


Hematologic neoplasms are associated with mutations in hematopoietic cells and chromosomal abnormalities. During aging, about 2–3% of the elderly have chromosomal abnormalities arising from clonal mosaicism, the immune system is impaired and the bone marrow loses its ability to replace blood cells.
ObjectiveTo describe the epidemiological and cytogenetic profile of hematological malignancies, highlighting the frequency of chromosomal alterations in these neoplasms associated with aging.
MethodA retrospective cross-sectional study with analysis of karyotype exams results was performed in the Cytogenetic Laboratory of thee Blood Center of the Faculdade de Medicina de Marilia (FAMEMA) between 1998 and 2016. Blood samples from child and adult patients with different hematological malignancies treated in the Onco-hematology Outpatient Clinics of the local blood center and hospitals, and external clinics were tested.
ResultsKaryotype exam results of 746 patients with a mean age of 54.7 years (±23.1) were analyzed. The elderly had the highest frequency of hematological malignancies (50.9%), followed by adults (38.3%) and young people (10.7%); elderly women had the highest percentage (55.0%). Normal karyotypes (46,XX/46,XY) were more common (61.8%) compared to abnormal karyotypes, especially among the elderly (56.4%). Myeloproliferative neoplasms were an exception with 67.4% of abnormal karyotypes.
ConclusionThere is a higher frequency of hematological malignancies among the elderly. It is possible to conclude that failures in genomic mechanisms and hematopoiesis with aging lead to the formation of cells with the chromosomal alterations found in hematological malignancies.
Hematological malignancies are often associated with mutations or asymmetric divisions in immature blood cell lines and specific chromosomal abnormalities (numerical and structural) such as aneuploidies, deletions, translocations and inversions.1,2
The first chromosomal alteration linked to cancer was identified in 1960, by Peter Nowell and David Hungerford, when they discovered the Philadelphia (Ph) chromosome in blood samples from a patient with chronic myeloid leukemia (CML).3 Since then, the cytogenetic diagnosis of chromosomal alterations in hematological malignancies has been helping physicians and researchers in the classification, staging and prognosis of these neoplasms.4
Aging is identified by some epidemiological studies as the main risk factor for the development of cancer.5 In addition to reduced efficiency of the immune system in the elderly, the bone marrow loses its ability to properly replace blood cells.6 About 2–3% of the elderly have chromosomal abnormalities originating from clonal mosaicism in blood samples. The presence of these abnormalities is associated with a ten-times greater risk to develop hematological malignancies.7
The study of cytogenetic alterations in geriatric oncology can provide better therapeutic and individual targeting of elderly patients and favor health and quality of life in this population that is more susceptible to aggressive pathologies.
The objective of this study was to characterize the epidemiological and cytogenetic profiles of different hematological malignancies, describing the prevalence of numerical and structural chromosomal alterations in neoplasms during the aging process.
MethodsStudy designA cross-sectional retrospective study based on the review of cytogenetic reports and karyotype exam results was performed in the Cytogenetic Laboratory of the Blood Center of the Faculdade de Medicina de Marilia (FAMEMA) from March 1998 to March 2016. The local Ethics Research Committee approved this study.
MaterialThe karyotype exam results utilized in this study were from samples obtained using peripheral blood or by bone marrow aspiration of the iliac crest or sternum bone of patients with different hematological malignancies.
Interpretation of the cytogenetic reports and classification of karyotype exams as normal or altered (numerical and structural chromosomal alterations) followed the International Cytogenetic Classification – ISCN 2013.8
Study populationPatients with hematological and lymphoid neoplasms were included in the study with patients (child and adult) being attended in the Onco-hematology Outpatient Clinic of the Blood Center of FAMEMA, the Clinical Oncology Department, Assis Regional Hospital and external oncology clinics. The cytogenetic monitoring of neoplasms in different phases was divided into two groups according to the clinical evolution and prognosis: one group of patients was submitted to a karyotype examination on only one occasion and a second group had more than one karyotype examination over the years.
