
The aim of this study was to analyze the reticulocyte maturity indices (low, medium, and high fluorescence ratios) in iron deficient 1- to 6-year-old children, and identify the prevalence of iron deficiency anemia in this population.
MethodsThe present study included 39 subjects, divided into two groups: control subjects (n=33), and subjects with iron deficiency anemia (n=6). The results were analyzed by Student’s t-test for comparison of means. Differences were considered significant when two-tailed p-value<0.05.
ResultsSubjects with iron deficiency anemia presented increases in the proportion of mean (10.3±4.7% us. 6.0±3.4%; p-value=0.003), and high fluorescence reticulocytes (2.3±0.87% vs. 0.9±0.9%; p-value=0.03) compared to the control group. The prevalence of anemia in this population was 15% (n=6).
ConclusionThe indices related to immaturity of reticulocytes are higher in the presence of iron deficiency, thus demonstrating a deficiency in the raw material to form hemoglobin and are, therefore, possible early markers of iron deficiency and anemia. We emphasize the need to standardize these indices for use in clinical practice and lab test results.
© 2014 Associação Brasileira de Hematologia, Hemoterapia e Terapia Celular. Published by Elsevier Editora Ltda. All rights reserved.
Iron deficiency, despite its high prevalence, and although its etiology is well known, is a problem that persists in both developed and underdeveloped countries, mainly affecting infants, preschool children, adolescents, and pregnant women.1
Anemia can be defined as a condition in which the hemoglobin (Hb) levels are lower than normal, with these levels varying depending on age and gender. According to the World Health Organization (WHO), normal Hb for children aged 6 months to 4 years is≥11g/dL.2
Considering these factors, new studies are being developed to provide new laboratory parameters to allow early detection and assessment of iron deficiency, as well as to identify highrisk population groups. From a public health perspective, an intervention is warranted.3
An important index in the diagnosis, classification, and monitoring of anemic patients is the peripheral blood reticulocyte count, which is a primary hematological test used to evaluate the bone marrow response to treatment for anemia.4
Reticulocytes are non-nucleated immature red blood cells in peripheral blood, containing residual RNA.5 The manual method for reticulocyte counts is the most commonly used in clinical laboratories, and is based on microscopic observation of residual ribosomal RNA, easily recognized by supravital staining.6
In recent years, automated reticulocyte analysis by flow cytometry has been incorporated into the laboratory routine as an alternative to the manual method. It is rapid, more accurate, and easy to perform, and provides both the number of reticulocytes and several indices that can be helpful in the diagnosis of pathologies, and in monitoring bone marrow recovery. These indices, which require standardization and definition of reference values, are yet to be used in the clinical practice.7
With this automated method, reticulocytes can be classified into three groups according to their fluorescence intensity, which reflects maturity: low fluorescence ratio (LFR), medium fluorescence ratio (MFR), and high fluorescence ratio (HFR).8 Therefore, intracellular RNA levels are directly related to fluorescence intensity, and, consequently, to the degree of maturation of reticulocytes.9
This study aimed to analyze the reticulocyte maturity indices (LFR, MFR, HFR) in iron deficiency in 1- to 6-yearold children, in order to determine their applicability in iron deficiency anemia, and to identify the prevalence of this condition in these children.
MethodsThe sample consisted of thirty-nine children, aged from 1 to 6 years, enrolled in a kindergarten (Casa da Criança Santo Antônio) in the city of Cachoeira do Sul, Rio Grande do Sul, Brazil, from August 2009 to July 2010.
Inclusion criteria were: children with ages above one year and under six years who were not under treatment with iron or vitamins. These items were verified by a questionnaire applied to the parents or legal guardians, who signed an informed consent form after the procedures of the study had been explained. Five children were excluded due to difficulties in respect to venipuncture.
This study was approved by the Human and Animal Research Ethics Committee of the Universidade Luterana do Brasil - ULBRA (Canoas, Brazil).
Blood samples from children were obtained using tubes containing ethylenediaminetetraacetic acid (EDTA) anticoagulant, and in tubes not containing EDTA.
