


Dendritic cell (DC) vaccines have demonstrated good efficacy in preventing relapse and in increasing survival of patients affected by a variety of both solid and hematological tumors. Most protocols used to generate these cells involve the automated separation of peripheral blood monocytes from patients. This approach requires specialized equipment, which elevates the cost of this type of therapy, potentially limiting the widespread access to patients. Method: In this study, we compare the yield and quality of dendritic cells generated from monocytes and isolated by an automated method or by manual methods using gradient centrifugation.
ResultsThe results demonstrate the equivalence of the 3 methods in relation to the yield and final quality of the product, however with considerable differences between the costs of these procedures. In addition, this study also demonstrates the feasibility of the antigenic pulse with autologous tumor cell lysates, constituting a source of antigens, not only easily obtained and manipulated, but also specific to the patient's tumor.
ConclusionThese findings may have important implications for emerging centers interested in using this medical approach and potentially increase the access of a greater number of patients to this therapeutic option.
Recent advances in techniques, such as genomics and proteomics, have enabled great advances in the understanding of the pathophysiology of several solid and hematological tumors.1 Unfortunately, these advances have not yet been converted into therapeutic options that effectively increase the survival of these patients. This is particularly crucial in the case of patients in situations of limited resources, where the high costs and limited availability of clinical trials represent a barrier to the access to new therapies, as is the case of the recently developed T lymphocytes with chimeric antigen receptors – the CAR-T cells.2 Another equally relevant concern is the toxicity of the treatments currently available, such as that of chemotherapy/radiation, hematopoietic stem cell transplantation or the CAR-T cells themselves.3
In this context, autologous dendritic cells (DCs) pulsed with tumor antigens appear as a possible therapeutic strategy for cancer. In fact, since the discovery of DCs in 1972,4 the accumulated information of their antigenic presentation and lymphocyte activation functions has led to the idea of their potential use as an element of anti-tumor immune surveillance.5 The first study that tested this approach in cancer patients was published in 1996 and evaluated the use of DCs pulsed with tumor peptide in four patients diagnosed with follicular B cell lymphoma. All patients developed a detectable antitumor cellular response; two of the patients showed complete tumor regression after the vaccination schedule.6 Since then, results of several clinical trials have conclusively demonstrated the safety of these vaccines and their effectiveness in developing a specific immune response against various types of solid tumors7-9 and hematologic neoplasms.10,11
In the specific case of acute myeloid leukemia (AML), dendritic cells electroporated with WT-1 (Wilms Tumor 1) mRNA have been shown to be safe and effective in normalizing WT-1 levels in peripheral blood compatible with the induction of molecular remission, leading to a considerable increase in overall survival, when compared to conventional treatment alone.12,13 It is important to highlight the safe toxicological profile of these applications, in addition to cost-effectiveness analyses, further demonstrating the equivalence of this treatment in relation to the consolidation with allogeneic stem cell transplantation.14
Once effectiveness has been demonstrated, the next challenge to be overcome is the widespread implementation of this adjuvant treatment for cancer patients. However, as automated cell separators in closed systems are required for most of the protocols employed, the required methodology is an expensive one, representing a financial barrier in the case of institutions with limited resources.
Our center offers cancer treatment at no cost to patients treated by the government health system and has been developing this type of therapy in recent years for both lung cancer15 and AML.16 In addition to providing a new and viable therapeutic option for patients, we further evaluated the yield of DCs acquired under different methods of cell separation, which are evidenced in this article. This paper proposes to discuss and review the applicability of these methods and the search for new forms of antigenic pulse, considering the possible implications for emerging centers.
Materials and methodsPatients and clinical trialsThis study included seven patients diagnosed with acute myeloid leukemia treated at the Hematology and Transfusion Medicine Center of the University of Campinas and two patients with pulmonary adenocarcinoma treated at the Pulmonology Outpatient Clinic of this University Hospital between 2015 and 2019. All patients provided written informed consent. This study was approved by the Ethics Committee of the University and conducted in accordance with the International Conference on Harmonization (ICH) guidelines and applicable regulations governing clinical trials.
Leukapheresis, monocyte separation and differentiation into dendritic cellsThe in vitro generation of dendritic cells from peripheral blood mononuclear leukocytes followed a protocol previously developed in our laboratory,17 with modifications. The patients selected for vaccination underwent a leukapheresis procedure to collect mononuclear leukocyte suspension, using a continuous cell separator (Com.Tec, Fresenius Kabi, Bad Homburg, Germany), C4Y kit, program: PBSC-Lymphocyte. The processing of leukapheresis bags and subsequent differentiation and maturation of the DCs were carried out in an ISO 7 clean room (Class-10,000), equipped with Class-100 biological safety cabinets for aseptic handling of the material, located at the Pediatric Research Center of the University (CIPED-UNICAMP).
