



Graft-versus-host disease is one of the main causes of morbidity and mortality in patients submitted to hematopoietic stem cell transplantation. This study reviewed the prevalence of lower female genital tract graft-versus-host disease following hematopoietic stem cell transplantation. A systematic search of the literature for articles published between 1982 and 2015 was performed. A growing number of young women suffering from malignant and benign hematological diseases are receiving allogeneic hematopoietic stem cell transplantation with very satisfactory results in relation to the disease itself. However, these patients face gynecological problems due to graft-versus-host disease. Correct diagnosis and early management are needed to avoid irreversible complications.
Hematopoietic stem cell transplantation (HSCT) is indicated for the treatment of malignant and benign hematological diseases as well as other non-hematological disorders, such as autoimmune diseases.1,2 Graft-versus-host disease (GVHD) occurs in 30–70% of the cases and frequently reduces the quality of life of transplant patients.1,3–5 GVHD is triggered by a complex immune response mediated by T-cells, in which the donated marrow does not recognize the host organism (recipient) and proceeds to destroy the tissues.5
Historically, the definition of acute GVHD was defined temporally, i.e., it manifested within one hundred days after transplantation.2 Currently, this concept is being reviewed and can be based on clinical characteristics.3 The acute presentation may manifest as cutaneous involvement with a maculopapular rash, erythroderma and blister formation, hepatic canalicular dysfunction, oral mucositis and upper and lower gastrointestinal tract dysfunction with nausea, vomiting, and diarrhea. It can be classified as being of classic, persistent, recurrent or late presentation.2
The biology of GVHD is complex because it is a process that occurs in several phases and involves the activation of donor T-cells. GVHD occurs when donor T-cells react against receptor proteins, the most important being those belonging to the human leukocyte antigens (HLA) system encoded by the major histocompatibility complex (MHC). HLA class I (A, B and C) has proteins expressed in almost all nucleated cells in the human body. HLA class II proteins (DRB1, DQB1 and DP) are generally expressed in hematopoietic cells, such as B cells, dendritic cells, and monocytes.5 The frequency of acute GVHD is directly related to the degree of incompatibility between donor and recipient HLA proteins.2
The acute form of GVHD is mediated by the activation and expansion of alloreactive lymphocytes derived from the donor (graft), host dendritic cells, and partly from donor dendritic cells by cross-presentation of alloantigens. This whole process leads to an imbalance in the production of inflammatory cytokines (tumor necrosis factor-alpha, interleukin-1β, and interleukin-6) and a reduction in the number of regulatory T-cells (Treg), that is, graft T-cells trigger a response that results in tissue damage of the host. 2,4,5
There is evidence that the pathogenesis of chronic GVHD is similar to autoimmunity processes.4,5 This form of the disease is often represented by a syndrome involving components of the cellular (innate and adaptive) and humoral immune responses, abnormal immune regulation and fibrosis. Clinical features are similar to those of autoimmune diseases, including scleroderma, Sjögren's syndrome, lichen planus, primary biliary cirrhosis, bronchiolitis obliterans, immune cytopenia, and chronic immunodeficiency.6,7 The organs or sites most commonly affected by GVHD are the skin, eyes, mouth, lungs, liver, intestine and genitals with manifestations typically appearing within the first year after HSCT, usually when immunosuppression is withdrawn.6–8 Commonly, symptoms start between two months and six years after HSCT. In approximately 10% of patients, however, symptoms start after one year.9
Genital GVHD is a common and underreported complication, affecting around 25% of all females submitted to HSCT;10 the vulva and vagina may be affected. The main signs and symptoms are sensitivity to palpation of the openings of the vestibular glands or vulvar mucosa, erosion of the mucosa, fissures, leukokeratosis, labial or clitoral fusion, fibrous vaginal ring, vaginal shortening, vaginal adhesions and complete vaginal stenosis. Other symptoms include dryness, burning, pruritus, pain on touch, dysuria, dyspareunia and consequent sexual dysfunction.11,12 The mean time to onset of genital GVHD is 7–10 months after HSCT, so genital GVHD is commonly a chronic manifestation.13 Preventive gynecological care, as well as early detection and treatment, are essential to reduce morbidity in these women.14
The pre-transplant clinical evaluation of women include recommendations about vulvovaginal GVHD, including early manifestations and complications and the importance of regular gynecological check-ups to help prevent severe gynecological complications, which often can become irreversible and have a significant negative impact on the quality of life.15 Most clinicians and gynecologists may not recognize gynecological complications occurring after HSCT. This is a concern in view of a growing long-term post-transplant women population who have been cured of their disease but can still suffer from severe gynecological complications. Therefore, an updated review of the scientific knowledge on relevant aspects of gynecological complications after HSCT is needed.