The hematology analysis of the samples was performed using a Sysmex KX-21N™ automated hematology analyzer. Reticulocyte counts were generated by Sysmex XT 2000.
Biochemical testing to confirm the iron status was carried out using an automated Dimensseq (ferrozine). Ferritin was measured using a chemiluminescence immunoassay (Elecsys 1010).
The sample was divided in two groups, the control group (non-anemic - Hb>11.0g/dL) and anemic (Hb<11.0g/dL). The control group consisted of individuals paired by age and gender with iron deficiency anemia, who were selected by laboratory studies. Data are reported as means and standard deviation (SD).
For the statistical analysis, the results were analyzed by Student's t-test for comparison of means. Differences were considered significant when the two-tailed p-value was<0.05. Data were submitted to statistical analysis using the Statistics Package for the Social Sciences (SPSS). The criteria used to define individuals with iron deficiency anemia (n=6) were lower than normal Hb (< 11g/dL) and iron level (< 13mmol/L).
Reticulocyte indices can be classified into three groups, according to the fluorescence intensity that reflects the maturity of reticulocytes (LFR: normal values between 81.0% and 96.4 %; MFR: between 1.1% and 15.2 %; HFR: between 0.03% and 3.95% of the total reticulocytes).8·10
ResultsThe study population consisted of 39 children, 21 male (53.8%) and 18 female (46.2%), with a mean age of 3.7years, enrolled in a kindergarten. All laboratory results were within the values considered normal for this age group.
The sample was divided into two groups: control group (non-anemic - n=33) and group with iron deficiency anemia (anemic - n=6). The demographic and clinical characteristics of the two groups are shown in Table 1.
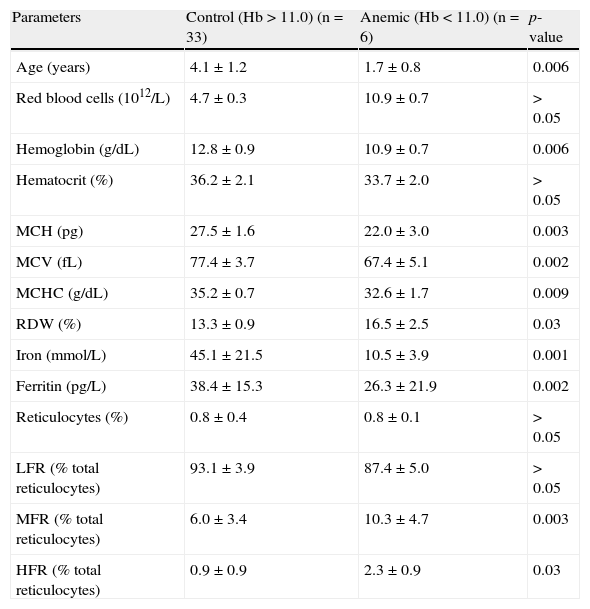
Demographic and clinical characteristics (mean±SD) compared between the control group and the group with iron deficiency anemia.
| Parameters | Control (Hb>11.0) (n=33) | Anemic (Hb<11.0) (n=6) | p-value |
| Age (years) | 4.1±1.2 | 1.7±0.8 | 0.006 |
| Red blood cells (1012/L) | 4.7±0.3 | 10.9±0.7 | > 0.05 |
| Hemoglobin (g/dL) | 12.8±0.9 | 10.9±0.7 | 0.006 |
| Hematocrit (%) | 36.2±2.1 | 33.7±2.0 | > 0.05 |
| MCH (pg) | 27.5±1.6 | 22.0±3.0 | 0.003 |
| MCV (fL) | 77.4±3.7 | 67.4±5.1 | 0.002 |
| MCHC (g/dL) | 35.2±0.7 | 32.6±1.7 | 0.009 |
| RDW (%) | 13.3±0.9 | 16.5±2.5 | 0.03 |
| Iron (mmol/L) | 45.1±21.5 | 10.5±3.9 | 0.001 |
| Ferritin (pg/L) | 38.4±15.3 | 26.3±21.9 | 0.002 |
| Reticulocytes (%) | 0.8±0.4 | 0.8±0.1 | > 0.05 |
| LFR (% total reticulocytes) | 93.1±3.9 | 87.4±5.0 | > 0.05 |
| MFR (% total reticulocytes) | 6.0±3.4 | 10.3±4.7 | 0.003 |
| HFR (% total reticulocytes) | 0.9±0.9 | 2.3±0.9 | 0.03 |
MCH: mean corpuscular hemoglobin; MCV: mean corpuscular volume; MCHC: mean corpuscular hemoglobin concentration; RDW: red cell distribution width; LFR: low fluorescence ratio; MFR: medium fluorescence ratio; HFR: high fluorescence ratio.
