

Blood is a valuable life resource that depends on the donation of blood by the community. As a result, it is crucial that the manner in which this expensive resource is used be correct and reasonable.
ObjectiveThe purpose of this study was to investigate the Maximum Blood Ordering for Surgery (MSBOS) in general, orthopedic and neurosurgical elective surgeries at the Poursina Hospital in Rasht in 2017.
MethodsAccording to the patient file number information, such as gender, age, type of surgery, number of blood units requested, number of cross-matched blood units, number of blood units transfusion, number of patients undergoing transfusion, number of patients who were cross-matched, initial hemoglobin and the underlying disease, was extracted from the HIS (Hospital Information System). Based on the collected data, a descriptive report of the cross-match to transfusion ratio (C/T), transfusion index (TI) and transfusion probability (%T) was performed, using average and standard deviation, by using the SPSS 16.
ResultsIn the present study, 914 patients from the neurosurgery, orthopedic and general surgery wards of the Poursina Hospital were studied. Of these, 544 were male (59.5%) and 370 were female (40.5%), aged 1–99 years, with a mean age of 43 years. The frequency distribution of C/T in this study was 1.29 in neurosurgery, 1.95 in orthopedic surgery and 1.96 in general surgery.
This study indicated that the C/T index was above the normal standard level in four different kinds of surgery, including leg fracture (2.71), cholecystectomy(2.71), forearm fracture (2.70), and skin graft (2.62).The C/T index was at the maximum normal level in thyroidectomy surgery (2.5). The other surgeries had the normal C/T index.
ConclusionOverall, all of the MSBOS indices were at the standard level in this study, although C/T indices were higher than the standard level in the surgeries for cholecystectomy, leg fracture, forearm fracture, hand fracture and skin graft.
Blood is a valuable life resource that depends on the donation of blood by the community. As a result, it is crucial that the manner in which this expensive resource is used be correct and reasonable.
In the United States, it is estimated that about 24 million units of blood and blood products are used annually for various diseases and injuries.1,2
Blood transfusion is a common pre-operative process that requires 3 pre-transfusion processes, including blood cross-matching to find the appropriate blood product for the patient, which may not be used after all. Studies showed that in Africa, about 7–10 percent of all blood units are lost due to the excessive demand for blood.2,3
Some disadvantages of unnecessary cross-matching are increased workloads in blood transfusion laboratories, loss of blood supply due to the expiration date and increased medical care costs.1
Numerous evidence-based studies and guidelines by different nationalities emphasize the reduction in the use of blood units in surgical operations.4
Studies have suggested that cross-matched blood (at least 2 units) should be available before cardiac surgery due to the increased risk of bleeding in people undergoing cardiac surgery. However, recent studies have indicated that about 50% of people undergoing cardiac surgery did not receive any blood units.5
Numerous guidelines have been designed to determine the number of blood units required before surgery, including the MSBOS (Maximum Surgical Blood Ordering Schedule) which was first introduced in the 1970s. This guideline consists of tables showing the number of blood units that are routinely cross-matched for each specific surgery, eliminating unnecessary preoperative tests, improving costs, reducing the number of cross-matched blood units and assisting the blood bank management.3,6–9
Many efforts have been made to improve this model due to the improvement of surgical technologies and new surgeries, such as laparoscopy. At each hospital, blood sampling programs are developed in collaboration with blood bank staff and major blood users, including surgeons and anesthesiologists.10,11
Accordingly, a study based on the MSBOS model at the Firoozgar Hospital in Tehran in 2002 and a similar study at Jahrom hospitals in 2014 showed a high C/T ratio (cross-match to transfusion ratio), as well as a lower percentage of cross-matched blood units used.12,13
According to previous studies on orthopedic and urological surgeries in the Guilan Province, the results indicated unfavorable blood transfusion conditions in the surgeries, but there are no studies on general surgeries and neurosurgeries in this province.