This narrative review of the literature about gynecological complications, in particular genital GVHD, after HSCT investigates the prevalence, pathogenic mechanisms involved, clinical manifestations and treatment management, in addition to the 2014 National Institutes of Health (NIH) chronic GVHD consensus guidelines.3 General recommendations for the care of these females in pre- and post-HSCT periods were also evaluated from the literature and our experience.
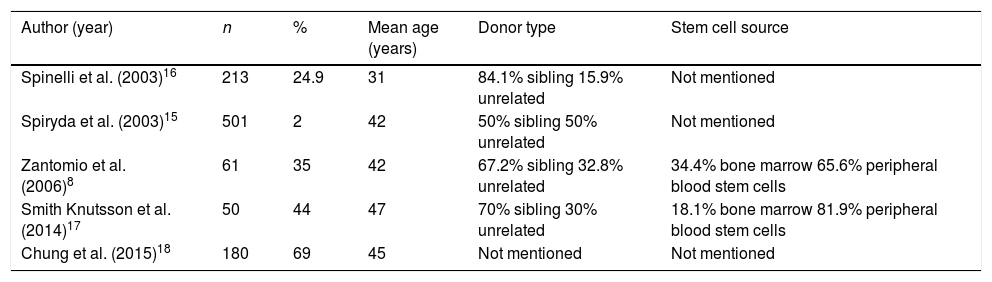
Prevalence, involvement and risk factors for gynecological graft-versus-host diseaseThe prevalence of genital GVHD varied in the published studies with rates ranging from 24.9% to 69% (Table 1).8,13,16–18 However, it is likely that this prevalence is underestimated because only patients who reported symptoms were included and there might be underreporting.17 A prospective surveillance program involving 61 patients reported a prevalence of 35% at one year and 49% at two years of follow-up (8). Spinelli et al.16 reported a prevalence of 25%. Smith Knutsson et al.17 reported 50 patients assessed over nine years with a genital prevalence of GVHD of 44%, while Chung et al.,18 evaluating 180 patients over four years, found 69% of genital GVHD. A long-term randomized study reported a higher prevalence of genital GVHD in recipients of mobilized peripheral blood transplants compared to bone marrow transplants.19 Variation of reported prevalence of genital GVHD depends on several factors, including, systematic, time-dependent gynecological evaluations regardless of symptoms and the diagnostic criteria used (symptoms only, examination findings with symptoms or without symptoms, etc.).14,17
Prevalence of female genital tract graft-versus-host disease.