There was a statistically significant difference in age between the groups. The group of patients with iron deficiency anemia had a statistically significant decrease in the amount of Hb, mean corpuscular volume (MCV), red cell distribution width (RDW), mean corpuscular hemoglobin concentration (MCHC), iron, and ferritin. No statistically significant difference was found in the reticulocyte counts. Regarding the reticulocyte indices, statistically significant differences were observed for MFR and HFR between the groups. The prevalence of anemia in this population was 15% (n=6).
DiscussionOne of the objectives of the present study was to analyze the reticulocyte maturity indices (LFR, MFR, HFR) in individuals with iron deficiency. These indices show the immaturity of reticulocytes and the bone marrow activity through fluorescence intensity.11
The reticulocyte count is one of the most common hematological tests to classify and monitor the treatment of different types of anemia, as well as to determine if the bone marrow is functional.7
An increase of immature reticulocytes in the blood of individuals with iron deficiency anemia represents a response to anemia, as long as the medullary tissue and the indispensable factors for erythropoiesis are preserved.
Anemic hypoxia stimulates the release of erythropoietin in the bone marrow, increasing cell proliferation and differentiation. If the reticulocyte concentration increases in the medulla, its maturation will be completed in the blood.8,11 In order to determine a possible relationship between the reticulocyte indices (LFR, MFR, HFR) and iron deficiency anemia, the study sample was divided into two groups. The MFR and HFR were significantly different between the groups.
The reticulocyte indices analyzed in the study are related to the amount of RNA contained in reticulocytes and, consequently, to their degree of immaturity. Despite the small sample of individuals with iron deficiency anemia, the results showed significantly higher values of MFR and HFR in individuals with iron deficiency compared to controls.12
In more severe anemia, the maturation time of reticulocytes in the medulla decreases, and an increased number of immature reticulocytes are released into the peripheral blood. These reticulocytes will remain more than 48 hours in the peripheral blood until they turn into red blood cells. Therefore, the immature reticulocyte count in the peripheral blood will be higher.4,9 Hence, we believe that the indices related to the immaturity of reticulocytes increase in the presence of iron deficiency, thus demonstrating a deficiency of the raw material for the formation of Hb. These results are consistent with other studies since they also presented elevations of MFR and HFR in iron deficiency anemia,7,9–11 but unlike others which showed no increase of these indices.12–14
Considering that the average lifespan of a red blood cell is about four months, and the daily renewal of erythrocyte mass corresponds to 1% of circulating red blood cells, abnormalities in the hematimetric indices of anemic individuals can take weeks to be detected. Thus, the reticulocyte indices may serve as early markers of iron deficiency and anemia.8,9
However, some studies have presented difficulties and limitations in the use of reticulocyte indices in the laboratory practice, either by the definition of their own indices, or the issue of standardizing and correlating indices among the different methods of detection employed using automated equipment.13,15,16
The prevalence of iron deficiency anemia in this study was 15% (n=6); this is a low figure compared to other studies carried out with the same age group,1,17 which found a prevalence of 63.2% and 47.8%. However, other studies have reported 11% of iron deficiency anemia, similar to the rate observed in this study.17,18 We believe that the small sample size analyzed in this study may have contributed to this low prevalence.
A limitation of the current study was the small sample size, which may have induced bias in the results.
ConclusionThe results suggest that the MFR and HFR are high in iron deficiency, suggesting increased erythropoietic activity in anemic individuals, which may potentially be used as early diagnostic markers for iron deficiency and anemia.
Conflicts of interestThe authors declare no conflicts of interest.

