



Hemophilia is an X-linked recessive genetic disorder which affects approximately 400,000 people globally. Differing healthcare reimbursement systems, budgetary constraints and geographical and cultural factors make it difficult for any country to fully deliver ideal care. Although developed countries have sufficient treatment products available, they are burdened by the higher expectation of outcomes, coupled with insufficient supportive care to monitor adherence and outcomes and to implement regular follow-up. In contrast, developing regions may not have ready access to factor replacement, but have developed excellent physiotherapy and rehabilitation programs. Although there are multiple studies that have attempted to assess country-specific variations in hemophilia care, very few compare hemophilia care between economically unequal countries and the challenges in achieving optimal hemophilia care. This literature review tries to bridge this gap and throws light on the country-specific differences in epidemiology, standard of hemophilia care and challenges faced in Canada and China. Data sources resulted in 20 studies (11 from Canada and 9 from China), which were reviewed. In a developed country, the main advantages are: the early treatment of bleeding episodes and the presence of a specialized interdisciplinary and comprehensive treatment concept. This is not the case in most developing countries, where the government does not have the resources to buy the necessary quantities of coagulation factors in the face of more urgent health priorities and hardly a few patients can afford to pay for their own treatment, even the on-demand home therapy.
Hemophilia is an x-linked recessive genetic disorder characterized by low levels of essential clotting factors. The two most common types of hemophilia are factor VIII deficiency (hemophilia A, or classic hemophilia) and factor IX deficiency (hemophilia B, or Christmas disease).1,2 Globally, hemophilia affects approximately 400,000 people, with an estimated prevalence of 1 in 5000 male live births for hemophilia A, and 1 in 30,000 live births for hemophilia B.1,2 The clinical manifestations of hemophilia A and B are indistinguishable and occur in mild, moderate and severe forms. The severe form of hemophilia is often characterized by frequent hemarthroses, leading to chronic crippling hemarthropathy, when not treated very early or prophylactically.3
Replacement therapy has been the mainstay of treatment to manage hemophilia worldwide, both prophylactically and in treating bleeding, by providing the missing coagulation factor. Replacement therapy involves the use of highly purified factor concentrates, prepared from human plasma or manufactured by recombinant technology.3 In addition, incredible advances in recombinant bioengineering have led to newer therapies with easier modes of administration, decreased immunogenicity, increased efficacy and extended half-lives. Despite the availability of safe and effective treatment modalities, managing congenital bleeding disorders is considered complex mostly due to their familial nature, high morbidity, and significant physiological and psychosocial complications.4
The World Federation of Hemophilia (WFH) guidelines, introduced in 2005 and updated in 2012, offer practical recommendations to diagnose and manage hemophilia, providing guidance on managing complications, such as musculoskeletal issues, inhibitors and transfusion-related infections. However, there still exist multiple challenges in the funding and implementation of high-quality, guideline-driven, evidence-based hemophilia care.1 Firstly, the rarity of hemophilia may limit the recognition and availability of tools and resources to confirm a diagnosis, as well as restrict options to manage the disease and its complications.1 Additionally, funding may be inequitable, inconsistent, incomplete or absent and further complicated by political and bureaucratic processes.1
Adherence to treatment recommendations and follow-up is an ongoing challenge common to long-term medical conditions.1 Data suggests that up to 20 % of the people with hemophilia (PWH) do not follow their prescribed treatment.1 Differing healthcare reimbursement systems, budgetary constraints and geographical and cultural factors make it difficult for any country to deliver ideal care. Although developed countries have sufficient treatment products available, they are burdened by the higher expectation of outcomes, coupled with insufficient supportive care to monitor adherence and outcomes and the implementation of a regular follow-up.3 In contrast, developing regions may not have ready access to factor replacement, but have developed excellent physiotherapy and rehabilitation programs. Hence, it is impossible to compare and contrast care quality and create models of care as per resources alone. It is therefore imperative to move away from the pursuit of one perfect model and, as an alternative, learn from the global similarities and differences in delivering hemophilia care, building the best approach, tailored to each healthcare system and patient population.1 Although there are multiple studies that have attempted to assess country-specific variations in hemophilia care, very few compare hemophilia care between economically unequal healthcare systems and the challenges encountered in achieving optimal hemophilia care. This literature review tries to bridge this gap and throw light on the country-specific differences in epidemiology, standard of hemophilia care, and challenges faced in Canada and China.
