
In 2001, the Brazilian Ministry of Health added hemoglobinopathies to the National Neonatal Screening Program to be implemented in three steps. In order to meet the proposed goals, it is crucial to establish periodic assessments of this program with the aim of monitoring its implementation.
ObjectiveTo assess the scope and the efficiency of the stages of the National Newborn Screening Program in identifying hemoglobin S.
MethodsA cross-sectional study was developed with the results of the heel prick test using the high performance liquid chromatography method for babies born in Mato Grosso do Sul from 2006 to 2010. The following variables were investigated: year, number of live births, total screening, coverage ratio, prevalence, time between the child birth and the blood collection; age at diagnosis; age at the time of the first consultation; and time between the diagnosis and the first appointment.
ResultsOver the five years of the study, the mean coverage rate was 91.77%. The prevalences of hemoglobin FAS and hemoglobin FS were 1.65% and 0.011%, respectively. Blood samples from 43.48% of children were collected from the second to the seventh day. The age at diagnosis was within the first 28 days in 87.80% of the screened children. The lowest mean indices for the first consultation and the time between the diagnosis and the first appointment (58.8 and 46.4days, respectively) occurred in 2010.
ConclusionsThe scope of the National Neonatal Screening Program for hemoglobinopathies is good, with a large number of individuals being tested. Efficiency is a suitable indicator to assess the program steps. Three points are recommended: the training of the individuals involved, studies to assess the assistance provided to the affected child, and genetic counseling to the mothers.
© 2014 Associação Brasileira de Hematologia, Hemoterapia e Terapia Celular. All rights reserved.
Hemoglobinopathies are recessively inherited genetic diseases, including sickle cell disease and thalassemias.1 The presence of hemoglobin S (Hb S), prevailing in sickle cell disease, consists in a change that characterizes it as a structural hemoglobinopathy, whereas thalassemia is a synthesis hemoglobinopathy. Individuals with Hb S have predominated in the screenings performed in the state of Mato Grosso do Sul (MS).2,3 In order to explain these findings, further research is needed. However, this study corroborates research developed in Dourados, MS, using molecular biology techniques to confirm the diagnosis of some hemoglobinopathies.4
Hb S can be found in the heterozygous state (sickle cell trait), which is considered asymptomatic, that is without disease; in a homozygous state (Hb SS or sickle cell anemia), or in association with other changes (Hb S/β-thalassemia, Hb SC, HB SD and others).5,6 Because of the clinical complexity and high death rate worldwide, these genetic changes, specifically sickle cell anemia, have contributed to the creation of community-based programs.7
In 2001, the Brazilian Ministry of Health, through the Act 822/01, added the hemoglobinopathies to the National Neonatal Screening Program (Programa Nacional de Triagem Neonatal) to be implemented in three steps in 12 Brazilian States.8 Under the responsibility of the Instituto de Pesquisas, Ensino e Diagnóstico da Associação de Pais e Amigos dos Excepcionais (IPED-APAE), the program is in its Step II in the State of Mato Grosso do Sul. Coverage has been increasing in the State; in 2002, the program already screened 92.06% of newborns.2 Since then, there have been no records of coverage of less than 87.41%.2
For the screening program to be able to reach the proposed goals,8 it is essential to establish periodic assessments, and divulge the results to the public health authorities intending to improve the system. The assessment of the scope and the efficiency of the program leads to its monitoring, aiming at better meeting the population’s needs.9 Accordingly, this study aims not only at assessing the comprehensiveness (coverage) of the program, but also at identifying the steps (efficiency) that need to be improved. Thus, the efficiency of the steps of the screening program was chosen as an appraisal indicator. The objective of this work was to assess the scope and the efficiency of the steps of the hemoglobin S screening program in the State of Mato Grosso do Sul, from 2006 to 2010.
MethodsThis is a cross-sectional study of the screening results for hemoglobinopathies of 181,973 children in the 78 municipalities of the State of Mato Grosso do Sul. Information was obtained from 923 registered collection stations of the screening program – IPED-APAE in the period from 2006 to 2010.
The variables studied to assess the scope were: year, number of live births,10 total screening, coverage rate, and prevalence of hemoglobinopathies, with the exception of thalassemia.
The variables studied to analyze the efficiency of the program were: the time between the child’s birth and the exam, the age at diagnosis, the child’s age at the time of the first consultation, and the time between the diagnosis and the first appointment. This study focused on sickle cell diseases as this proved to be the most common hemoglobinopathies.
The date of the first consultation was taken from the records of IPED-APAE. The time between the diagnosis and the first appointment was calculated from the date of the diagnosis, and from the date of the first consultation.
