.2) | 0.2306 |
| 14. Unable to play a useful role in life | 14 (40.0) | 14 (19.4) | 21 (60.0) | 58 (80.6) | 0.0232 |
| 15. Lost interest in things | 20 (57.1) | 26 (36.1) | 15 (42.9) | 46 (63.9) | 0.0392 |
| 16. Feeling that you are a worthless person | 8 (22.9) | 6 (8.3) | 27 (77.1) | 66 (91.7) | 0.063 |
| 17. Thoughts of ending your life have been on your mind | 6 (17.1) | 6 (8.3) | 27 (77.1) | 66 (91.7) | 0.2008 |
| 18. Feeling tired all the time | 14 (41.2) | 16 (22.2) | 20 (58.8) | 56 (77.8) | 0.0432 |
| 19. Uncomfortable feelings in your stomach | 15 (42.9) | 23 (30.6) | 20 (57.1) | 50 (69.4) | 0.2094 |
| 20. Easily tired | 17 (48.6) | 23 (31.9) | 18 (51.4) | 49 (68.1) | 0.0954 |
This study revealed that approximately 11% of the subjects of 50 years of age and older presented anemia according to WHO criteria in both health care clinics. The low prevalence of anemia in our cohort corroborates other studies that also assessed the prevalence of anemia among free-living elderly people; Guralnik et al. presented data regarding a North American population,12 Salive et al. reported on the Epidemiologic Study of the Elderly (EPESE)13 and Inelmen et al. described data in a representative Italian population.14 In the current study, the anemia was mild in the majority of the anemic subjects. In this cohort, normocytic anemia was the most common type of anemia (between 54.5% and 70%), which is consistent with a Brazilian study that studied free-living elderly individuals in southern Brazil.15 Anemia of inflammatory response is most often described as a normocytic normochromic anemia and is usually mild.16 The risk factors linked to the majority of chronic diseases, such as diabetes, have been shown to increase inflammation,17 and in this study, there were high frequencies of both diabetes and hypertension. Despite having observed a negative correlation between hemoglobin levels and age, with lower hemoglobin values in the elderly when compared to the pre-elderly group, it is not believed that these values are due to age. There is a body of evidence that suggests that most cases of anemia in older people are due to poor health and should prompt further investigations in the clinical practice, even when the person has no apparent clinical disease.12,18
With regard to the high prevalence of hypertension in the current cohort, the literature shows that the prevalence of hypertension increases with age in adults19 and can reach a prevalence as high as 80%.20–23 It is important to point out that hypertension is independently associated with cardiovascular diseases in the elderly.
This study focused on a description of the prevalence of diseases related to elderly individuals and their quality of life. Although there were no social and demographic differences, the study was performed in two contrasting areas of Diadema. While the Piraporinha clinic is located in a more privileged area, in the city center, the Eldorado clinic is located in the poorer outskirts. The subjects that live in the outskirts had significantly lower scores for two PADL and two IADL than the subjects who lived in the city center. Subjects from Eldorado also presented a significantly higher prevalence of minor psychiatric disorders, when compared to the subjects from Piraporinha. Moreover, the prevalence of diabetes was much higher in the Eldorado health care clinic. The literature shows that the incidence of depression and impaired cognitive function increases in elderly individuals with diabetes.24 Moreover, depression in elderly patients with diabetes is a strong predictor of hospitalization and death25; anxiety and stress in the elderly are important health issues frequently associated with poorer physical and emotional well-being.26
ConclusionRegardless of the location of the health care clinic, there are prevalences of anemia, hypertension and diabetes in the populations of pre-elderly and elderly individuals. Both these groups showed degrees of dependency and impairment of health status. Our findings might aid public health care managers in the targeting of strategies to promote better health in the aging population.
Conflicts of interestThe authors declare no conflicts of interest.
Funding for this work was provided by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). The authors would like to thank Raquel Susana Foglio for the English review.