The purpose of this study was to investigate the Maximum Blood Order for Surgery (MSBOS) in general, orthopedic and neurosurgical elective surgeries at the Poursina Hospital in Rasht in 2017. The results of this study can be used to inform all those involved in the process of blood transfusion, with subsequent improvements in costs, time, and laboratory work.
Material and methodsTo obtain the required information, a list was initially compiled which comprised all those for whom blood units were prepared up to 72h after they had gone under general anesthesia in orthopedic surgery, neurosurgery and general surgery in 2017. Patients undergoing emergency surgery, patients with coagulopathy, febrile patients, patients with hemoglobin levels below 7 and patients with a history of reaction to blood transfusions were excluded. After the selection of patients for this study, based on the mentioned inclusion and exclusion criteria, 914 patients were chosen for the current study from 9 types of surgeries in the orthopedic ward, 4 types of surgeries in the neurosurgery ward and 11 types of surgeries in the general surgery ward. According to the patient file number, the information, such as gender, age, type of surgery, number of blood units requested, number of cross-matched blood units, number of blood units transfused, number of patients undergoing transfusion, number of patients who were cross-matched, initial hemoglobin and the underlying disease, was extracted from the HIS (Hospital Information System). The following three main indices were used to evaluate the use of blood units:

A ratio lower than or equal to 2.5 was considered indicative of significant blood usage.

A value greater than or equal to 30% was considered indicative of significant blood usage.

A value greater than or equal to 0.5 was considered indicative of significant blood utilization.14
Based on the collected data, a descriptive report of C/T, TI, and %T was performed by using the SPSS 16. The descriptive analysis of quantitative variables was stated by using the mean and the standard deviation. The relative and absolute frequencies (percentages) were used to report the descriptive analysis of categorical variables.
ResultsIn the present study, 914 patients from the neurosurgery, orthopedic and general surgery wards at the Poursina Hospital were studied. Of these, 544 were male (59.5%) and 370 were female (40.5%), aged 1–92 years, with a mean age of 43.76 years (standard deviation (SD)=18.76).
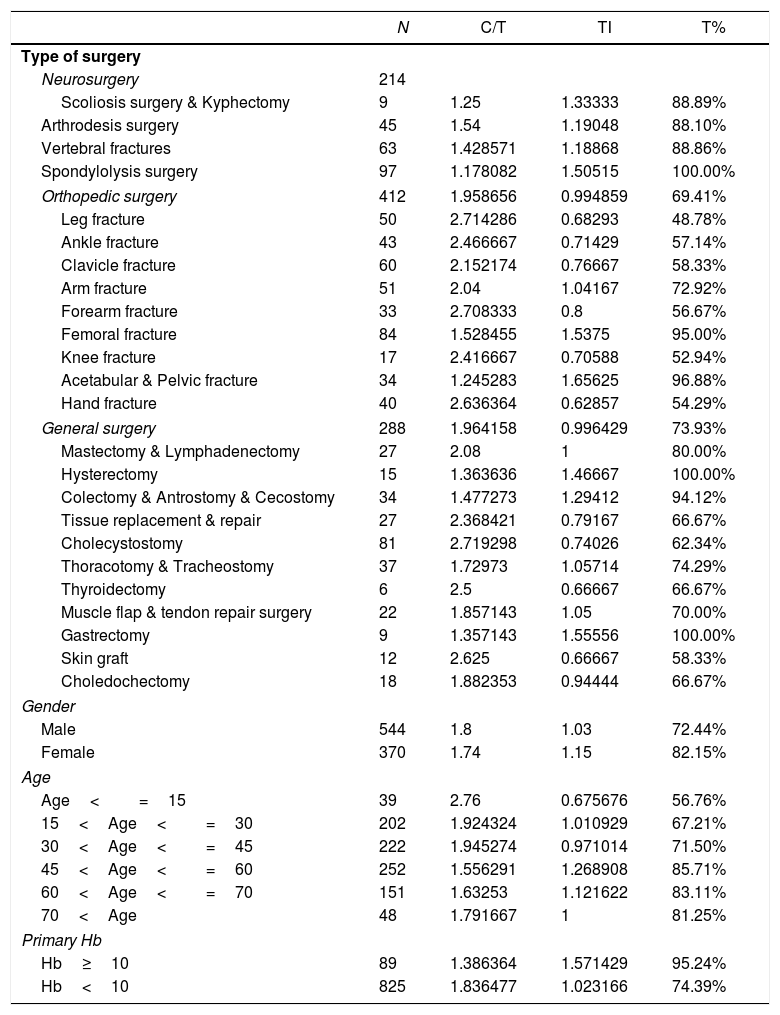
Twenty-four different surgeries in 3 wards were surveyed in this study. The greatest number of cases were spondylolysis surgeries (97) and the fewest, thyroidectomies (6).
