
Assessing trends in the rate of transfusion-transmissible infections (TTIs) in blood donors is critical to the monitoring of the blood supply safety and the donor screening effectiveness. The objective of this study was to conduct a trend analysis of TTIs and associated demographic factors of donors at a public blood bank in the central Brazil.
MethodsA retrospective analysis (2010–2016) of blood donation data was performed to determine the prevalence of markers for TTIs. Multinomial and multivariate logistic regression were used to verify the association between the explanatory variables and TTIs. The trend was evaluated with the Prais Winsten’s regression analysis.
ResultsThe prevalence of TTIs was 4.04% (5,553 donors) among 137,209 donors, with a steady trend in the analyzed period. The seroprevalence for the hepatitis B virus (HBV), syphilis, hepatitis C virus (HCV), human immunodeficiency virus (HIV), Chagas disease, and human T-lymphotropic virus (HTLV) were 1.63%, 0.87%, 0.46%, 0.21%, 0.21% and 0.09%, respectively. The prevalence of HBV decreased (b = −0.021, p < 0.001), while syphilis increased (b = 0.112; p = 0.001), during the period investigated. The probability for a positive test for TTI was higher among donors with a low level of education, aged ≥30 years old, without stable marital status, and first-time donors.
ConclusionsEven with the reduction in HBV, the increased rate of syphilis may have contributed to the fact that the overall rate of TTIs did not decrease in the evaluated period.
Blood transfusion therapy is not entirely free from the risk of the transmission of infectious agents from the donor to the recipient. The most common infectious agents include: the Hepatitis B Virus (HBV), Hepatitis C Virus (HCV), Human Immunodeficiency Virus (HIV) and the bacterium Treponema pallidum, which causes syphilis. Therefore, the World Health Organization (WHO) recommends that all blood collected should be tested for transfusion-transmissible infections (TTIs) caused by these pathogens.1 In Brazil, in addition to screening for these TTIs, it is mandatory to screen all blood bags for human T-lymphotropic virus 1 and 2 (HTLV-1/2) and for Trypanosoma cruzi, which causes Chagas disease.2 In addition to the serological screening, all candidates for blood donation are submitted to clinical screening, which consists of an interview with a trained professional, with the objective of evaluating the clinical history and lifestyle of the donor in relation to exposure to risk factors for transfusion-transmissible diseases.2
The average prevalence rate of TTIs in low- and middle-income countries is higher, when compared to high-income countries, probably because of the precarious health services, hygiene habits, cultural factors and limitations in detection techniques.3
Continuous monitoring of infection rates in blood donors and awareness of their profiles is the major safety conduct, as the blood supply is directly associated with the incidence and prevalence rates of TTIs among blood donors. The TTIs rates result from the effectiveness of clinical and laboratory screening and the demographic composition of the donor population.4 Therefore, the objective of this study was to conduct an analysis over time of the prevalence of TTIs and associated factors in donors at a public blood bank in central Brazil.
MethodsSettingsThis research was carried out at the main public blood bank in the state of Goiás (Hemocentro de Goiás — HEMOGO), which is responsible for coordinating the other blood banks in the state. The HEMOGO is in Goiânia, capital of the state of Goiás, with approximately 1,466,105 inhabitants5 and a school enrollment ratio of 96.4% (population aged 6–14).6
The HEMOGO performs the donor recruitment, clinical and serological screening, collection, processing, distribution and transfusion. The HEMOGO is in central Goiânia, outside the hospital environment, and receives a large number of donors, approximately 25,000 per year. In addition to the collections in its own headquarters, the HEMOGO makes external collections through two mobile collection units. It is responsible for sending bags of blood components to the three largest hospitals in the metropolitan Goiânia and to several health units in the state of Goiás.
Study procedures/data collectionData from the volunteers who donated to the blood bank, and who were recruited by the mobile unit (external collection) from 1/1/2010 to 31/12/2016, were included in the analysis. Socio-economic data, such as age, gender, marital status, city of residence, frequency of donations and serological results, were obtained from the computer system of the blood bank. In order to preserve the privacy of donors required by law,2 donor names were not disclosed by the blood bank, being individualized by numerical codes. First-time donors and repeat donors were also included in the study. First-time donors are those who donated for the first time at this hemotherapy service, while repeat donors are those who donated at this hemotherapy service two or more times in a 12-month period.
