
The severe acute respiratory syndrome-2 virus (SARS-Cov2) continues to be a threat worldwide, with over 415 million cases and 5 million deaths, as of the time this study was written.1 All efforts to discover therapeutic, diagnostic and preventive strategies have been the priority of the medical and scientific community. By 2020, several vaccines had become available for use in different parts of the world, over 40 candidate vaccines were in human trials and over 150, in preclinical trials.2 Robust data on vaccine efficacy is available in the literature and there is no question of its importance in the battle against the COVID-19. The safety of these vaccines is also well documented in clinical trials with healthy subjects, though as clinicians, we must be vigilant with patients who have pre-existing autoimmune diseases. The most common immune cytopenia reported post-vaccination was immune thrombocytopenic purpura (ITP); rarely was autoimmune hemolytic anemia (AIHA) mentioned. The AIHA is characterized by an increased destruction of red blood cells (RBCs), mediated by autoantibodies against RBC antigens. This report details the case of a female patient with a severe relapsed AIHA after receiving the booster with mRNA-1273 vaccine.
Case presentationA 33-year-old female was admitted because of symptoms of severe anemia. She was apparently well until 1 day after the covid-19 booster vaccination, when she developed flu-like illness and pain at the injection site, for which she took paracetamol. After two days post-vaccination, she developed dizziness, generalized weakness and pallor. As she had a history of AIHA, which had been in remission, she immediately underwent a complete blood count. This showed severe anemia with a hemoglobin count of 52g/L; hematocrit, 0.15; WBC 5.0 segs, 65; lymphocytes, 0.24, monocytes, 0.06, and; platelets, 165,000/ul. A hematology consult was performed and an oral steroid, using prednisone 1mg/kg/day, was started. After 3 days, there was progression of symptoms and hence, the patient was advised to be hospitalized.
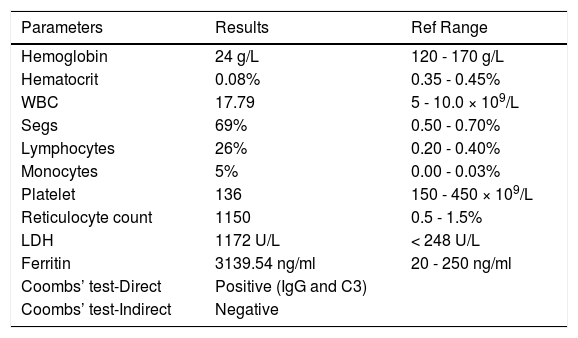
Upon admission, the patient appeared to be weak and was wheelchair-assisted and slow to respond, but had person, time and place orientation. Her vital signs showed a BP of 110/70; HR, 122 bpm; RR, 23, and; T, 37.0. On physical examination, the patient was pale and had sallow skin; slightly icteric sclerae; pale palpebral conjunctivae; palmar pallor, and; no hepatosplenomegaly. The laboratory exams showed severe anemia, reticulocytosis, direct Coombs’ test positive (IgG and C3 positive), elevated LDH and hyperferritinemia. (Table 1) The medical history included AIHA diagnosed in 2012, with 7 episodes of hemolysis over a span of 10 years, the last of which was in late 2020 during her pregnancy and was mild, with a hemoglobin of 90 g/L, and she responded well to an oral steroid. She has been in remission thereafter. There were no illnesses in the preceding 6 months. The review of medications showed folic acid, calcium and vitamin D, with no new drugs being taken for the past 6 months. She had her primary doses of COVID-19 vaccine last June and July 2021, using the inactivated virus vaccine (Sinovac/Coronavac), which proved uneventful. Her last complete blood count (CBC) was performed during the month of her second vaccine dose, which was normal, with a hemoglobin of 132 g/L; hematocrit, 0.38; WBC, 5.88; segs, 52; lymphocytes, 40; monocytes, 0.07, and; basophil, 0.01. Her platelet count was adequate.
Laboratory results on admission.