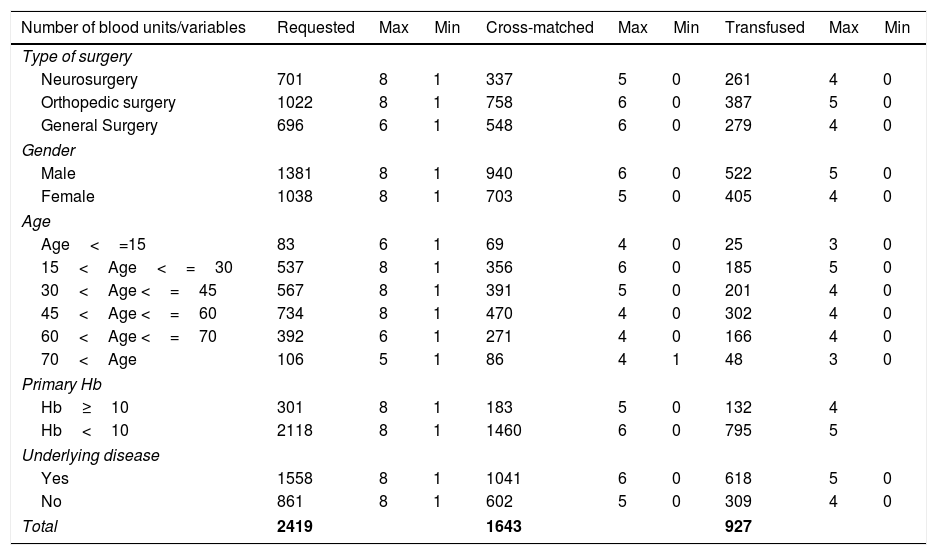
Two hundred and fourteen participants (23.4%) were from the neurosurgery ward, 412 (45.1%) from the orthopedic surgery ward and 288 (31.5%) from the general surgery ward. The minimum number of blood units requested for these three wards was 1 and the maximum number, 8 (Table 1). The frequency distribution of C/T in this study was 1.29 in neurosurgery, 1.95 in orthopedic surgery and 1.96 in general surgery. The highest C/T index was in leg fracture surgery (2.71) and cholecystectomy (2.71) and the lowest, in spondylolysis surgery (1.17), as shown in Table 2.
Distribution number of blood units based on different variables.