| Author (year) | n | % | Mean age (years) | Donor type | Stem cell source |
|---|---|---|---|---|---|
| Spinelli et al. (2003)16 | 213 | 24.9 | 31 | 84.1% sibling 15.9% unrelated | Not mentioned |
| Spiryda et al. (2003)15 | 501 | 2 | 42 | 50% sibling 50% unrelated | Not mentioned |
| Zantomio et al. (2006)8 | 61 | 35 | 42 | 67.2% sibling 32.8% unrelated | 34.4% bone marrow 65.6% peripheral blood stem cells |
| Smith Knutsson et al. (2014)17 | 50 | 44 | 47 | 70% sibling 30% unrelated | 18.1% bone marrow 81.9% peripheral blood stem cells |
| Chung et al. (2015)18 | 180 | 69 | 45 | Not mentioned | Not mentioned |
Better strategies for care and support of post-transplant complications may explain the increase in the identification of genital GVHD over the years.14 The average time to the onset of gynecological manifestations is 7–10 months after transplantation,16 but late onset, after one year, is not uncommon.8,11
In fact, the exact time of onset is often not clear and both doctors and patients, especially asymptomatic women and those who are sexually inactive, may delay in detecting clinical symptoms.14 Genital GVHD findings in the gynecological examination may be the initial manifestation of GVHD in up to 27% of the cases.16
The main risk factor for the development of chronic genital GVHD is the use of peripheral blood as the source of the progenitor cells for the transplant, representing a risk three times higher than that obtained from bone marrow cells.8,19,20 The type of conditioning, type of donor, parity, age, and presence of vaginal infection at the time of transplantation do not appear to have an impact on the prevalence of genital GVHD.8,16
Clinical manifestations of female genital graft-versus-host diseaseOften, genital GVHD is associated with GVHD manifestations in other organs, especially the skin, oral mucosa, eyes and gastrointestinal tract and can even appear long after the initial manifestation of GVHD.21–23 In 68% of cases, the symptoms affect the vulva only, while in 26% both the vulva and the vagina are affected, with vulvar lesions usually preceding the vaginal lesions. The time lag between the start of vulvar and vaginal symptoms offers an opportunity to start prophylactic measures, to prevent the occurrence of more severe complications, such as vaginal stenosis, with consequent impairment of sexual function.13,14
The genital symptoms may include dysuria, the sensation of dryness and burning in the vulva, a sensitivity of the vulva and vaginal introitus to touch or when washing, vaginal bleeding after intercourse and dyspareunia.12,16,24,25
Vaginal secretion is mentioned by 25% of patients with vaginal involvement, especially in the early stages, but in its mild form, it may be asymptomatic and detected only in the gynecological examination.26
The most common complaints are vulvar dryness (80%)15 and dyspareunia, affecting sexual activity (50%).24 Penetration dyspareunia is often and easily distinguished from deep dyspareunia. Introital pain results from inflammation of the openings of the vestibular glands (Bartholin's and Skene's glands), erosions or vulvar fissures, and less frequently, from labial fusion. Deep dyspareunia occurs in patients with synechiae or vaginal shortening. Amenorrhea and cyclical pelvic pain due to hematocolpos are considered severe symptoms.17,27,28
Stratton et al.11 analyzed 33 females submitted to HSCT and reported that 29 (88%) had vulvar or vaginal symptoms compatible with GVHD, with the onset of manifestations around 267 days after transplantation. The authors also reported the presence of dyspareunia in 21 (63.6%) women, vulvar erythema in 27 (93.1%), vulvar fissures or erosions in 15 (51.2%), fusion of the clitoris in three (10.3%), vaginal synechiae in five (17.2%), and total obstruction of the vagina in one (3.4%) patient.