Serological testingAccording to the Brazilian legislation,2 screening was performed at this blood bank for: hepatitis B, with HBsAg (chemiluminescent microparticle immunoassay, Abbott), anti-HBc IgG or IgG + IgM (chemiluminescent microparticle immunoassay, Abbott), and nucleic acid test (NAT) (Biomanguinhos, introduced in January/2016); hepatitis C, with HCV antibody test (chemiluminescent microparticle immunoassay Abbott) and NAT (Biomanguinhos, introduced in January/2013); HIV, with Anti-HIV1/2 or anti-HIV 1/2 and p24 antigen (chemiluminescent microparticle immunoassay Abbott) and NAT (Biomanguinhos, introduced in January/2013); HTLV-I/II, with antibody anti-HTLV-I-II (Enzyme-Linked Immunosorbent Assay, Abbott); syphilis, with non-treponemal antibody (VDRL, Abbott) until August/2014 and treponemal antibody from September/2014 (Enzyme-Linked Immunosorbent Assay, Abbott), and; Chagas disease, with Trypanosomal cruzi antibody (Enzyme-Linked Immunosorbent Assay, Abbott), according to the kit manufacturer instructions.
In this study, the donors with a reagent result for any of the tests in the first sample, were considered serologically inapt.
Statistical analysesData processing and statistical analyses were carried out using Stata 13.0 software (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX, US: StataCorp LP). Multinomial and multivariate logistic regression were used to verify the association between the explanatory variables and the positive serology results. For the trend analysis of the time series, we applied the Prais Winsten regression, which provided the beta value (slope of the line). A significance level of 95% was established for statistical analyses.
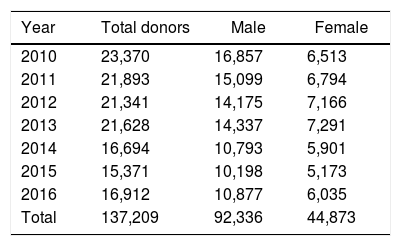
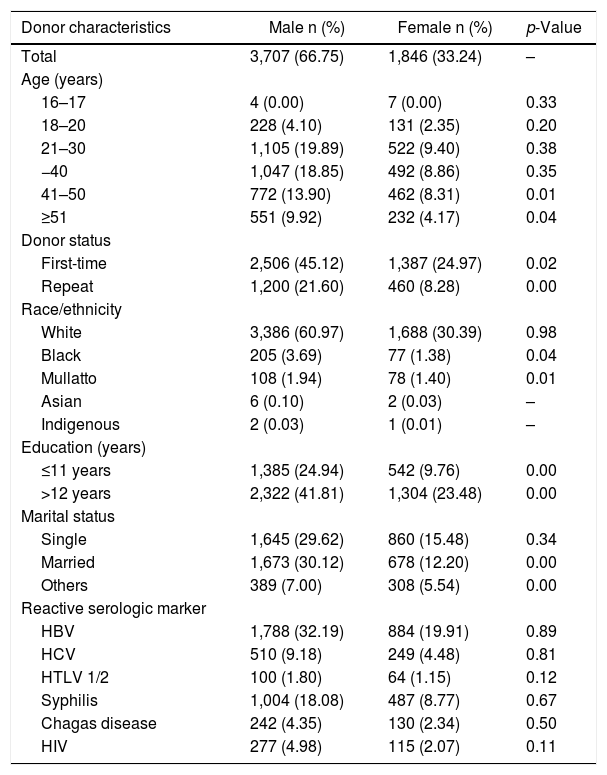
ResultsFrom January 2010 to December 2016, there were 149,891 blood donations, made by 137,209 donors, of whom 92,336 (67.29%) were males and 44,873 (32.70%) were females (Table 1). Most of them, 108,916 (79.37%) were volunteer donors and the remaining were replacement blood donors. Their ages ranged from 16 to 60 years. Overall, 5,553 donors (4.04%) had a reactive result for one or more TTIs. Among them, the majority were men, 41 years old or over, had more TTIs than women (p < 0.05) and were married (p < 0.05). Of those, 2,672 donors (48.11%) were HBV positive, 1,491 donors (26.85%) were syphilis positive, 759 donors (13.66%) were HCV positive, 392 donors (7.05%) were HIV-positive, 372 (6.69%) were positive for Chagas disease and HTLV reactivity was seen in 164 (2.95%). The overall prevalence of HIV, HBV, HCV, and syphilis was 0.28%, 1.94%, 0.55% and 1.08%, respectively. There were no differences in prevalence among men and women. Table 2 shows the demographic characteristics of the donors with reactive results for TTIs by gender, and reactive serologic markers.