| Number of blood units/variables | Requested | Max | Min | Cross-matched | Max | Min | Transfused | Max | Min |
|---|---|---|---|---|---|---|---|---|---|
| Type of surgery | |||||||||
| Neurosurgery | 701 | 8 | 1 | 337 | 5 | 0 | 261 | 4 | 0 |
| Orthopedic surgery | 1022 | 8 | 1 | 758 | 6 | 0 | 387 | 5 | 0 |
| General Surgery | 696 | 6 | 1 | 548 | 6 | 0 | 279 | 4 | 0 |
| Gender | |||||||||
| Male | 1381 | 8 | 1 | 940 | 6 | 0 | 522 | 5 | 0 |
| Female | 1038 | 8 | 1 | 703 | 5 | 0 | 405 | 4 | 0 |
| Age | |||||||||
| Age<=15 | 83 | 6 | 1 | 69 | 4 | 0 | 25 | 3 | 0 |
| 15<Age<=30 | 537 | 8 | 1 | 356 | 6 | 0 | 185 | 5 | 0 |
| 30<Age <=45 | 567 | 8 | 1 | 391 | 5 | 0 | 201 | 4 | 0 |
| 45<Age <=60 | 734 | 8 | 1 | 470 | 4 | 0 | 302 | 4 | 0 |
| 60<Age <=70 | 392 | 6 | 1 | 271 | 4 | 0 | 166 | 4 | 0 |
| 70<Age | 106 | 5 | 1 | 86 | 4 | 1 | 48 | 3 | 0 |
| Primary Hb | |||||||||
| Hb≥10 | 301 | 8 | 1 | 183 | 5 | 0 | 132 | 4 | |
| Hb<10 | 2118 | 8 | 1 | 1460 | 6 | 0 | 795 | 5 | |
| Underlying disease | |||||||||
| Yes | 1558 | 8 | 1 | 1041 | 6 | 0 | 618 | 5 | 0 |
| No | 861 | 8 | 1 | 602 | 5 | 0 | 309 | 4 | 0 |
| Total | 2419 | 1643 | 927 | ||||||
Max: maximum number of units which was requested, cross-matched or transfused for each patient; Min: minimum number of units which was requested, cross-matched or transfused for each patient.
Descriptive analysis of variables.
| N | C/T | TI | T% | |
|---|---|---|---|---|
| Type of surgery | ||||
| Neurosurgery | 214 | |||
| Scoliosis surgery & Kyphectomy | 9 | 1.25 | 1.33333 | 88.89% |
| Arthrodesis surgery | 45 | 1.54 | 1.19048 | 88.10% |
| Vertebral fractures | 63 | 1.428571 | 1.18868 | 88.86% |
| Spondylolysis surgery | 97 | 1.178082 | 1.50515 | 100.00% |
| Orthopedic surgery | 412 | 1.958656 | 0.994859 | 69.41% |
| Leg fracture | 50 | 2.714286 | 0.68293 | 48.78% |
| Ankle fracture | 43 | 2.466667 | 0.71429 | 57.14% |
| Clavicle fracture | 60 | 2.152174 | 0.76667 | 58.33% |
| Arm fracture | 51 | 2.04 | 1.04167 | 72.92% |
| Forearm fracture | 33 | 2.708333 | 0.8 | 56.67% |
| Femoral fracture | 84 | 1.528455 | 1.5375 | 95.00% |
| Knee fracture | 17 | 2.416667 | 0.70588 | 52.94% |
| Acetabular & Pelvic fracture | 34 | 1.245283 | 1.65625 | 96.88% |
| Hand fracture | 40 | 2.636364 | 0.62857 | 54.29% |
| General surgery | 288 | 1.964158 | 0.996429 | 73.93% |
| Mastectomy & Lymphadenectomy | 27 | 2.08 | 1 | 80.00% |
| Hysterectomy | 15 | 1.363636 | 1.46667 | 100.00% |