Cell suspensions collected by apheresis underwent monocyte separation (CD14+ cells) using three different methods:
- i)
Automated: automatic separation using a tubular system with magnetic beads (commercial system CliniMacs®);
- ii)
Manual 1: monocyte purification by centrifugation gradients, using the Ficoll® and Percoll® reagents (Sigma Aldrich, USA), achieved by a single passage of the complete amount of leukapheresis material, and;
- iii)
Manual 2: monocyte purification by centrifugation gradients, using the same procedure used for ‘Manual 1′, however divided into two consecutive passages, each with half of the leukapheresis material, to maintain the cell viability.
The resulting cell suspension, regardless of the separation process, was adjusted to the concentration of 2 × 106 viable cells/ml in the specific culture medium for differentiation of dendritic cells (DendriMACS™ GMP Medium, Miltenyi Biotec, Germany) and subsequently plated in 150 mm treated culture dishes (Corning, NY, USA). For differentiation into immature dendritic cells, adherent cells were cultured at 37 °C in 5% CO2 for five days in DendriMACS Medium containing 100 IU/ml penicillin and streptomycin (10 μg/ml), 50 ng/ml MACS GMP recombinant human granulocyte-macrophage colony-stimulating factor (GM-CSF) and 50 ng/ml MACS GMP recombinant human interleukin-4 (IL-4) (Miltenyi Biotec, Germany).
On day 3, the cultures were supplemented with the same cytokines and fresh medium. On day 6, maturation factors were added: 50 ng/ml of MACS GMP recombinant human tumor necrosis factor alpha (TNF-α) (Miltenyi Biotec, Germany) and 2.5 µg/ml prostaglandin E2 (PGE2) (Cayman Chemical, USA), following which the cells were cultured for two more days.
Antigenic pulse: RNA electroporation or diffusion of tumor lysates in coculturesMature DCs from AML patients were electroporated with the Wilms’ tumor gene 1 (WT1) mRNA on the eighth day of culture, produced through a plasmid kindly provided by Prof. Evelien Smits (Tumor Immunology Laboratory, University of Antwerp, Belgium). A total of 20ηg of WT1 mRNA were added to the cell suspension and then electroporated with a 300 V exponential decay pulse for 7 ms in 0.4 cm cuvettes, using the Electro Square Porator ECM 830 electroporator (BTX Genetronics, USA). After recovery, the DCs were subjected to quality control tests, as described below, and cryopreserved until administration of the vaccine.
Cell lysates from the patients with lung adenocarcinoma were obtained from the patient tumor itself and used as an antigenic source. To produce these cell lysates, a small sample of the tumor removed during surgery was subjected to physical maceration and the cells were then lysed for 5 cycles, alternating freezing (freezer at −80 °C, 30 min.) and washing (room temperature, 10 min.). The total cell disruption was validated microscopically using trypan blue staining. After sonication for 10 min, the lysate was centrifuged at 14,000 rpm (30 min, 4 °C). The supernatant was recovered and stored at −80 °C for later use in cocultures with dendritic cells during the maturation phase (48 h).
Final product evaluation and quality control testsThe phenotype, viability and expression of DC activation markers were determined by flow cytometry, using antibodies conjugated to fluorochromes: 7AAD, anti-CD14, anti-CD83, anti-CD86, anti-CD80, anti-CD11c and anti-human leucocyte antigen - DR isotype (anti-HLA-DR) (BD-Pharmingem). Samples for microbiological control (aerobic and anaerobic bacteria) were incubated in Bact-alert 120 medium (Organon Teknika, USA) on the final day of cell culture and before freezing. Immunocytochemistry was performed in cytospin preparations of the final product of the vaccine to document antigen expression after electroporation or incubation with tumor lysates: for WT-1 in the case of patients with AML and WT-1, cofilin-1, CEA and TTF1 in the case of lung cancer. Minimum criteria for vaccine release were considered: negative bacteriological control tests, DC phenotype, showing maturation markers with more than 80% viable (7AAD negative) DCs by flow cytometry, and positive immunocytochemistry.