MethodologyThe literature review attempted to identify all the available information on hemophilia care in Canada and China. The literature search was limited to hemophilia information available in these countries in the last two decades. The major search items included: – ‘Hemophilia’, ‘Hemophilia A’, ‘Hemophilia B’, ‘Canada’, ‘China’, ‘Management of Hemophilia’, ‘Treatment of Hemophilia’, ‘Challenges in Hemophilia care’ and ‘Challenges in Hemophilia management’. The researchers then conducted iterative searches in electronic databases, such as PubMed and Google Scholar. Furthermore, they appraised the references of selected articles for relevant material on the topic. The subject demanded a thorough and systematic search. Therefore, the data sources were not only limited to articles published in journals, but also included grey literature. The sources for grey literature were:
- •
Research forums,
- •
Institutional reports,
- •
Newsletters,
- •
Hemophilia society reports,
- •
Relevant websites,
- •
Popular internet search engines,
- •
Others (blogs, newsletters, and social media platforms).
The search strategy was broad and sensitive, in order to include as many relevant articles as possible, through subsequent manual screening. The researchers collected data through an extensive literature review process to present the consolidated information. A thematic analysis approach was used to analyze the data retrieved in this review (Figure 1). The findings were then presented and discussed in detail.
Results
The researchers retrieved a total of 280 articles on hemophilia care in Canada and China in the initial search with the mesh terms. Subsequently, abstract sifting yielded 65 relevant articles that described the hemophilia status, challenges in care and other related information in these countries. The common reason for exclusion was non-relevance and language other than English. Twenty citations met the inclusion criteria and were reviewed further (Figure 1).
The characteristics of the studies included:
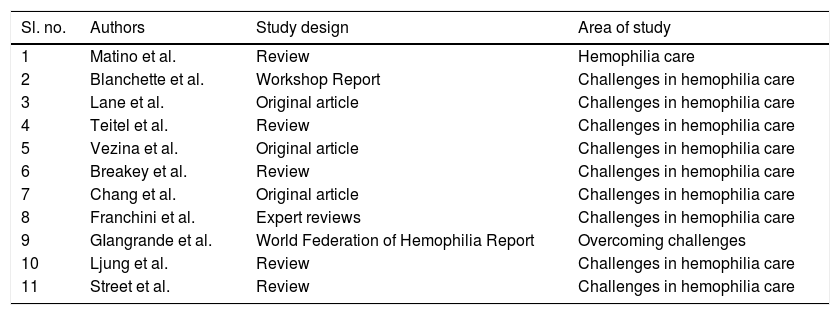
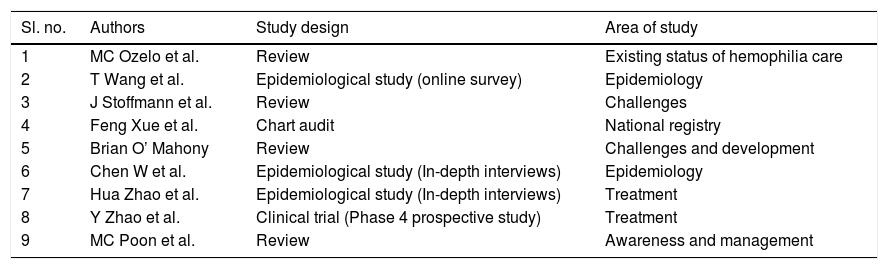
The literature search from PubMed and Google Scholar revealed 20 manuscripts, of which 11 were from Canada and nine were from China. Moreover, the grey literature search for relevant data in popular search engines yielded three sources for Canada and none for China. Among the 11 retrieved manuscripts on the hemophilia scenario in Canada, there were five literature reviews, three original articles, a workshop report, an expert review and a World Federation of Hemophilia report. Among the nine manuscripts appraised for China: four were reviews, three were epidemiological reviews, one clinical trial and one chart audit. The grey literature sources included annual reports from the hemophilia society in Canada. The characteristics of these studies are also listed in Tables 1 and 2.