The findings at physical examination resemble the symptoms of erosive lichen planus and include adhesions of the labia minora, introitus and vaginal canal, and loss of vulvar architecture caused by fusion of the labia minora and the clitoris prepuce that can result in burying of the clitoris (Figure 1) and narrowing of the introitus.28–30

Vaginal synechiae, decreased elasticity and shortening of the vaginal canal make it difficult or impossible to view the cervix entirely for the collection of a Pap smear and withdrawal bleeding, in cases of cyclic hormone replacement. These symptoms also make sexual intercourse difficult or impossible.31–34
In 1982, Corson et al.12 reported the first five cases of women with sclerosing vaginitis and the formation of stenosis. Since then, several cases have been reported with complete vaginal obliteration.31–33 However, it is believed that the majority of cases involve mild GVHD of the vulva or vagina, which may be asymptomatic and detected only by clinical examination.19 For this reason, it is advised that even asymptomatic patients be routinely examined, to prevent the development of more severe conditions.35
Vulvodynia is a chronic pain syndrome in which the patient feels pain on palpation of the openings of the vestibular glands (Skene's and Bartholin's glands), labia majora and minora, and different degrees of vestibular erythema, similar to that found in gynecological GVHD. The history of symptoms prior to transplantation helps to distinguish between differential diagnoses.36
Diagnosis and staging of female genital graft-versus-host diseaseThe NIH developed a project to obtain a consensus on the criteria to be used in clinical studies of chronic GVHD. These criteria have enabled standardization of the clinical evaluations to be used in the diagnosis while providing a means of scoring the organs involved and overall assessment of severity. They also enable a better analysis of the prevalence of GVHD and help in the evaluation of the severity of impairment of organ or site, whether alone or combined, and its influence on late transplant-related mortality.3,35
Several prospective and retrospective studies have validated many aspects of this consensus for the diagnosis of GVHD,35 however, in specific organs and sites, the minimum criteria for diagnosing chronic GVHD were not clearly defined. Therefore, a new consensus was created in 2014 based on the available evidence, in which the diagnostic criteria for genital GVHD were modified.3
The overall assessment of the severity of GVHD is usually based on the number of components or sites involved and the degree of involvement of each component affected. The recommendations for diagnosis, according to the NIH 2014 guidelines,3 include scoring based on the severity of signs and not on symptoms, as proposed by the NIH in 2005.35 For this reason, it is crucial that a specialist (a gynecologist or other professional with experience in the field) examine the patient, and be able to score female genital GVHD correctly. If a gynecologist is not available, the evaluation of external genitalia can be performed, at least to determine if there is “discomfort in the exam”.
The examination begins with a careful inspection of the vulva, perineum and perianal region to check for signs of vulvar GVHD, and gentle palpation of the openings of the vestibular glands (Skene's and Bartholin's glands), labia minora and majora, with cotton-tipped applicators. The vaginal examination begins with a single-digit exam to determine the possible presence of vaginal synechiae, followed by a specular examination to evaluate the vaginal walls, cervix, and vaginal content, as well as the collection of material for an investigation of fungus, herpes simplex virus and other pathogens, as indicated. Cervical cytology should be obtained annually. If the woman is sexually active, it is important to determine whether gentle palpation causes pain similar to that experienced during sexual intercourse. A photographic record of the lesions is good practice whenever possible.3
The scores range from 0 to 3, with a score of 0 being attributed to patients without signs, 1 for mild signs with or without discomfort in the exam, 2 for moderate signs and symptoms with some discomfort in the physical exam, and 3 for those with severe signs with or without symptoms.3
In accordance with the clinical score, genital involvement is classified as mild, moderate or severe:3
- 1.
Mild (any of the following): erythema on the mucosal vulvar surfaces, vulvar lichen planus or lichen planus sclerosus (Figure 2).
- 2.
Moderate (any of the following): inflammatory changes of erosive vulvar mucous, fissures of the vulvar folds.
- 3.
Severe (any of the following): a fusion of the labia majora and labia minora, clitoral fusion, vaginal adhesions, circumferential fibrous vaginal ring, vaginal shortening, synechiae, dense sclerotic changes and complete vaginal stenosis.

GVHD classification systems were previously proposed with a score for severity by Spinelli et al.,16 Stratton et al.11 and Zantomio et al.8 There are some differences between these classifications but they are all based on symptoms. In 2003, Spinelli et al.16 reported that 25% of 213 transplanted women developed genital GVHD. Using their own classification, 66%, 22%, and 12% of these women had mild, moderate and severe genital GVHD, respectively.