Statistical analysisThe following data were compared between the 3 methods evaluated: total number of viable cells in the apheresis product, number of monocytes isolated, monocyte separation yield and total number of dendritic cells produced and ready for application, as well as the yield of dendritic cells produced in relation to the number of separated monocytes and the number of initial total leukocytes. Analysis of variance (ANOVA) was performed to compare the 3 groups, using the Vassarstats portal (http://vassarstats.net/), and results with p < 0.05 were considered significant.
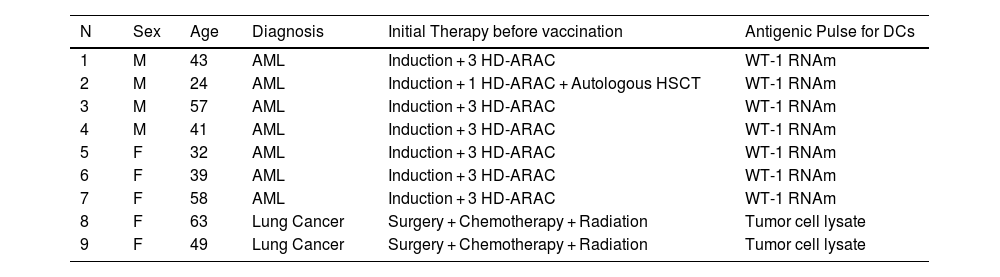
ResultsPatient clinical and laboratory characteristicsVaccine doses were produced for 7 patients diagnosed with AML and in complete remission after conventional treatment (chemotherapy or chemotherapy + autologous hematopoietic stem cell transplant) and 2 patients diagnosed with stage IIIA-N2 lung adenocarcinoma, treated with surgery, chemotherapy and radiation (clinical and demographic data detailed in Table 1).
Clinical and demographic data of patients.
For patients with AML, chemotherapy consisted of induction with daunorubicin and cytarabine and consolidation with high-dose cytarabine (HD-ARAC) or HD-ARAC plus autologous hematopoietic stem cell transplant (HSCT). For patients with lung adenocarcinoma, the post-surgery treatment consisted of chemotherapy with carboplatin + paclitaxel, followed by 25 sessions of radiation on the mediastinal region.
Comparison of cell yield and cost between the 3 cell separation methodsThree of the patients had vaccines produced by the automated monocyte separation in the CliniMacs® system and six patients, by the manual separation, using the in-house method with centrifugation gradients. In 3 of these cases of manual separation, the entire product of leukapheresis was subjected to the centrifugation process in gradients at once, whereas, in the other 3, the product of leukapheresis was divided in half, each one processed separately (therefore, in two parallel gradient separation processes).
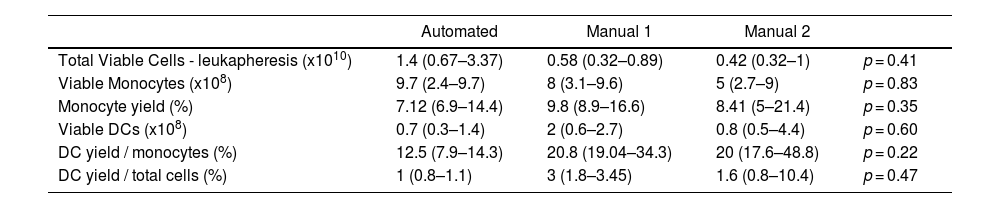
There were no differences between the 3 groups regarding the total number of viable cells in the apheresis product, number of isolated monocytes, yield of separate monocytes or total number of dendritic cells produced and ready for application, nor in the yield of dendritic cells, in relation to the number of separated monocytes or initial total leukocytes. The comparison between the three methods is presented in Table 2.
Comparison of cell yields among the different cell separation methods. Data are presented as median (min.-max.). DC: dendritic cells.
Regarding the quality of the final product, the following quality criteria were met for all patients: > 90% cell viability (verified by negativity in 7AAD), > 80% positivity for maturation markers (CD83, CD86, HLA-DR), negative bacterial cultures and positive immunocytochemistry (Figure 1).
.")
Immunocytochemistry demonstrating DCs with positive cytoplasmic labeling after antigenic pulse: A and B: DCs before and after electroporation with WT-1 mRNA, respectively, and internalization of antigen confirmed by reaction with anti-WT1 antibody; C and D: DCs before and after co-culture with lung cancer lysate positive for cofilin-1; internalization of antigen confirmed by reaction with anti-cofilin-1 antibody (panel D).