Total blood donors by gender distribution, 2010–2016 in central western Brazil.
| Year | Total donors | Male | Female |
|---|---|---|---|
| 2010 | 23,370 | 16,857 | 6,513 |
| 2011 | 21,893 | 15,099 | 6,794 |
| 2012 | 21,341 | 14,175 | 7,166 |
| 2013 | 21,628 | 14,337 | 7,291 |
| 2014 | 16,694 | 10,793 | 5,901 |
| 2015 | 15,371 | 10,198 | 5,173 |
| 2016 | 16,912 | 10,877 | 6,035 |
| Total | 137,209 | 92,336 | 44,873 |
Demographic characteristics of blood donors with TTIs, by gender and reactive serologic markers in Brazil (2010–2016).
| Donor characteristics | Male n (%) | Female n (%) | p-Value |
|---|---|---|---|
| Total | 3,707 (66.75) | 1,846 (33.24) | – |
| Age (years) | |||
| 16–17 | 4 (0.00) | 7 (0.00) | 0.33 |
| 18–20 | 228 (4.10) | 131 (2.35) | 0.20 |
| 21–30 | 1,105 (19.89) | 522 (9.40) | 0.38 |
| −40 | 1,047 (18.85) | 492 (8.86) | 0.35 |
| 41–50 | 772 (13.90) | 462 (8.31) | 0.01 |
| ≥51 | 551 (9.92) | 232 (4.17) | 0.04 |
| Donor status | |||
| First-time | 2,506 (45.12) | 1,387 (24.97) | 0.02 |
| Repeat | 1,200 (21.60) | 460 (8.28) | 0.00 |
| Race/ethnicity | |||
| White | 3,386 (60.97) | 1,688 (30.39) | 0.98 |
| Black | 205 (3.69) | 77 (1.38) | 0.04 |
| Mullatto | 108 (1.94) | 78 (1.40) | 0.01 |
| Asian | 6 (0.10) | 2 (0.03) | – |
| Indigenous | 2 (0.03) | 1 (0.01) | – |
| Education (years) | |||
| ≤11 years | 1,385 (24.94) | 542 (9.76) | 0.00 |
| >12 years | 2,322 (41.81) | 1,304 (23.48) | 0.00 |
| Marital status | |||
| Single | 1,645 (29.62) | 860 (15.48) | 0.34 |
| Married | 1,673 (30.12) | 678 (12.20) | 0.00 |
| Others | 389 (7.00) | 308 (5.54) | 0.00 |
| Reactive serologic marker | |||
| HBV | 1,788 (32.19) | 884 (19.91) | 0.89 |
| HCV | 510 (9.18) | 249 (4.48) | 0.81 |
| HTLV 1/2 | 100 (1.80) | 64 (1.15) | 0.12 |
| Syphilis | 1,004 (18.08) | 487 (8.77) | 0.67 |
| Chagas disease | 242 (4.35) | 130 (2.34) | 0.50 |
| HIV | 277 (4.98) | 115 (2.07) | 0.11 |
There were 282 (5.07%) donors with multiple infections. Out of 282, 113 (40.07%) had HBV and syphilis coinfection, 38 (13.47%) had HBV and HCV coinfection, 33 (11.70%) presented with HIV and syphilis coinfection, 30 (10.63%), with HBV and Chagas disease coinfection, 19 (6.73%) co-infected with HIV and HBV and 36 donors (12.76%) had other co-infections. It was observed that 14 donors (4.96%) had three different TTIs.