Female genital GVHD with characteristics similar to lichen planus or lichen sclerosus and vaginal synechiae or stenosis are the most common diagnostic signs that do not require a biopsy. However, erosions, fissures and sores are distinctive signs that require the exclusion of possible infection, drug effects, malignancy and other causes.3
A biopsy may also be required for diagnosis in these cases if GVHD is not confirmed in another organ.3 Shulman et al.21 recommend biopsies in cases of suspected GVHD to avoid misdiagnosis, but recognize that the histopathological exam has its limitations. For Lara et al.,26 genital biopsy is important in the differential diagnosis between GVHD and symptoms secondary to hypoestrogenism.
It is emphasized that the histological findings of female genital GVHD are consistent with those of cutaneous GVHD and of the other mucous membranes. These findings include signs of chronic and acute inflammation, the presence of cells undergoing apoptosis in the basal layer, detachment of the epithelial lining of the mucosa, hyalinization and thickening of the collagen fibers, capillary ectasia and mononuclear inflammatory infiltration of the submucosa.26
Treatment of genital graft-versus-host diseaseThe treatment goals for chronic GVHD include relief of symptoms, control of the disease and prevention of damage and disability.35 As a rule, the intensity of treatment should vary according to the extent and severity of the manifestations of the disease. Patients with mild or asymptomatic symptoms and those with the disease limited to a single organ or site can often be controlled periodically or with topical treatment without the need for prophylactic immunosuppressive treatment. Patients with more severe manifestations or the involvement of multiple organs require systemic treatment.34
Preventive measuresHormonal therapy instituted early on, whether systemic or topical, correcting the ovarian failure caused by the use of medicines in the conditioning phase, maintains the physiological characteristics of the genital tract, facilitating early detection of symptoms of GVHD and control of contraception and menorrhagia.7 The use of topical estriol as a 1mg cream or 1mg suppositories on alternate days mitigates atrophy of the vaginal epithelium caused by ovarian failure and accentuated by the action of corticosteroids, and maintains lubrication and vaginal elasticity, allowing sexual activity. Its use should be associated to whichever regimen is chosen.26,37
Support measures, such as the use of emollients and topical moisturizers, sitting in a lukewarm bath and the application of viscous xylocaine can ease the discomfort, particularly in the early stages. It is important to encourage a return to sexual activities, when possible after normalization of platelets with the use of lubricated condoms, to prevent the formation of vaginal synechiae and early onset of vaginal GVHD.13,38
Blocking of menstrual flow to prevent bleeding in the conditioning phase should use combined continuous oral contraceptive and maintained until the normalization of platelets. Synchronization of conditioning for the post-menstrual phase should be performed, whenever possible.7
Early phase treatmentVulvar and introital lesions are the first identified lesions commonly seen in the form of erosions.15 Potent topical steroids in the form of ointment or cream, which have better absorption and emollient action, are the most indicated in this place. Clobetasol propionate 0.05% can be applied directly to the lesions twice daily, until the disappearance of the lesions, followed by gradual reduction of the dose until complete suspension. A compress, or bathing in lukewarm water before the application of corticosteroids facilitates their absorption.26
Damage to the vaginal mucosa may include the formation of ulcers and loose synechiae, and vaginal secretion. The use of hydrocortisone (25mg suppositories) or suppositories with 1mg of estriol twice daily is recommended, decreasing the dose once the symptoms have been controlled, then maintaining twice-weekly administrations and gradually reducing the dose until complete suspension.30 An alternative to suppositories is the application of corticosteroid (hydrocortisone 25mg) with a penile prosthesis to prevent the formation of synechiae.27,30
In a series of 11 patients, Spiryda et al.15 described the use of vaginal cream consisting of a 200mg oral suspension of cyclosporine diluted in an oily base twice daily for four weeks followed by weaning for two months. They observed healing of vaginal erosions after two weeks with its concomitant use with vaginal dilators thereby avoiding the need of surgery to correct stenosis in four of the 11 women studied. The seven women who underwent surgery to correct synechiae and vaginal stenosis continued to use the medicine after surgery and in 6–12 weeks, they were able to have sexual intercourse. Only one patient showed no improvement with clinical or surgical treatment, due to thick synechiae. Finally, local treatment associating corticosteroid and estrogen appeared to decrease the progression from mild to severe lesions, preventing surgical treatment.24
Treatment of late complicationsLate complications, such as adhesions and occlusions in various segments of the genital tract, can be treated surgically with subsequent use of steroids and topical estrogen therapy. Procedures such as dilation and drainage or hysterectomy may be necessary in extreme cases of obliteration with the formation of collections in the cervical canal and uterine cavity (hematometra).28,31–33 However, in the study of Spinelli et al.,16 63% of patients required surgery for vaginal GVHD, despite aggressive vulvar treatment.