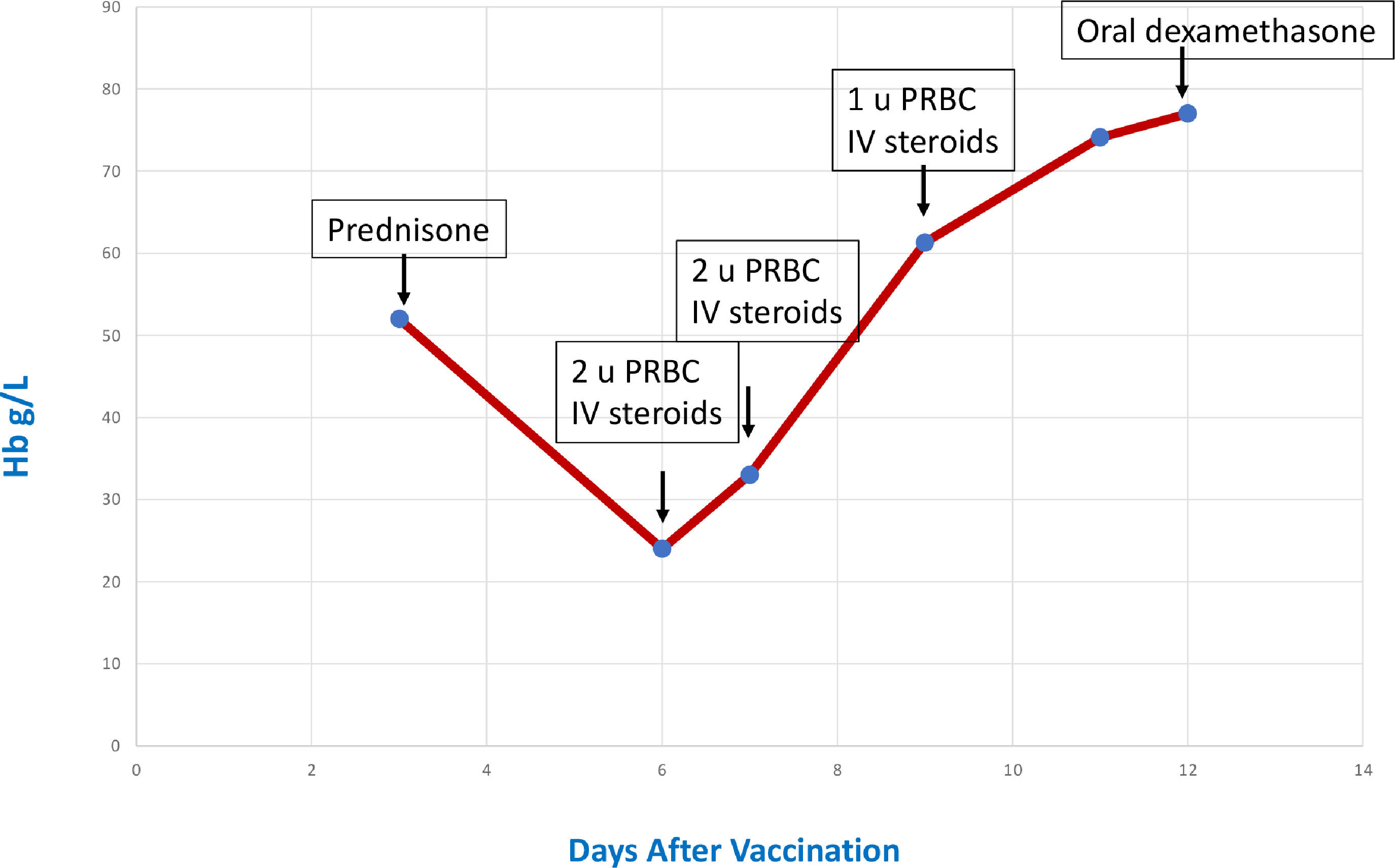
The patient was started on an intravenous steroid. Packed red cells were transfused to alleviate the symptoms of anemia. There were elevations in the blood sugar while on the steroid, which were managed with insulin. The hemogram was monitored wherein a steady rise was seen during the hospitalization. (Figure 1) She was discharged stable with oral steroids.