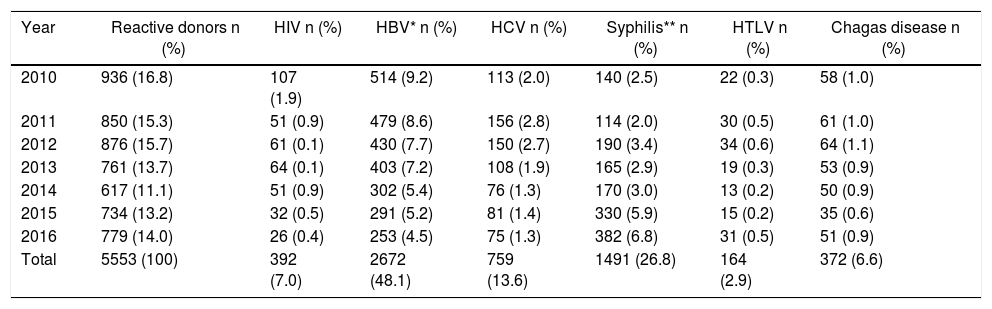
The most prevalent TTI among donors was hepatitis B (1.63%), which presented a decreasing trend (b = −0.021, p < 0.001), followed by an increased trend in syphilis (0.87%), which became the most prevalent TTI in 2015 (b = 0.112, p = 0.001). We found that the other infections presented a constant prevalence in the investigated period (Table 3). During the studied period, we did not detect any infection in the immunological window stage, investigated with the NAT method.
HIV, HBV, HCV, syphilis, HTLV and Chagas in blood donors in central western Brazil from 2010 to 2016.
| Year | Reactive donors n (%) | HIV n (%) | HBV* n (%) | HCV n (%) | Syphilis** n (%) | HTLV n (%) | Chagas disease n (%) |
|---|---|---|---|---|---|---|---|
| 2010 | 936 (16.8) | 107 (1.9) | 514 (9.2) | 113 (2.0) | 140 (2.5) | 22 (0.3) | 58 (1.0) |
| 2011 | 850 (15.3) | 51 (0.9) | 479 (8.6) | 156 (2.8) | 114 (2.0) | 30 (0.5) | 61 (1.0) |
| 2012 | 876 (15.7) | 61 (0.1) | 430 (7.7) | 150 (2.7) | 190 (3.4) | 34 (0.6) | 64 (1.1) |
| 2013 | 761 (13.7) | 64 (0.1) | 403 (7.2) | 108 (1.9) | 165 (2.9) | 19 (0.3) | 53 (0.9) |
| 2014 | 617 (11.1) | 51 (0.9) | 302 (5.4) | 76 (1.3) | 170 (3.0) | 13 (0.2) | 50 (0.9) |
| 2015 | 734 (13.2) | 32 (0.5) | 291 (5.2) | 81 (1.4) | 330 (5.9) | 15 (0.2) | 35 (0.6) |
| 2016 | 779 (14.0) | 26 (0.4) | 253 (4.5) | 75 (1.3) | 382 (6.8) | 31 (0.5) | 51 (0.9) |
| Total | 5553 (100) | 392 (7.0) | 2672 (48.1) | 759 (13.6) | 1491 (26.8) | 164 (2.9) | 372 (6.6) |
Prais Winsten: *b = −0.021, p < 0.001; **b = 0.112, p = 0.0.
A total of 63 donations, 0.04% of the total population of donors, was from indigenous individuals, 73% were male, the median age was 34 (18–57), 44% were married, 42% were first-time donors, 57% repeat donors and all of them lived in the urban region. The TTI rate among them was 4.76%, with an increasing trend (b = 0.082; p = 0.039), even though we did not observe any changes in the number of donations. The cases of TTIs among indigenous donors were syphilis, Chagas disease, and hepatitis B and syphilis co-infection.