Given that topical and (particularly) systemic use of immunosuppressive drugs increases the risk of the manifestation of human papillomavirus (HPV)-induced lesions, post-transplant women should have frequent screening for cervical cancer and its precursor lesions and warts should be surgically excised or cauterized with the application of trichloroacetic acid or laser therapy.16
Furthermore, the development of solid tumors is a long-term complication of HSCT. A large European multicenter study evaluating patients who underwent HSCT over a 15-year period showed that the risk of a second neoplasm was 11.5±2.3% with late mortality attributed to secondary cancer in 7%. 39 In a study by Savani et al.,39 more than 40% of patients who underwent HSCT had abnormal cervical cytology with 20% having high-grade epithelial lesions. Abnormal cytology was detected at around 51 months after the transplant. Some studies suggest that changes in T-cell immunity against HPV or the loss of antibody titers together with the use of immunosuppression for the treatment of GVHD can all contribute to reactivation of HPV leading to the development of dysplasia and squamous cell carcinoma of the female genital tract. 37,40,41 Therefore, recurrent anal or genital warts and cytological abnormalities probably represent reactivation of previous HPV infection rather than a new infection. Furthermore, the clinical manifestation of HPV in these patients may be more common, and progress more rapidly as observed in other immunodepressed patients.42
Given the importance of HPV infection in the pathogenesis of cervical cancer, vaccination against HPV may be offered to young women after the transplant.39,41,42 It is worth considering that the HPV vaccine has been effective in reducing the prevalence of anal and genital warts and cervical intraepithelial neoplasias, and is currently recommended for girls and women aged 9–26 years, but it is not a routine in females outside this age range.43
Guidelines for vaccination against preventable infections after HSCT were published, although antibody responses may be partial. The majority of centers start immunizations in these patients approximately 6–12 months after the transplant. Thus, vaccination one year after transplantation, in theory, could prevent the reactivation of the disease by HPV, if an antibody response is generated.44
ConclusionsA growing number of young women suffering from hematological diseases, both malignant and non-malignant, are receiving allogeneic HSCT with very satisfactory results concerning the disease itself.
However, the full extent of the gynecological problems faced by these patients is becoming increasingly apparent. The real-life application of patient care and genital GVHD monitoring is challenging for transplant centers that do not have a dedicated gynecologist–obstetrician specialized in GVHD. Therefore, it would be ideal for all transplant centers to have a gynecologist capable of monitoring patients in the post-transplantation period. This professional should introduce preventive actions and be alert to recognize genital GVHD lesions early in order to avoid irreversible complications as well as other complications such as HPV recurrence, tumor development, and sexual dysfunction.
More studies are needed to assess this population, given the complexities involved. In this context, it is crucial that the gynecologist–obstetrician and the hematologist–oncologist work together to achieve better results for patients.
Financial supportNone.
Conflicts of interestThe author declares no conflicts of interest.
The authors wish to thank Mary Flowers, director of the Adult Clinical Care Long-Term Follow-Up Program (LTFU) at Hutchinson Center and Seattle Cancer Care Alliance (SCCA) and professor of Medicine in the University of Washington, Seattle, for reviewing the manuscript and offering valuable suggestions. The authors also thank Amaral Carvalho Hospital Outpatient Service (Jaú, SP, Brazil) for kindly providing the pictures for this article. Patients provided consent for the publication of photos for didactic purposes.


