




Hematology Specialist Association 18. National Congress
More infoMultiple myeloma (MM) and acute myeloid leukemia (AML) are malignant clonal diseases of cells in different lineages. Only 79 cases of the two diseases occurring together have been reported in Pubmed in the last 10 years. However, simultaneous occurrence of MM and AML on presentation in chemotherapy-naive patients is rare, with only a 25 cases reported in the literature so far. (1)This case presents our experience with a patient who was diagnosed with AML shortly after the diagnosis of MM.
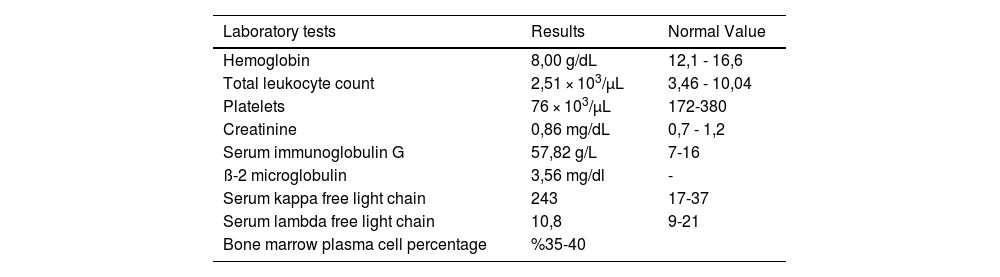
Case reportA 57-year old male patient was referred to hematology due to pancytopenia. Serum immunofixation confirming monoclonal gammopathy of IgG kappa was detected. ß-2 microglobulin was found as 3,56 mg/dL. All routine tests required for MM diagnosis and follow-up were performed. (table 1) Bone marrow biopsy showed 40% plasma cell infiltration stained with CD38, CD138 and kappa. PET/CT scan revealed lytic lesions in the bones. t(4;14) was found positive in fluorescence in situ hybridization analysis. Bortezomib, lenalidomide, dexamethasone (VRD) regimen was started. After 4 cycles of VRD, the patient was hospitalized due to febrile neutropenia and severe dyspnea. Pulmonary embolism and pneumonic infiltration were not detected in thorax CT. However; bilateral septal edema and pleural effusion up to 3,5 cm were detected. Pleural fluid sampling was performed. No infectious agent was detected in exudative effusion. 3,25% myeloid blasts, 1,99% plasma cells were found by flow cytometry of pleural fluid. (figure 1) A bone marrow biopsy was performed again due to blasts in the pleural fluid results. Biopsy showed 40% myeloid blasts (CD117 and CD34) and 18% plasma cells in the bone marrow parenchyma. (figure 2) We decided to treat the patient with 7+3 induction chemotherapy (Idarubicin and cytarabine) with daratumumab and dexamethasone (Dara-d). After induction and one course of dara-d, bone marrow biopsy was performed again to evaluate response.
The patient could not achieve remission and died due to acute respiratory failure.
Results
ConclusionMultiple myeloma (MM) and acute myeloid leukemia (AML) may usually develop in the same patient but they are generally seen in MM patients receiving chemotherapy and in due course of treatment AML develops. (2) Presence of AML with MM in a shortly after treatment begins is an extremely rare occurrence. Concurrent diagnosis of these two hematological malignancies yields a poor prognosis. (3)References:(1) Jamal I, Shuchismita S, Choudhary V. Twin Malignancy of Acute Myeloid Leukemia and Multiple Myeloma in a Chemotherapy-Naïve Patient: A Rare Occurrence. J Lab Physicians. 2022 Oct 20;15(2):306-310. doi: 10.1055/s-0042-1757588. PMID: 37599817; PMCID: PMC10437150.(2) Parapia L, Abbott CR, Masters G, Roberts BE. Simultaneous pre sentation of acute myelomonocytic leukaemia and multiple myeloma. Acta Haematol 1982;68(02):153–156 (3) Annino L, Martino P, Barsotti P, Serra P, MArinozzi V, Mandelli F. Multiple myeloma and acute myelomonocytic leukemia: simultaneous occurrence without previous chemotherapy. Acta Haematol 1980;64:195–200
Laboratory and bone marrow biopsy findings of the patient at the time of diagnosis

Figure 1: (A) Chest X-ray showed pleural effusion. (B) Pleural fluid was positive for myeloid blasts. (C) Plasma cell persentage of pleural fluid.

Figure 2: (A) Bone marrow biopsy, H & E stain × 40. The bone marrow is hypercellular. (B) Bone marrow biopsy, H & E stain × 40, The number of normal hematopoietic elements is markedly increased, the infiltrate consists of plasma vcells and blasts. (C) Approximately 40% CD34 staining in the bone marrow parenchyma. (D) CD117 staining cells are 18% of the mrrow. (E) Number of cells stained with CD138, 18% of parenchyma.