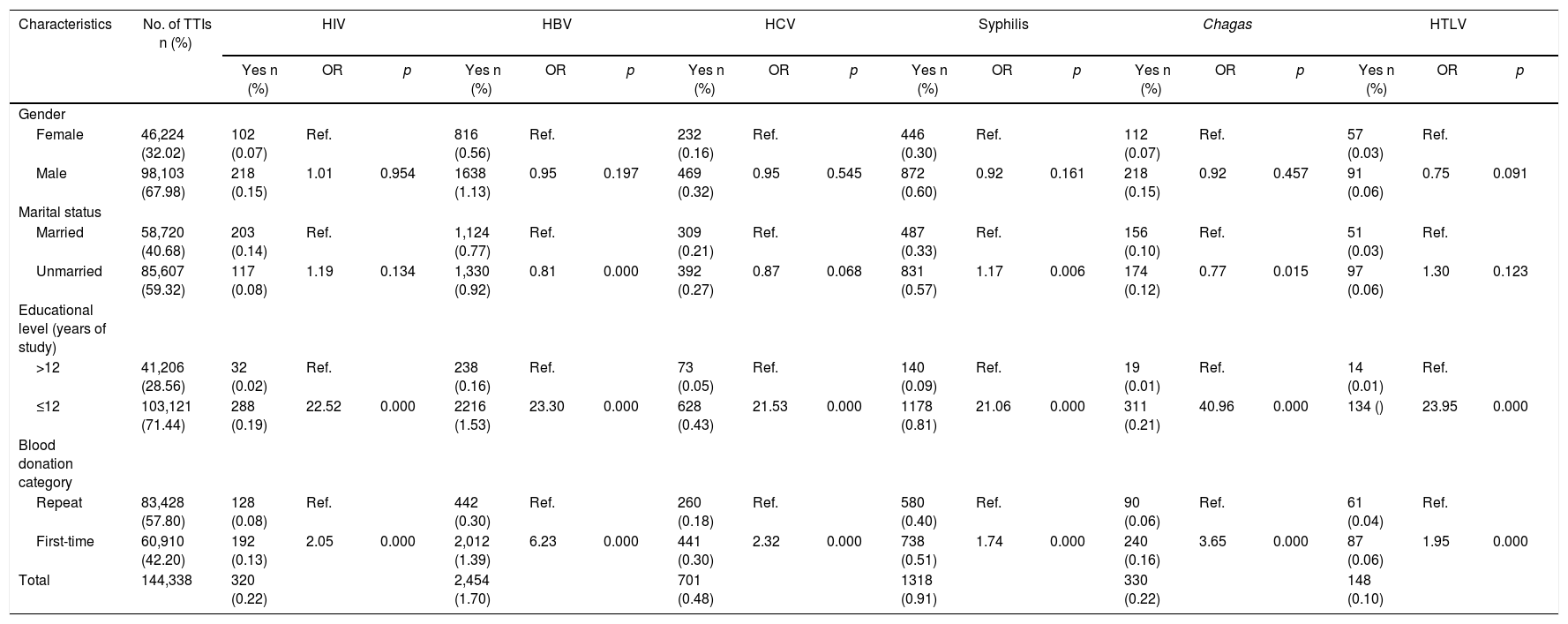
Among unmarried donors, the TTI rate was 3.61% and the chance of having syphilis was higher (OR = 1.17, p < 0.006) than for married donors. Among donors with 12 years or less of study, the rate was 4.29% and they presented a higher chance for any TTI (OR 2.0, p < 0.0001). Among the first-time donors, the chance of presenting positive TTI tests was two-fold higher than for repeat donors (OR = 2.0, p < 0.0001), with HBV infection being six times more likely to occur (Table 4).