The screening steps at IPED-APAE are performed in accordance with the technical criteria defined in the Manual of Technical Standards and Operational Routines of the screening program.8
The process starts with blood collection for tests on filter paper (Schleicher & Schuell 903), using the heel prick technique in Family Health Clinics, maternity wards or hospitals, by a member of the nursing team or a trained technician.
After collecting and drying the sample, it is placed in an envelope for biological materials and sent to a testing laboratory. Municipalities with ambulances going to Campo Grande (the State capital) ship the samples directly to the screening laboratory for newborn diseases.
In the laboratory, the blood samples are classified in respect to the quality of the blood sample, and the data relating to the age of the child at the time of the collection is recorded. The criteria adopted to discard the blood sample are: unsuitable sample (visual), insufficient blood for all tests, and early sample (obtained within the first 48 hours after birth). Samples discarded due to the above criteria are returned to the place of origin for the collection of another sample. This study included valid samples only.
Hemoglobin screening is performed using the VARIANTnbs High Performance Liquid Chromatography (HPLC) system. This is a qualitative screening that identifies the presence of normal (Hb F and A) and abnormal hemoglobins (Hb S, D, C, and E).
This methodology is recognized as the gold standard by the Brazilian Ministry of Health. The results of the tests are available as web reports sent to the health clinics via the internet, printed, or sent by e-mail.
Newborns with results suggestive of hemoglobinopathies are scheduled for their first consultation with a hematologist at APAE-IPED. Subsequently, a clinical follow-up is carried out during the first year of life, and after this period the children are referred to the Campo Grande Regional Hospital to confirm the diagnosis.
This research was approved by the Research Ethics Committee of the Universidade Federal de Mato Grosso do Sul (protocol #1.822/2010/UFMS). For the statistical analysis, descriptive measures were calculated using the Statistical Analysis Software (SAS) version 9.0 for Windows. The following formula was used to calculate the coverage of the screening program: coverage=number of screened babies / number of live births×100. Prevalence rates were estimated by point and 95% confidence intervals (95% CI).
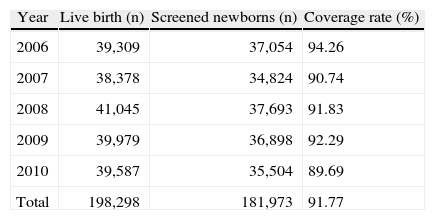
ResultsBased on the number of live births, the coverage rate varied over the five-year period (Table 1); the highest coverage occurred in 2006 (94.26%), and the lowest in 2010 (89.69%).
Overall screenings and coverage rate of newborns investigated at IPED APAE, Mato Grosso do Sul, 2006 to 2010.
| Year | Live birth (n) | Screened newborns (n) | Coverage rate (%) |
| 2006 | 39,309 | 37,054 | 94.26 |
| 2007 | 38,378 | 34,824 | 90.74 |
| 2008 | 41,045 | 37,693 | 91.83 |
| 2009 | 39,979 | 36,898 | 92.29 |
| 2010 | 39,587 | 35,504 | 89.69 |
| Total | 198,298 | 181,973 | 91.77 |
IPED-APAE: Instituto de Pesquisas, Ensino e Diagnósticos da Associação de Pais e Amigos dos Excepcionais.
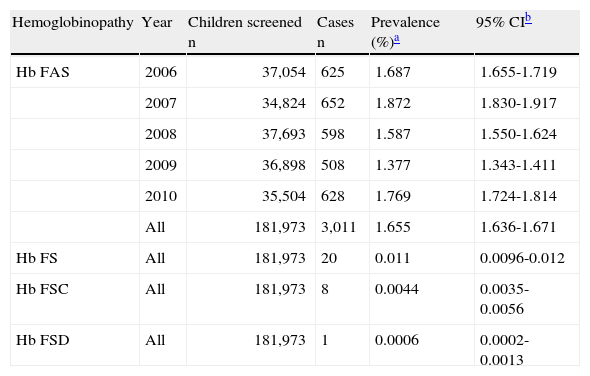
Of the total of 181,973 samples screened by the program, 3,040 were diagnosed with Hb S in different genotypic associations; 20 cases were diagnosed with Hb FS; eight had results for Hb FSC, one for Hb FSD, and 3,011 were Hb FAS, the asymptomatic form of the disease.
When examining the prevalence among 181,973 children screened (Table 2), Hb S was the most frequent hemoglobinopathy, with Hb FAS being the most prevalent in 2007. The prevalence of the homozygous form, sickle cell anemia, was 0.011% with one case in 9,098 children screened.