The characteristics of studies included (Canada).
| Sl. no. | Authors | Study design | Area of study |
|---|---|---|---|
| 1 | Matino et al. | Review | Hemophilia care |
| 2 | Blanchette et al. | Workshop Report | Challenges in hemophilia care |
| 3 | Lane et al. | Original article | Challenges in hemophilia care |
| 4 | Teitel et al. | Review | Challenges in hemophilia care |
| 5 | Vezina et al. | Original article | Challenges in hemophilia care |
| 6 | Breakey et al. | Review | Challenges in hemophilia care |
| 7 | Chang et al. | Original article | Challenges in hemophilia care |
| 8 | Franchini et al. | Expert reviews | Challenges in hemophilia care |
| 9 | GIangrande et al. | World Federation of Hemophilia Report | Overcoming challenges |
| 10 | Ljung et al. | Review | Challenges in hemophilia care |
| 11 | Street et al. | Review | Challenges in hemophilia care |
The characteristics of studies included (China).
| Sl. no. | Authors | Study design | Area of study |
|---|---|---|---|
| 1 | MC Ozelo et al. | Review | Existing status of hemophilia care |
| 2 | T Wang et al. | Epidemiological study (online survey) | Epidemiology |
| 3 | J Stoffmann et al. | Review | Challenges |
| 4 | Feng Xue et al. | Chart audit | National registry |
| 5 | Brian O’ Mahony | Review | Challenges and development |
| 6 | Chen W et al. | Epidemiological study (In-depth interviews) | Epidemiology |
| 7 | Hua Zhao et al. | Epidemiological study (In-depth interviews) | Treatment |
| 8 | Y Zhao et al. | Clinical trial (Phase 4 prospective study) | Treatment |
| 9 | MC Poon et al. | Review | Awareness and management |
Grey literature:
AnalysisWe analyzed data from 18 sources on hemophilia in these countries and categorized them under four key themes covering the vital aspects of hemophilia care:
- •
Epidemiology of hemophilia
- •
Standard of hemophilia care
- •
Challenges in hemophilia care
- •
Ongoing transformation programs
Hemophilia leads to burdensome clinical repercussions and societal expenses. The clinical burden can be reduced by improving diagnosis and expanding access to prophylaxis treatment.5 A large multinational study on hemophilia is the hemophilia experience, results and opportunities (HERO) study on the self-reported outcomes of PWH from both developed and developing countries. The lives of PWH differed widely among countries as per the study.6,7 The PWH face more barriers for optimal treatment in developing countries than in developed ones due to limited healthcare resources.8
Canada: Hemophilia A and B affect about 2500 and 600 Canadians, respectively. (https://www.hemophilia.ca/hemophilia-a-and-b/).9 The Canadian Hemophilia Registry identified 3216 hemophilia A patients (males: 2,833, females: 333), 718 hemophilia B patients (males: 909, females: 109) and 4492 patients affected by von Willebrand Disease (vWD) in 2017. https://fhs.mcmaster.ca/chr/data.html.10
China: China ranks third (14,390 individuals with hemophilia) as per the World Federation of Hemophilia (WFH) Annual Global Survey (2016).11 However, owing to the huge population in China, the hemophilia population in the country could be around 80,000–120,000.8
Standard of hemophilia careCanada: The Canadian Hemophilia Society (CHS), founded in 1953, is affiliated with the World Federation of Hemophilia, which is officially recognized by the World Health Organization.12 The organization established a flexible and adaptable national standard of care with emphasis on uniformly high-quality care with the different associations comprising nurses, physiotherapists or social workers, as well as patients via the Canadian Hemophilia Society.1,12
A functional, efficient and accountable system of hemophilia care was initiated and developed in Canada by the comprehensive care centers.12 Canada has a national registry system that monitors home infusions. The information is entered electronically by patients and then analyzed to determine the appropriateness of the treatment regimen and track product inventories and utilization.1 Furthermore, strategies, such as telemedicine, are used to communicate with patients and their caregivers. Nurse coordinators connect extensively with patients by telephone. Some center teams conduct outreach clinics to smaller centers with a concentration of patients. Programs funded by the government or the local chapter of the CHS financially support families to travel to the hemophilia treatment centers (HTC) for annual assessments. Electronic infusion reporting systems are used to track product use.12