Blood donors characteristics and adjusted odds ratios for transfusion-transmissible infections (TTIs), 2010–2016, Brazil.
| Characteristics | No. of TTIs n (%) | HIV | HBV | HCV | Syphilis | Chagas | HTLV | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes n (%) | OR | p | Yes n (%) | OR | p | Yes n (%) | OR | p | Yes n (%) | OR | p | Yes n (%) | OR | p | Yes n (%) | OR | p | |||
| Gender | ||||||||||||||||||||
| Female | 46,224 (32.02) | 102 (0.07) | Ref. | 816 (0.56) | Ref. | 232 (0.16) | Ref. | 446 (0.30) | Ref. | 112 (0.07) | Ref. | 57 (0.03) | Ref. | |||||||
| Male | 98,103 (67.98) | 218 (0.15) | 1.01 | 0.954 | 1638 (1.13) | 0.95 | 0.197 | 469 (0.32) | 0.95 | 0.545 | 872 (0.60) | 0.92 | 0.161 | 218 (0.15) | 0.92 | 0.457 | 91 (0.06) | 0.75 | 0.091 | |
| Marital status | ||||||||||||||||||||
| Married | 58,720 (40.68) | 203 (0.14) | Ref. | 1,124 (0.77) | Ref. | 309 (0.21) | Ref. | 487 (0.33) | Ref. | 156 (0.10) | Ref. | 51 (0.03) | Ref. | |||||||
| Unmarried | 85,607 (59.32) | 117 (0.08) | 1.19 | 0.134 | 1,330 (0.92) | 0.81 | 0.000 | 392 (0.27) | 0.87 | 0.068 | 831 (0.57) | 1.17 | 0.006 | 174 (0.12) | 0.77 | 0.015 | 97 (0.06) | 1.30 | 0.123 | |
| Educational level (years of study) | ||||||||||||||||||||
| >12 | 41,206 (28.56) | 32 (0.02) | Ref. | 238 (0.16) | Ref. | 73 (0.05) | Ref. | 140 (0.09) | Ref. | 19 (0.01) | Ref. | 14 (0.01) | Ref. | |||||||
| ≤12 | 103,121 (71.44) | 288 (0.19) | 22.52 | 0.000 | 2216 (1.53) | 23.30 | 0.000 | 628 (0.43) | 21.53 | 0.000 | 1178 (0.81) | 21.06 | 0.000 | 311 (0.21) | 40.96 | 0.000 | 134 () | 23.95 | 0.000 | |
| Blood donation category | ||||||||||||||||||||
| Repeat | 83,428 (57.80) | 128 (0.08) | Ref. | 442 (0.30) | Ref. | 260 (0.18) | Ref. | 580 (0.40) | Ref. | 90 (0.06) | Ref. | 61 (0.04) | Ref. | |||||||
| First-time | 60,910 (42.20) | 192 (0.13) | 2.05 | 0.000 | 2,012 (1.39) | 6.23 | 0.000 | 441 (0.30) | 2.32 | 0.000 | 738 (0.51) | 1.74 | 0.000 | 240 (0.16) | 3.65 | 0.000 | 87 (0.06) | 1.95 | 0.000 | |
| Total | 144,338 | 320 (0.22) | 2,454 (1.70) | 701 (0.48) | 1318 (0.91) | 330 (0.22) | 148 (0.10) | |||||||||||||
The analysis of the blood donations in the central region of Brazil showed that TTI rates were constant between 2010 and 2016 and that first-time blood donors, donors over 30 years old, and those with a lower level of schooling, presented the highest chances of having TTIs. The prevalence of TTIs was similar, when compared to the national average in the period 2010–2015, which was 3.89%.7 However, when compared with other regions of the country, we observed that the rate found is lower than that found in the southern region (5.0%),8 the northern region (5.23%) and the northeastern region (4.08%) regions.7 Therefore, in countries with a continental dimension, such as Brazil, these rates vary according to the region, as they are influenced by different social, cultural and economic conditions. According to the WHO, the prevalence of HBV, HCV, and HIV infections among blood donors in different parts of the world ranges from 0.008 to 6.08%, 0.004 to 1.96%, and 0.0004 to 2.0%, respectively.9 In Brazil, TTI rates among blood donors range from 0.28 to 23.2% for HBV,10,11 0.1 to 1.1% for HCV,10,12 0.03 to 0.2% for HIV,13,14 0.01 to 0.14% for HTLV,15,16 0.14 to 0.88% for syphilis,17,18 and 0.1 to 0.6% for Chagas disease.8,19
During the study period, hepatitis B was the most prevalent infection among blood donors, however, a declining trend has been observed over the years, except in 2015. The rate found for hepatitis B was concordant with the expected range for the Americas, which is 0.4–1.6%.20 In addition, in the central region of Brazil, hepatitis B rates decreased from 9.42% in 2001 to 3.04% in 2010.21 Likewise, in southern Brazil, hepatitis B rates fell from 4.2% to 1.8% between 2003 and 2012.8 Several factors may be involved in this reduction, such as increased vaccination policies and changes in the legislation, such as the requirement for the NAT for all samples,2 which promotes a more rigorous donor selection to improve transfusion safety.