| Colectomy & Antrostomy & Cecostomy | 34 | 1.477273 | 1.29412 | 94.12% |
| Tissue replacement & repair | 27 | 2.368421 | 0.79167 | 66.67% |
| Cholecystostomy | 81 | 2.719298 | 0.74026 | 62.34% |
| Thoracotomy & Tracheostomy | 37 | 1.72973 | 1.05714 | 74.29% |
| Thyroidectomy | 6 | 2.5 | 0.66667 | 66.67% |
| Muscle flap & tendon repair surgery | 22 | 1.857143 | 1.05 | 70.00% |
| Gastrectomy | 9 | 1.357143 | 1.55556 | 100.00% |
| Skin graft | 12 | 2.625 | 0.66667 | 58.33% |
| Choledochectomy | 18 | 1.882353 | 0.94444 | 66.67% |
| Gender | ||||
| Male | 544 | 1.8 | 1.03 | 72.44% |
| Female | 370 | 1.74 | 1.15 | 82.15% |
| Age | ||||
| Age<=15 | 39 | 2.76 | 0.675676 | 56.76% |
| 15<Age<=30 | 202 | 1.924324 | 1.010929 | 67.21% |
| 30<Age<=45 | 222 | 1.945274 | 0.971014 | 71.50% |
| 45<Age<=60 | 252 | 1.556291 | 1.268908 | 85.71% |
| 60<Age<=70 | 151 | 1.63253 | 1.121622 | 83.11% |
| 70<Age | 48 | 1.791667 | 1 | 81.25% |
| Primary Hb | ||||
| Hb≥10 | 89 | 1.386364 | 1.571429 | 95.24% |
| Hb<10 | 825 | 1.836477 | 1.023166 | 74.39% |
In the present study, 6 different age groups were studied, including patients under 15 years, 15–30 years, 30–45 years, 45–60 years, 60–75 years and over 75 years. The lowest number of cross-matched blood units was zero and the highest was 6 (Table 1). The frequency distribution of the C/T index in this study showed that the greatest index was 2.76 in participants under 15 years and the lowest, 1.55 in participants 45–60 years. The C/T index in this study was 1.80 in male participants and 1.74 in female participants (Table 2).
This study indicated that the lowest participant primary hemoglobin was 7g/dL and the highest, 17g/dL. The patients were divided into 2 groups, based on primary hemoglobin over 10g/dL and below 10g/dL. The C/T was 1.38 in participants with hemoglobin above 10g/dL and 1.83 in participants with hemoglobin below 10g/dL. In the present study, 349 participants (38%) had no underlying disease and 565 (61%) participants had at least one underlying disease (Table 2).
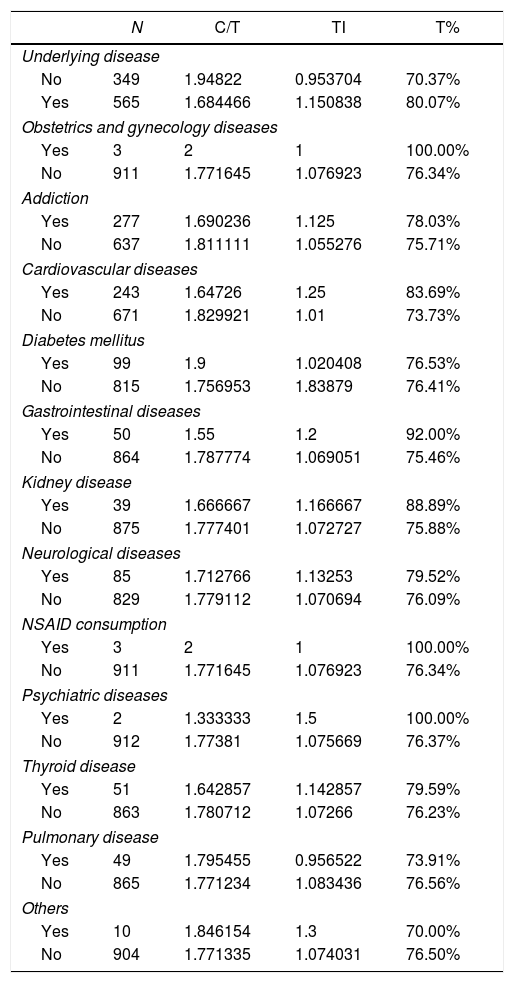
According to Table 3, the highest frequency was related to the history of addiction and tobacco use with 277 cases (30%), and the lowest frequency was related to the history of psychiatric disease, with 2 cases (0.21%). This study noted that the C/T index was 1.94 in participants without any underlying disease and 1.68 in participants with at least one underlying disease (Table 2).