China: Hemophilia care has significantly progressed in China due to the contribution of the World Federation of Hemophilia (WFH) since 1993. However, both medical and non-medical interventions are far from satisfactory and only a small proportion of PWH are officially registered.13,14
The Hemophilia Treatment Center Collaborative Network of China (HTCCNC) was established in conjunction with the WFH in 2004 to improve hemophilia care in China.14 Several pharmaceutical companies and non-governmental organizations (NGOs) have helped to build and improve the six founding HTCs (Tianjin, Guangzhou, Shanghai, Beijing, Hefei and Jinan) comprising the HTCCNC.13 Lately, there has been a rapid growth in the number of HTCs – from six to 50 between 2004 and 2016 – and the work of the organization Hemophilia Home of China has increased public awareness on hemophilia, with a greater coverage of the cost of concentrates by health insurance companies.1
Challenges in hemophilia careThe challenges in hemophilia care in respective countries are presented below as per the country-specific perceptions (Figure 2).
Challenges in Canada
- 1
Under-diagnosis: There may be 30,000 Canadians with symptoms of bleeding disorders serious enough to require specialized care, yet only 8500 are registered in Canada’s comprehensive care centers. The CHS developed its CODE rouge program in 2011 to reach out to women with bleeding disorders.15,16 One in 100 Canadians, men and women, carry an inherited bleeding disorder gene and more than 35,000 have symptoms severe enough for medical care. Yet, many have not been properly diagnosed, particularly the people of Aboriginal origin.15,16 One reason for the delay in the diagnosis of hemophilia or treatment for a bleed in the Aboriginal people is that they live far from the regions where HTCs are concentrated.17
- 2
Inhibitor development: Since the advent of an adequate supply of safe clotting factor concentrates in Canada since the1990s, the major challenge in the treatment of hemophilia is inhibitors.18,19 People of African-American origin in Canada are twice at the risk of developing inhibitors. This may be because recombinant concentrates were developed using FVIII haplotypes from a white population.15,16,20
- 3
Aging with Hemophilia: Advances in hemophilia care since the 1950s have contributed to an overall improved life expectancy and quality of life in Canada. Hence, people with hemophilia can experience age-related clinical problems previously unobserved among them. Moreover, they suffer from the long-term effect of existing complications, such as liver problems secondary to hepatitis or further mobility problems related to hemophilic arthropathy. The improved life expectancy brings new challenges to bleeding disorder healthcare providers, particularly in Canada.15,16,21
- 4
The ‘sneaky’ effects of prophylaxis: Primary prophylaxis (preventative factor replacement therapy) is considered the gold standard of care for hemophilia in Canada, as most individuals generally experience only minor bleeding and have few or no major bleeding episodes in their joints, muscles or soft tissues. Therefore, many patients start feeling invulnerable and return too quickly to their activities (such as walking, running or sports) or partake in inappropriate activities or career choices with serious short-, medium-, and long-term repercussions for their musculoskeletal health. In addition, the introduction of home treatment and prophylaxis is considered to be a double-edged sword. “People with hemophilia have gained a lot of autonomy and their health status has been substantially improved; however, now some young people with hemophilia only come to the HTCs to pick up their coagulation products. They neglect the importance of being monitored by the HTC’s multidisciplinary team, particularly when they regard the injuries as being minor”.15,16,22
- 5