Prevalence of hemoglobinopathies estimated as percentages of total and 95% confidence interval in children screened at IPED-APAE, Mato Grosso do Sul, 2006 to 2010.
| Hemoglobinopathy | Year | Children screened n | Cases n | Prevalence (%)a | 95% CIb |
| Hb FAS | 2006 | 37,054 | 625 | 1.687 | 1.655-1.719 |
| 2007 | 34,824 | 652 | 1.872 | 1.830-1.917 | |
| 2008 | 37,693 | 598 | 1.587 | 1.550-1.624 | |
| 2009 | 36,898 | 508 | 1.377 | 1.343-1.411 | |
| 2010 | 35,504 | 628 | 1.769 | 1.724-1.814 | |
| All | 181,973 | 3,011 | 1.655 | 1.636-1.671 | |
| Hb FS | All | 181,973 | 20 | 0.011 | 0.0096-0.012 |
| Hb FSC | All | 181,973 | 8 | 0.0044 | 0.0035-0.0056 |
| Hb FSD | All | 181,973 | 1 | 0.0006 | 0.0002-0.0013 |
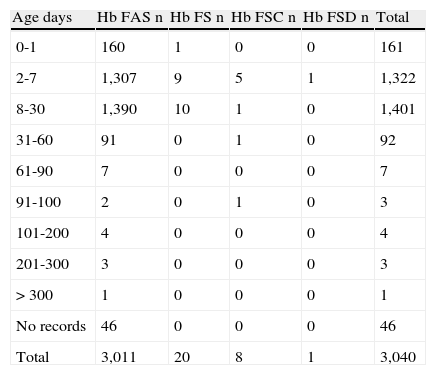
In respect to the time from birth to the blood sampling for neonatal screening, Table 3 shows that, of the children screened with hemoglobin S, 161 (5.3%) underwent the test before 48 hours of life; 1,322 (43.48%), between the second and seventh day, and 1,401 (46.1%), between the eighth and 30th day. A further 46 (1.5%) children presented positive results for Hb FAS, yet there was no record of their age at the time of collection.
Occurrence of cases of sickle cell trait and sickle cell disease according to age in days at time of sample collection for neonatal screening at IPED-APAE, Mato Grosso do Sul, 2006 to 2010.
| Age days | Hb FAS n | Hb FS n | Hb FSC n | Hb FSD n | Total |
| 0-1 | 160 | 1 | 0 | 0 | 161 |
| 2-7 | 1,307 | 9 | 5 | 1 | 1,322 |
| 8-30 | 1,390 | 10 | 1 | 0 | 1,401 |
| 31-60 | 91 | 0 | 1 | 0 | 92 |
| 61-90 | 7 | 0 | 0 | 0 | 7 |
| 91-100 | 2 | 0 | 1 | 0 | 3 |
| 101-200 | 4 | 0 | 0 | 0 | 4 |
| 201-300 | 3 | 0 | 0 | 0 | 3 |
| > 300 | 1 | 0 | 0 | 0 | 1 |
| No records | 46 | 0 | 0 | 0 | 46 |
| Total | 3,011 | 20 | 8 | 1 | 3,040 |
Data related to the occurrence of cases of sickle cell trait and sickle cell disease, according to age in days at the time of diagnosis, indicate that among the children screened, 2,669 were between 0 and 28 days at diagnosis, and 371 were older. Among the newborns, 24 had sickle cell disease genotypes (18 with Hb FS, five with Hb FSC, and one with Hb FSD), and 2,645 had the sickle cell trait genotype (Hb FAS).
Among the children older than 28 days at diagnosis, five cases had the disease (two with Hb FS, and three with Hb FSC), and 366 had Hb FAS.
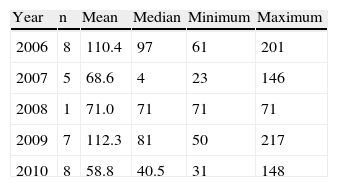
As for the age of children at the time of the first appointment, in 2009, the mean age was 112.3days (n=7; median=81; range: 50-217days), whereas in 2010, there was a decrease in age at the first consultation, with a mean of 58.8days (n=8; median=40.5; range: 31-148days) (Table 4).
Age of the children in days, at time of the first consultation after diagnosis in the neonatal screening program at IPED-APAE, Mato Grosso do Sul, 2006 to 2010.
| Year | n | Mean | Median | Minimum | Maximum |
| 2006 | 8 | 110.4 | 97 | 61 | 201 |
| 2007 | 5 | 68.6 | 4 | 23 | 146 |
| 2008 | 1 | 71.0 | 71 | 71 | 71 |
| 2009 | 7 | 112.3 | 81 | 50 | 217 |
| 2010 | 8 | 58.8 | 40.5 | 31 | 148 |
The highest mean number of days between the diagnosis of sickle cell disease and the first consultation was in 2006 (n=8; mean: 86.8; median=63.5; range: 50-154days). In 2010, the average number of days between the diagnosis and the first appointment was the lowest (n=8; mean: 46.4; median=28; range: 4-135days).