To compare costs between automated and manual methods, we assumed that the indirect costs, such as human resources and infrastructure, were the same for the three methods. Thus, we evaluated the cost differences of reagents and materials used in the processes, from the delivery of the leukapheresis bag to the laboratory until the monocytes were plated in culture, which included the cost of plastic materials, Clinimacs® kits and reagents for centrifugation in gradients. Despite the fact that this is not an accurate evaluation of cost and that even between the two manual methods there may be some variation in relation to the amount of reagents used, we were able to grossly observe a savings of approximately $285 dollars for each dose of vaccine (1 × 107 cells) produced by manual methods.
DiscussionVaccines using autologous dendritic cells have been used as treatment for relapse prevention in numerous types of tumors with positive results, including improved survival.12,13 Most of the protocols used for the production are based on the automated separation of monocytes from the patient peripheral blood and their subsequent differentiation in cultures to mature dendritic cells. This methodology assumes the use of a robust cell separation apparatus that includes kits of tubes, buffers and specific antibodies, adding considerable cost to the process. In addition, their availability may depend on the international importation of these materials and the use of specific machinery and, therefore, may encounter logistical barriers for their development on a universal scale.
In this study, we showed that manual monocyte separation through centrifugation gradients is a feasible technique for the production of these vaccines, using DCs pulsed with tumor antigens, with results equivalent to the automated method and, therefore, exempting the use of this specialized apparatus. For any of the methods compared, cell yields were satisfactory and equivalent, but with considerable differences in cost. These results may have important implications for developing countries, where the current treatment of several neoplasms still faces access restrictions, and where the development of therapies produced in-house at lower costs should be encouraged.
Though not statistically significant, there is a tendency towards a greater number of monocytes isolated by the automated method that has not been reflected in a greater number of dendritic cells produced. We can speculate that perhaps the contact with the various buffers, as well as the extensive piping system in the automated separation apparatus, may lead to physical changes in the monocytes that could impair their performance and differentiation in subsequent cultures. Although the specific causes for these changes have not yet been completely understood, significant morphological changes have in fact been described in dendritic cells, depending on the type of immunomagnetic separation used in the monocyte purification process.18
Regarding the cell separation based on centrifugation gradients, we chose to test a variation of the standard protocol, dividing the apheresis product into 2 portions, in the hypothesis that a single pass of the entire cell suspension could lead to lower separation yield by a greater cluster of cells and less contact with density gradient media. However, despite the small number of samples evaluated, the similarity of results obtained allowed us to discard the double protocol, which required more time on the bench.
Regarding the pulse of antigens, we used two strategies. Since WT-1 is widely expressed in AML, we chose to set up its mRNA electroporation, as this would allow the production of specific vaccines for the majority of the patients affected by the disease. On the other hand, in lung adenocarcinoma, there is no antigen expressed as specifically as WT-1 for AML and the evaluation of the expression of different proteins is necessary, subsequently requiring different transcripts/peptides for different patients. Therefore, we opted for the use of autologous tumor cell lysates, in order to provide a material composed of a pool of antigens, which are specific, not only to the disease, but also to the patient. This leads to the greater personalization of the product to the patient tumor characteristics, associated with other benefits: theoretically there is no need for immunohistochemical confirmation of any of the antigens at diagnosis and the surgical specimen is readily available and easily manipulated, requiring only temperature cycles and mechanical maceration. However, the negative point is the sole use for patients who have undergone surgical procedures or, in the case of hematological neoplasms, had their biopsy material stored before chemotherapy.
ConclusionThis study, therefore, reflects the search for more feasible and viable models of immunotherapy within the budget restrictions to which the projects are exposed in countries, such as Brazil. It was possible, through repeated manipulations and adjustments in cell separation protocols, to reach a satisfactory yield, in relation to the number of doses produced, but at a considerably lower cost with the use of manual techniques. The production and application of this type of cell vaccine is not new at several institutions in developed countries,19–21 however, the preferred method for cell separation has been essentially based on automated devices. Thus, our results demonstrate the efficacy of a manual method for clinical grade and routine application of DC vaccines, eliminating the need for automated cell separators. In addition, our study launches new bases for the development of alternative modalities of antigenic pulse for vaccines, such as tumor lysates, which deserve further studies in order to enable the development of more robust forms of immunotherapy.
FundingThis research was supported by the São Paulo Research Foundation (FAPESP), grant number 2017/21801-2.
We thank Raquel Susana Foglio for her important support with the English language review.