Charting the CHARMS Course: A key component of the system for collecting data is the Canadian Hemophilia Assessment and Resource Management Information System (CHARMS). It was developed and implemented across Canada in 1998. However, the present structure of CHARMS is not optimal. The information patients collect, with old paper ‘bleed sheets’ or newer electronic systems based on the web or handheld devises must be manually fed into CHARMS, as is information about product distribution. All this work is unnecessarily time- and human resource-intensive.15,16
- 1
Poor healthcare infrastructure: China’s health coverage system is complex and extremely variable among cities, rural areas and provinces and often excludes hemophilia. The situation is exacerbated because most hospitals with the capacity to diagnose and care for PWH are localized to the east of China, along the more economically developed coastline. Patients living in smaller cities and rural areas are often misdiagnosed or not diagnosed at all; care in these areas is limited and treatment is usually neither available nor affordable.13 This, in combination with social exclusion, means that Chinese PWH also experience a significantly lower quality of life, compared to the healthy male population.23
- 2
Poor management of registries: Registries comprising either individual or aggregate patient data can further the understanding of variations in treatment; describe care patterns, including appropriateness and disparities in the delivery and quality of care; examine factors that influence prognosis and quality of life, and; provide evidence on resource utilization.24 Patient members of the National Registered Center in China are now more than 13,000 and the data is used to improve diagnosis rates and hemophilia knowledge and explore China’s national treatment environment.1 However, the current registry does not provide information on mortality and does not allow for continuous vigilance on treatment regimens. The existing registry contains only 10 % of the estimated population. Most diagnosed hemophiliacs belong to areas with better economy and healthcare infrastructure. The large population of unidentified hemophiliacs belongs to the less developed areas, especially rural areas. Identifying the patients and maintaining a registry is an essential component for policy decision-making.25
- 3
Lack of awareness: China has a large population and a vast territory. Therefore, it also has the largest number of people with hemophilia in the world. However, there are many patients with no access to proper treatment and information on hemophilia treatment and care. They live in isolation with a sense of loneliness and helplessness.26
- 4
Lack of reimbursement schemes: Hemophilia, a costly yet treatable rare disease, receives 100% reimbursement coverage in most developed and some developing countries. The Chinese Ministry of Health announced in 2012 that 20 high-cost diseases (including hemophilia) should be prioritized to ease the economic burden of patients with hemophilia. A study from China in 2013 on the reimbursement policies of three major social insurance schemes reported that, while there is a significant variation among cities, the average co-pay requirement is more than 50% and the annual reimbursement is usually capped below USD16k (100k CNY). Hemophilia treatment reimbursement in China is still at a low level and there is a need for unique approaches to reduce the economic burden of patients with hemophilia.27
- 5
Lack of home therapy: Hemophilia patients depend on infusions of clotting factors throughout their lives. Transient treatments at hospitals do not guarantee effectiveness in controlling the disease. Thus, home therapy or personalized care is particularly important for hemophiliacs. Home therapy for hemophilia is the prevention, evaluation and treatment of bleeding that occurs at home for the hemophiliac and/or their family members. Home therapy is helpful for the early treatment of bleeding and the reduction of pain and the risk of deformity and hospitalizations associated with complications.28 However, a recent study from the Shanxi province reported that home therapy for hemophilia remains in a preliminary stage due to certain obstacles.29 Certain factors behind unsuccessful home therapy are:
- 6
Lack of professional knowledge and home therapy skills,
- 7
Lack of confidence in carrying out home therapy,
- 8
Limited access to therapy.