Descriptive analysis of underlying disease.
| N | C/T | TI | T% | |
|---|---|---|---|---|
| Underlying disease | ||||
| No | 349 | 1.94822 | 0.953704 | 70.37% |
| Yes | 565 | 1.684466 | 1.150838 | 80.07% |
| Obstetrics and gynecology diseases | ||||
| Yes | 3 | 2 | 1 | 100.00% |
| No | 911 | 1.771645 | 1.076923 | 76.34% |
| Addiction | ||||
| Yes | 277 | 1.690236 | 1.125 | 78.03% |
| No | 637 | 1.811111 | 1.055276 | 75.71% |
| Cardiovascular diseases | ||||
| Yes | 243 | 1.64726 | 1.25 | 83.69% |
| No | 671 | 1.829921 | 1.01 | 73.73% |
| Diabetes mellitus | ||||
| Yes | 99 | 1.9 | 1.020408 | 76.53% |
| No | 815 | 1.756953 | 1.83879 | 76.41% |
| Gastrointestinal diseases | ||||
| Yes | 50 | 1.55 | 1.2 | 92.00% |
| No | 864 | 1.787774 | 1.069051 | 75.46% |
| Kidney disease | ||||
| Yes | 39 | 1.666667 | 1.166667 | 88.89% |
| No | 875 | 1.777401 | 1.072727 | 75.88% |
| Neurological diseases | ||||
| Yes | 85 | 1.712766 | 1.13253 | 79.52% |
| No | 829 | 1.779112 | 1.070694 | 76.09% |
| NSAID consumption | ||||
| Yes | 3 | 2 | 1 | 100.00% |
| No | 911 | 1.771645 | 1.076923 | 76.34% |
| Psychiatric diseases | ||||
| Yes | 2 | 1.333333 | 1.5 | 100.00% |
| No | 912 | 1.77381 | 1.075669 | 76.37% |
| Thyroid disease | ||||
| Yes | 51 | 1.642857 | 1.142857 | 79.59% |
| No | 863 | 1.780712 | 1.07266 | 76.23% |
| Pulmonary disease | ||||
| Yes | 49 | 1.795455 | 0.956522 | 73.91% |
| No | 865 | 1.771234 | 1.083436 | 76.56% |
| Others | ||||
| Yes | 10 | 1.846154 | 1.3 | 70.00% |
| No | 904 | 1.771335 | 1.074031 | 76.50% |
Restriction of the excessive blood unit usage before surgery is an important aspect in the enhancement of patient safety, reducing the cost and waste of blood transfusion. Excessive request for cross-matched blood can limit the access to blood units the patient needs, increase the burden on the blood bank staff, reduce blood bank reserves, allow blood units to expire and increase hospital treatment costs. To prevent the above, guidelines such as the MSBOS, have been created.4
Based on the results of the present study, in general, all the indices of the MSBOS (TI=1.07, T%=76.42, C/T=1.77) were within the normal range (TI≥0.5, T%≥30%, C/T≤2.5) in this hospital. However, the number of blood units requested (2419) in this academic center was significantly higher than the cross-matched (1643) and transfused (927) blood units, so only 67.92% of the total blood units requested were crossmatched and 38.32% of all requested blood units were transfused. As an example, for an arthrodesis surgery in the neurosurgery department, eight units of blood were requested. Only five units of them were crossmatched and two units were transfused. Due to a defect in the recording of information in the HIS system, the data on neurosurgery and thyroidectomy operations were less than those for other surgeries.