The prevalence of HCV (0.46%), HIV (0.21%), Chagas disease (0.21%) and HTLV (0.09%) found in this research is similar to the rates found in other studies conducted with blood donors in Brazil.8,18 These rates are higher in countries, such as Brazil, which is an endemic region for the Chagas disease, when compared to developed countries.
Syphilis rates increased between 2010 and 2016, mainly in 2015. This result is concordant with the observation that syphilis incidence in Brazil increased from 2.0 to 42.5 cases per 100 thousand inhabitants between 2010 and 2016.22 At least two factors may explain the increasing trend in syphilis among the blood donors. First, changes in the syphilis screening assay; a non-treponemal testing was used until August 2014. From September 2014 to the present, a more sensitive and specific syphilis screening assay has been implemented (treponemal antibody). Second, the scarce availability of Benzathine penicillin. In the second half of 2014, the supply of raw material and diluent used to manufacture Benzathine benzylpenicillin was interrupted, leading to reduced availability of this medication in the country, thus compromising the treatment of patients.23 This also led to the increase by 27.8% in the number of syphilis cases in the Brazilian population between 2015 and 2016,22 directly reflecting the uptake and growth in positive tests among blood donors.
The prevalence of TTIs among self-declared indigenous donors in the present study was 4.76%, which was high when compared to a recent study for screening for HIV and syphilis in indigenous communities in the Amazon region (1.74%).24 It is probable that the indigenous population in Goiás has more contact with the urban population than that in Amazonia, since all indigenous subjects in our study are from the urban region. These results are in line with data from the literature that show that 99.9% of the indigenous population living in Goiania lives in the urban area.6 Furthermore, national data has shown increasing trends in HIV infection among indigenous people in the northern region of the country in the last decade.25 This population is subject to an increased vulnerability to infection due to the structural conditions of life and the profound epidemiological transition experienced by indigenous people, which promotes the spread of HIV and other sexually transmitted infections.26
Repeat donors usually have an altruistic behavior and feel responsible for the safety of blood-group recipients.27 These donors are tested every time they donate, and when positive for any of the infectious agents, these individuals will not be able donate blood any longer. In this way, the prevalence of TTIs in this donor category is reduced.28 These observations may explain why we found higher probability of first-time donors presenting TTIs, when compared to repeat donors.
The observed relationship between the low educational level and the higher age with the greater chance of the donor presenting TTIs was also found in other studies conducted in Brazil29,30 and in the world.31,32 A low educational level may be associated with lower financial resources, worse hygiene conditions and scarcer healthy life habits, which are risk factors for TTIs.33
We believe that the change in the screening test for syphilis has impacted the overall serological inability rate. The introduction of the NAT methodology had no influence on the detection of donors in the immunological window period, but this result may be due to the low number of donors included in this study.
This study may contribute to a better characterization of the profile of the donations at a public blood bank in Brazil. Our findings demonstrate trends in the pattern of the blood donations and the agents responsible for the TTIs over seven years. Once adequately collected, processed and analyzed, data from blood banks are a significant source of epidemiological information,34 and these results can support the development of donor recruitment strategies, contributing to the assurance of transfusion safety related to TTIs.
Conflict of interestThe authors declare no conflicts of interest.
The authors Lívia Pessoni and Érica Aquino made substantial contributions to the research design, the acquisition, analysis and interpretation of data and the drafting of the paper. The author Keila Alcântara was responsible for revising it critically and approving the submitted and final versions.
We would like to thank FAPEG and CAPES (AUXPE 1665/2016).