- 9
Low usage of prophylaxis care: Primary prophylaxis is usually not possible in China because of inadequate resources, particularly in rural areas. Hence, joint outcomes and quality of life (QoL) are worse in China compared to developed countries, where primary prophylaxis is the standard care.30 Nearly 75% of the patients with hemophilia in China have a moderate/severe degree of arthropathy. Nonadherence to prophylaxis is possibly due to differences in patient expectations and communication of the benefits from the hemophilia treatment center. There is a critical need for a more widespread development of the comprehensive hemophilia care teams and education to modify the attitude of the patients/parents and other healthcare workers in accepting the importance of preventive care (in addition to acute care), including prophylaxis.31
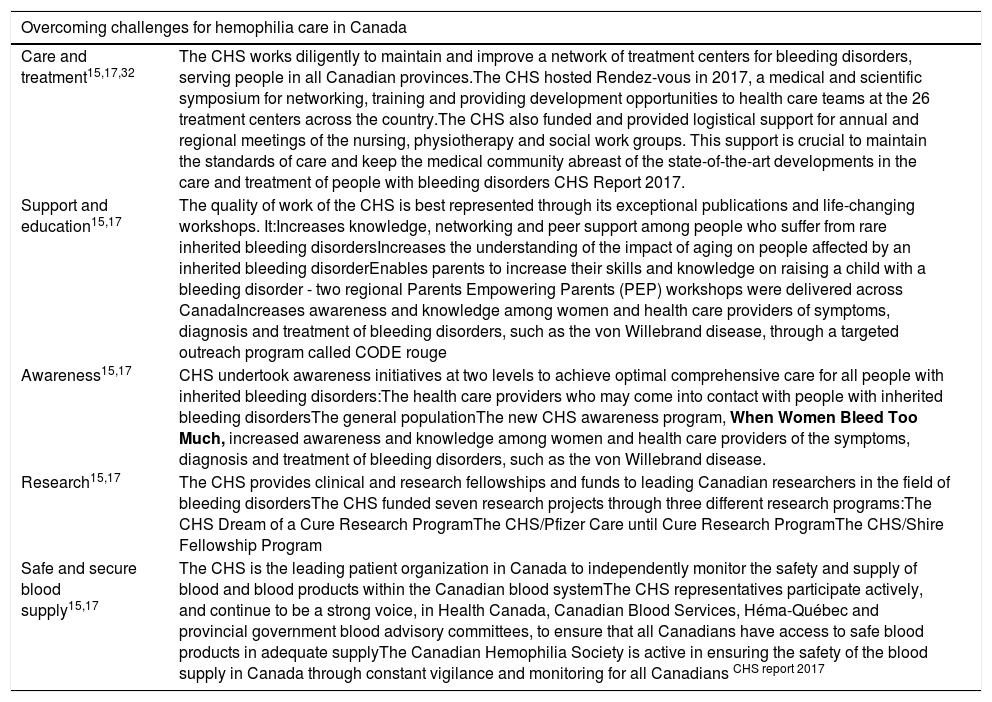
Challenges can be barriers to progress, but they can also be opportunities to innovate and grow. The challenges faced by both the countries differ markedly. Some innovative measures have been taken up by the respective countries to overcome the challenges and other countries can also take these to improve hemophilia care (Table 3).