In the present study, the MSBOS indices were evaluated in different surgeries, although overall values were within the standard level, the C/T index in cholecystectomy (2.719), calf fracture (2.714), forearm fracture (2.70), hand fracture (2.63) and skin graft surgeries (2.62), respectively, was higher than the standard level, the highest being in thyroidectomy surgeries (2.5). Other surgeries were within the normal range (Figure 1). Past studies showed a similar result, compared to the present study. In the study of Hosseini et al., 2016, on cholecystectomy surgeries, none of the MSBOS indices were within the standard level (C/T=20, TI=0.1, T%=7.5%).15 Adegboye et al., 2018, indicated that none of the MSBOS indices were at the standard level in forearm fracture surgeries in their study (T%=12.5%, C/T=15, TI=0.12). However, the standard limit set in this study was different from the present study (T%>50%, C/T<2, TI>0.5). Moreover, all the MSBOS indices in tibiofibular fracture surgeries were not within standard range (T%=0%, C/T=0, TI=0). In their study, 3 patients underwent leg fracture surgery, 6 blood units were requested, and 2 units were cross-matched, but none of them were transfused.2 In the studies by Khalili et al., 2002, (C/T=11.8, T%=8.69, TI=0.26) and Hosseini et al., 2016, (C/T=20.3, TI=0.1, T%=9.3%), all the MSBOS indices were higher than standard levels in thyroidectomy surgeries.12,15

In the present study, all the MSBOS indices were totally within the standard level in all age groups, although the C/T index (2.76) was higher than the established standard in the under 15 years group, requiring further study to establish the cause. Other age groups had desirable MSBOS indices at the standard level. In the study by Soleimanha et al., 2015, the highest C/T was in those under 20 years (4.48). However, only orthopedic surgeries were studied in their study.11
In the present study, both groups (hemoglobin less than 10 and hemoglobin greater than 10) had the standard indices. However, those with hemoglobin higher than 10 had indices closest to the standard level. In the study by Khoshrang et al., 2013, pre-operative hemoglobin was identified as an influencing factor in increasing the demand for blood and cross-matched units, so the individuals with hemoglobin less than 7 had higher MSBOS indices than the other groups (p<0.380).16 In the study by Feliu et al., 2014, the MSBOS indices obtained in the group with hemoglobin over 10 were not at the standard level (T%=8, C/T=8.62, TI=0.11).17
In the present study, in the evaluation of the MSBOS indices in patients with underlying disease, all the indices were at the standard level. However, the individuals without any underlying disease had indices closer to the standard level, compared to those with at least one underlying disease. Some individuals may have multiple underlying diseases at the same time, so it is necessary to examine the influence of each disease separately and evaluate its effect on the MSBOS indices in future studies. In the present study, patients with diabetes had the highest C/T ratio (1.9), compared to others. Similarly, in the study by Sandoughdaran et al., 2013, diabetes was one of the main predictive factors for an intraoperative blood transfusion. Other factors included gender, body mass index (BMI), pre-operative hemoglobin, smoking and hypertension. However, their study was focused solely on the CABG (Coronary Artery Bypass Grafting) surgeries.18
According to the study previously conducted at the Poursina Hospital in 2015,11 compared to the present study, the hospital has improved over time. Following the instruction of the MSBOS at this hospital, the cost of hospital and patient costs and the workload imposed on the blood bank staff has been reduced. However, as noted, the amount of blood requested in this hospital was higher than the desired amount, which means that only 38.32% of all requested blood units were transfused. The importance of being attentive to the MSBOS guidelines, reviewing hospital guidelines, inspecting them for compliance and, ultimately, providing more facilities for blood transfusion is paramount.
ConclusionIn summary, the results of this study indicated that the blood transfusion and cross-match request at Poursina Hospital in Rasht is in good condition. Among the factors for its success may be the adequate level of knowledge of all those involved in the process of blood transfusion, including surgeons, surgical assistants, anesthesiologists and blood bank staff, as well as in all the instructions communicated to the hospital regarding blood transfusions. In this study, all the MSBOS indices were at the standard level, although the C/T indices were higher than the standard level in the surgeries for cholecystectomy, leg fracture, forearm fracture, hand fracture and skin graft. Blood requests were also excessive throughout the surgery, compared to the number of cross-matched and injected units, requiring more monitoring of the number of blood unit requests, especially in the listed operations and in compliance with the MSBOS guidelines.
Ethical considerationsIn this study, the required information was extracted from patient files, without mentioning their names in the research to preserve patient privacy. In addition, we received ethical exemption status from the Research Ethics Committee at the Guilan University of Medical Sciences.
Conflicts of interestThe authors declare no conflicts of interest.
We appreciate the support of the Clinical Research Development Unit of Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.