DiscussionThe mean coverage of screening program in this study was 91.77% between 2006 and 2010, with the highest rate in 2006 (94.26%). In a study conducted in the Brazilian Federal District, the coverage rate was 83.4% in 2006,11 and in Bahia State, the average coverage rate was 88.9% in the period from 2007 to 2009.12 The program’s national goal is to achieve a coverage of 100%.8
The differences among the Brazilian regions can be justified by the structure and the organization of services. The uptake of live births, the number of collection stations, the shipment of samples in a suitable timeframe, and the articulation between the steps, are of utmost importance for the program's success. As for the equity of access, the local services should be aware of niche populations, because of the risk of failing to collect samples given the cultural, social, and economic heterogeneity of Mato Grosso do Sul, which borders Bolivia and Paraguay, and has the second largest indigenous population in the country.13
Regarding the prevalence of the hemoglobinopathies, the results show that, of 181,973 children screened, 3,040 (1.67%) presented Hb S in different genotypic associations.
This finding confirms those described in the literature, i.e., in Brazil, Hb S is the commonest hemoglobinopathy, marked by a high prevalence, and potential morbidity.14 These results corroborate the epidemiological survey developed in Mato Grosso do Sul, from 2000 to 2005, in which, among the children screened, 2,624 (1.38%) presented Hb S in different genotypic associations.2
In the present study, the highest prevalence for Hb FAS was 1.87% in 2007. This finding places Mato Grosso do Sul, together with Santa Catarina (0.9%),15 among the Brazilian states with the lowest prevalence of sickle cell disease. These results are different from those of Bahia, which presented one case for every 650 live births screened (n=257); Bahia is the State with the highest prevalence of sickle cell disease.16
Attention should be paid to the results related to the time between the birth and neonatal screening, which revealed early collections in 5.3% of the cases. In Brazil, the Ministry of Health reported that, in 2011; 62.11% of the tests were performed by the seventh day of life, disregarding the results in cases of early collection.17
When analyzing the age in days at the time of collection, it was found that 43.48% occurred from the second to seventh day, as recommended by the screening program.8
Globally, the results of studies in respect to the age at the time of collection are fairly diversified. Research conducted in the Gaza Strip, in the Palestinian Territories, showed that 61% of the collections occurred between the 11th and 17th day of life.18 In Brazil, in Porto Alegre city, the average was 11 days;19 in Sergipe State 17 days, with 50% of samples being collected in children older than 28 days;20 in Campina Grande city, the average was 29.8days,21 and in Marília, São Paulo State, the average was 27 days.22
A weak point in this study lies in the absence of a record of the age at the time of collection for 46 children positive for Hb FAS.
Concerning the age in days at diagnosis, 87.80% of the results were ready while the subjects were neonates (up to 28 days). In discussing this figure, it was observed that early diagnosis favors interventions and, therefore, positively influences the outcome of the disease.23
In recent years, the expectations related to morbidity and mortality from sickle cell disease have changed dramatically, partly due to the higher accuracy of tests, early diagnosis, and greater knowledge about the disease. Another reason is the increased sensitivity of the public health institutions in Brazil, motivated by social movements focused on the black population, and by the societies of Hb S gene carriers.5
Regarding the age of the child at the first consultation, and the time between the diagnosis and the first appointment, 2010 had the lowest indices among the years studied, which led to a shorter time to diagnosis. According to the literature, the earlier the diagnosis and treatment of sickle cell disease, the less likely patients will have complications, thereby increasing the survival and the quality of life.24
Routine preventive measures for patients with sickle cell disease should be initiated within the first two months of life, as at the first consultation; parents and guardians should be counseled about prophylaxis against infections, immunizations, and also taught to identify the complications of the disease, reducing morbidity and mortality.25
The screening program defines the intervals between the steps, so as to provide the patient with early diagnosis and timely treatment. Therefore, the gap between the birth and the initiation of the treatment should be short, so that the program can be effective in preventing sequels, in promoting social inclusion, and in reducing suffering.23
ConclusionThe scope of the screening program for hemoglobinopathies in the state of Mato Grosso do Sul is successful, with a mean coverage of 91.77%, thereby providing diagnoses of Hb S for the population. Efficiency, the indicator employed in this study, identified two steps that need to be improved: the time of the sample collection, which in many cases is too early, and age at diagnosis of more than 28 days. Thus, the authors of this study would like to make three recommendations: continuous training of those involved, further studies to assess the assistance provided to affected children, and the provision of genetic counseling to mothers.
Conflicts of interestThe authors declare no conflicts of interest.
The authors wish to thank IPED-APAE, Campo Grande, MS for making data regarding newborn screening of the municipalities of Mato Grosso do Sul availability, and Fundação de Apoio ao Desenvolvimento do Ensino, Ciência e Tecnologia do Estado de Mato Grosso do Sul (FUNDECT) for the research grant.