Overcoming challenges.
| Overcoming challenges for hemophilia care in Canada | |
|---|---|
| Care and treatment15,17,32 | The CHS works diligently to maintain and improve a network of treatment centers for bleeding disorders, serving people in all Canadian provinces.The CHS hosted Rendez-vous in 2017, a medical and scientific symposium for networking, training and providing development opportunities to health care teams at the 26 treatment centers across the country.The CHS also funded and provided logistical support for annual and regional meetings of the nursing, physiotherapy and social work groups. This support is crucial to maintain the standards of care and keep the medical community abreast of the state-of-the-art developments in the care and treatment of people with bleeding disorders CHS Report 2017. |
| Support and education15,17 | The quality of work of the CHS is best represented through its exceptional publications and life-changing workshops. It:Increases knowledge, networking and peer support among people who suffer from rare inherited bleeding disordersIncreases the understanding of the impact of aging on people affected by an inherited bleeding disorderEnables parents to increase their skills and knowledge on raising a child with a bleeding disorder - two regional Parents Empowering Parents (PEP) workshops were delivered across CanadaIncreases awareness and knowledge among women and health care providers of symptoms, diagnosis and treatment of bleeding disorders, such as the von Willebrand disease, through a targeted outreach program called CODE rouge |
| Awareness15,17 | CHS undertook awareness initiatives at two levels to achieve optimal comprehensive care for all people with inherited bleeding disorders:The health care providers who may come into contact with people with inherited bleeding disordersThe general populationThe new CHS awareness program, When Women Bleed Too Much, increased awareness and knowledge among women and health care providers of the symptoms, diagnosis and treatment of bleeding disorders, such as the von Willebrand disease. |
| Research15,17 | The CHS provides clinical and research fellowships and funds to leading Canadian researchers in the field of bleeding disordersThe CHS funded seven research projects through three different research programs:The CHS Dream of a Cure Research ProgramThe CHS/Pfizer Care until Cure Research ProgramThe CHS/Shire Fellowship Program |
| Safe and secure blood supply15,17 | The CHS is the leading patient organization in Canada to independently monitor the safety and supply of blood and blood products within the Canadian blood systemThe CHS representatives participate actively, and continue to be a strong voice, in Health Canada, Canadian Blood Services, Héma-Québec and provincial government blood advisory committees, to ensure that all Canadians have access to safe blood products in adequate supplyThe Canadian Hemophilia Society is active in ensuring the safety of the blood supply in Canada through constant vigilance and monitoring for all Canadians CHS report 2017 |
| Overcoming challenges for hemophilia care in China | |
|---|---|
| Improving comprehensive care14 | A number of HTCCNC member hematologists (11), physiatrist (one), nurses (five) and laboratory scientist (one) have received or will be receiving the WFH short-term (5–8 weeks) fellowships for targeted training at various WFH IHTC since 1997These trained personnel are now in leadership roles at their own centers – and many are chairing the various HTCCNC working groups. They are in a position to develop comprehensive hemophilia care in the true senseFor example, Beijing formed a consortium of four hospitals to provide comprehensive care to adults and children, in addition to emergency care and special diagnostic testing. |
| Innovative reimbursement schemes24 | Some cities in China pioneered innovative policies for a better coverage for hemophilia patients, such as:The Guangzhou health insurance bureau decreased hemophilia co-payments to less than 10% after their extensive review of the economics of hemophilia treatmentThe local health insurance bureau in Qingdao decided to joint-fund prophylaxis treatment for pediatric patients with a FVIII manufacturer. |
| Improving awareness23 | Some patients created a website named Hemophilia Home of China (HHC) (www.xueyou.org) in May 2000. The hemophilia patient organization, the Hemophilia Home of China, was established in October 2000 because of the websiteThe HHC website was updated in 2003 with the support and assistance of the WFH. The updated website includes basic knowledge, Chinese traditional medicine, treatment guides, media reports, online doctor services, registration of patients, hemophilia news, knowledge of hemophilia, hemophilia experience, hemophilia life, online surveys, e-magazines, chat room, guestbook, forums and other itemsSix experts, including a pediatrician, emergency physician, nurse, dentist, psychologist and physiotherapist, contribute their time and energy to answer patient questions on hemophilia through the websiteMoreover, prominent national hemophilia experts are invited to deliver hemophilia-related lectures via a video chat room and answer patient questionsThis gives many patients in remote areas the opportunity to consult these experts face-to-face. The HHC website not only gives them knowledge and information, but also provides a platform for them to communicate with the outside world |