Discussion
Vaccination is considered the most promising approach to turn the tide in any pandemic, including COVID-19. It confers protection from viral infection by eliciting protective antibody response. Since early 2020, global attempts have been made to produce a suitable vaccine against the SARS-Cov2. Several types of vaccines were developed, namely, the inactivated virus, live attenuated, non-replicating/replicating viral vector and mRNA vaccines. Messenger RNA vaccines have emerged as front runners in the commencement of vaccination programs. They work by providing the blueprint of the pathogen's antigen. The body's ribosomes translate the mRNA into spike proteins. These are then released from the cell, allowing the host to mount an immune response.3 The current evidence suggests that mRNA vaccines elicit a strong humoral response due to the production of neutralizing antibodies, coupled with a robust cellular response by inducing functional and pro-inflammatory CD4 + and CD8 + T cells and expression of Th1 cytokines.4-5 Large placebo-controlled phase III trials on the mRNA-1273 reported a vaccine efficacy rate of 86.4% and 94.1% and hence, it was granted emergency use authorization (EUA) for the prevention of COVID-19.6-7 These vaccine clinical trials, aside from mentioning the low incidence of local and systemic reactions (e.g. fever, chills and headache), not one has cited hematologic side effects. It was only during the large-scale vaccination efforts that immune thrombocytopenic purpura (ITP) and thrombocytopenia with thrombosis syndrome (TTS) for mRNA and vector-vaccine, respectively, were reported.8-10;11-14 In these reports, the exact pathogenesis was not fully determined, but autoimmunity and/or molecular mimicry were hypothesized as the possible mechanism/s.
Autoimmune hemolytic anemia (AIHA) is defined as a decompensated acquired hemolysis caused by the host's immune system acting against its own red cell antigens. It is classified as primary or secondary, depending on the presence of an underlying disease or condition promoting immune dysregulation.15 There are 2 types, based on the temperature at which the antigen-antibody reaction occurs. Warm AIHA constitutes 80 to 90% of adult cases, hemolysis is mediated by IgG antibodies at 37°C while cold AIHA involves IgM antibodies with the maximal reaction at temperatures < 4°C. The rate of hemolysis and the severity of the anemia may vary from mild to severe and life-threatening. The typical laboratory features include anemia, reticulocytosis, spherocytes in blood smear, elevated LDH, indirect hyperbilirubinemia, positive Coombs’ test and other specific serologic tests, depending on the type of the AIHA.16 The literature has shown that both the COVID-19 infection and vaccine may trigger AIHA. Angileri et al., in their correspondence to the British Journal of Hematology, found that the ANK-1(Ankyrin-1), an RBC membrane protein shares a putative immunogenic-antigenic epitope with 100% identity to the spike glycoprotein of the SARS-CoV-2. This may lead to erythrocyte destruction through antibody cross-reactivity and molecular mimicry.17 Taherifard et al., in a systematic review of 58 articles, showed 58.5% (55/94 patients) developed ITP, while 23.4% (22/94 patients) had AIHA during the course of the COVID-19 infection.18 This was consistent with the review by Jacobs et al. showing 50 patients with AIHA associated with the COVID-19 infection, the majority being the cold-type AIHA 36% (18/50), 28% (14/50), the warm type AIHA and others, mixed and Evan's syndrome.19
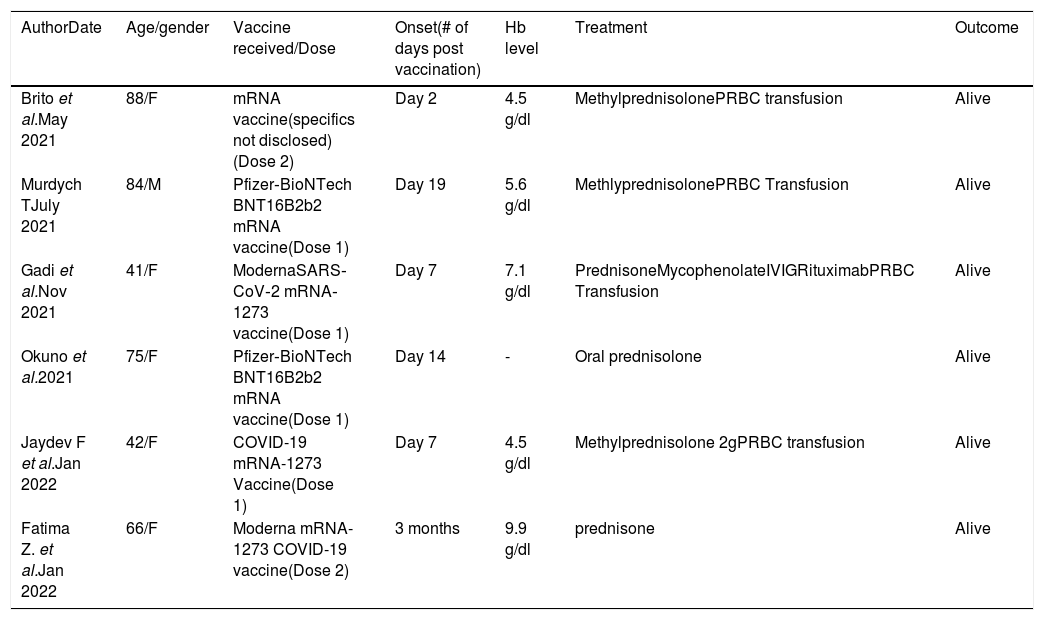
Various case reports have been published regarding AIHA after COVID-19 vaccination, all of whom received the mRNA vaccine. Hemolysis was noted in the majority after the first dose, but was also seen after the second dose. The severity of the symptoms ranges from mild to severe. The diagnosis is made based on the clinical presentation, chronology of events from vaccination and confirmation with a positive direct antiglobulin test. The onset of symptoms ranged from day 2 to day 19 post-vaccination.20-24 The most delayed onset reported was 3 months post-vaccination.25 The standard management used in AIHA is employed in these cases. The treatment involves immunosuppression with corticosteroids, such as prednisone at 1mg/kg/day as first-line therapy. The second-line therapy includes the use of Rituximab, an anti-CD20 monoclonal antibody. And the third-line therapy includes the use of azathioprine, cyclosporine, cyclophosphamide and mycophenolate mofetil (Table 2).
Case reports of AIHA after COVID-19 vaccination.
In a prospective study involving 108 patients with pre-existing autoimmune cytopenia who received the COVID-19 vaccination, patients were monitored through complete blood count and LDH determination. Out of the total population, 4 patients experienced clinically significant hemoglobin reduction requiring treatment adjustment. Three of the four had received the mRNA vaccine prior to the onset of the symptoms. An increment in the steroid doses eventually improved the hemolysis.26 Another retrospective study showed the possibility of relapsed autoimmune cytopenia from a pre-existing disease, which tends to be more severe and hence, should be closely monitored post-vaccination.27
This patient is unique in 2 ways; 1) she has a pre-existing autoimmune hemolytic anemia-in remission, and; 2) she completed primary Covid-19 vaccination using inactivated virus vaccine with no adverse effect. Hemolysis was only noted during her booster shot using the mRNA vaccine.
ConclusionThis case showed the possibility of recurrence of the AIHA shortly after the COVID-19 vaccination. Although it cannot definitely determine any causation, we cannot exclude the possibility of the patient's mRNA vaccination as an inciting or precipitating factor. Patients with pre-existing autoimmune cytopenia should be closely monitored. A hemolytic event is responsive to steroids and other immunosuppressive agents.
Ethical considerationsThe patient's consent for publication was obtained.