| Improving the usage rate of the prophylaxis regimen13 | The HTTCNC, which includes a prophylaxis working group, was established with the WFH to improve the care of PWHThe HTCCNC began studies evaluating the delivery of low-dose prophylaxis in boys with severe hemophilia A (10 IU/kg twice a week) and hemophilia B (20IU/kg weekly) due to the lack of affordability of standard full-dose prophylaxis for most families in China1 |
| Twinning program with Canada14,33 | A twinning program was initiated in China from 1997 to 2007 by the WFH. The earlier six China HTCs were twinned with Canadian HTCs; China became a WFH Global Alliance for Progress (GAP) Program member in 2009 to improve the diagnosis and treatment of people with hemophilia with the successful conclusion of the WFH Center Twinning Program in China at the end of 2007 |
| Ongoing projects to improve hemophilia in China | Hemophilia Data Management System ProjectGlobal Alliance for ProgressNovo Nordisk Hemophilia Foundation - Phase I and IIChina Hemophilia Treatment Center ProjectKogenate FS Patient Assistance Program |
The early treatment of bleeding episodes and home therapy has quickly evolved as the primary management option in developed countries. The presence of specialized interdisciplinary centers with 24-h service, training and education of patients are the main advantages of the comprehensive treatment concept in developed countries. This is not the case in most developing countries where the government does not have the resources to buy the necessary quantities of coagulation factors in the face of more urgent health priorities and hardly a few patients can afford to pay for their own treatment, even for on-demand home therapy. Other problems are the insufficient supply of clotting factor concentrates, the lack of access to these concentrates and the absence of specialized care centers.
Hemophilia societies must develop national policies and goals, understand the realities of their regions and acknowledge the global reality for people with hemophilia. While national differences in management of hemophilia are clearly evident, the hemophilia community is one global community and the members should advise and assist each other in reaching their mutual goals.
The common global strategies to improve hemophilia care worldwide are:
- I
Global guidelines and protocols: There is a need to build evidence-based algorithms/protocols, depending on local/national needs. Global guidelines can even be adapted for those PWH living some distance away from treatment centers.
- II
Government support: The governments must actively become involved in allocating resources to hemophilia care.
- III
Care delivery: Hemophilia treatment centers provide hemophilia services throughout a country. The care delivery system must be robust in the country to reach out to all the sections of the society.
- IV
Collaboration: There is a need for global collaboration to optimize the delivery of care and education to match the needs of PWH. International networks must be created to train medical professionals. Collaboration calls for the sharing of research ideas in the disease environment. Global collaboration would also improve access to various hemophilia treatment products.
- V
Maintaining registries: Registries are a benchmark to optimize care for hemophilia. They help to track resource utilization. Registries provide information on the use of treatment products, including the monitoring of prophylaxis and immune tolerance induction (ITI) data, which is not always gathered by healthcare providers within the formal setting of the HTC. Real-time patient data is necessary to raise awareness on hemophilia and highlight the burden of the disease, particularly in terms of quality of life, and establish key epidemiological benchmarks. Treatment and outcomes data must be used to develop cost utility arguments to drive improvements in resourcing hemophilia care. This promotes the gathering of the relevant evidence for better care.
- VI
Personalized care: Personalized care must be enhanced in countries with limited resources to improve treatment adherence and outcomes. It is vital to identify the various barriers to personalized care and strategies to improve the same.
- VII
Patient organizations: Patient organizations play a vital role in hemophilia care and should be encouraged at the global and national levels. Developing and sustaining an effective national patient organization requires many skills, much perseverance and an integral approach, including volunteers, staff and key clinicians. They must be trained on effective management, public relations skills, fundraising, advocacy and patient education.
The ultimate aim is to make a difference in the lives of people with haemophilia, regardless of the unique challenges in each country.
Conflict of interestWe wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.