Patients were grouped according to age using the Brazilian Institute of Geography and Statistics (IBGE) and World Health Organization (WHO) classifications: young (0–19 years), adult (20–59 years) and elderly (60 years of age or older).9,10 The age of the patients at the time of the first karyotype examination and cytogenetic diagnosis was considered for the stratification into age groups.
Inclusion and exclusion criteriaPatients with karyotype results of onco-hematological diseases as defined by the WHO classification criteria for hematological and lymphoid neoplasms based on the morphology and specific cytogenetic alterations of each malignancy were included in this study.11,12 Patients submitted to bone marrow transplantation, patients without information of their date of birth or hypothesis of neoplasm diagnosis and patients presenting symptoms or characteristics associated with neoplasms but without reference to a specific pathology were excluded from the study. Moreover, patients under chemotherapy at the first collection of oncological material and cytogenetic analysis were excluded.
Statistical analysisCategorical variables such as the demographic, clinical and cytogenetic data of patients are presented as relative and absolute frequencies. Pearson's chi-square test and Fisher's exact test were used to compare variables in relation to the studied parameters with a p<0.0001 being adopted to define significance. All statistical analyses were performed with the Statistical Package for Social Science (SPSS), version 17.0.
ResultsThis study analyzed the results of karyotype exams in cytogenetic reports at the diagnosis of 746 patients with hematological and lymphoid neoplasms since 1998. Information collected was stored in a database of the Cytogenetics Laboratory of FAMEMA. Of the 746 patients enrolled in the study, 604 patients performed the examination once and 142 patients, who had continued cytogenetic monitoring over the years, performed the karyotype examination more than once (Figure 1).

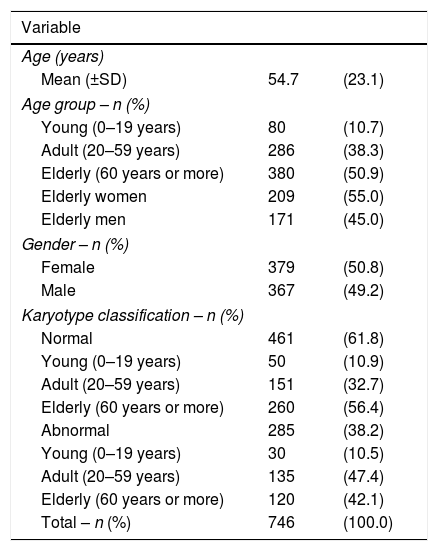
The mean age of the study sample was 54.7 (±23.1) years and 379 (50.8%) patients were female. The highest prevalence of hematological malignancies was found in the elderly (50.9%), followed by the adult age group (38.3%) and the young age group (10.7%). Of the elderly, the women were diagnosed with the highest percentage of hematological malignancies (55.0%). The results show a higher prevalence of normal karyotypes among the elderly (56.4%), when compared to adults (32.7%) and children (10.9%) (Table 1).
Demographic profile and karyotype classification of patients with hematological neoplasms.
| Variable | ||
|---|---|---|
| Age (years) | ||
| Mean (±SD) | 54.7 | (23.1) |
| Age group – n (%) | ||
| Young (0–19 years) | 80 | (10.7) |
| Adult (20–59 years) | 286 | (38.3) |
| Elderly (60 years or more) | 380 | (50.9) |
| Elderly women | 209 | (55.0) |
| Elderly men | 171 | (45.0) |
| Gender – n (%) | ||
| Female | 379 | (50.8) |
| Male | 367 | (49.2) |
| Karyotype classification – n (%) | ||
| Normal | 461 | (61.8) |
| Young (0–19 years) | 50 | (10.9) |
| Adult (20–59 years) | 151 | (32.7) |
| Elderly (60 years or more) | 260 | (56.4) |
| Abnormal | 285 | (38.2) |
| Young (0–19 years) | 30 | (10.5) |
| Adult (20–59 years) | 135 | (47.4) |
| Elderly (60 years or more) | 120 | (42.1) |
| Total – n (%) | 746 | (100.0) |
SD: standard deviation.
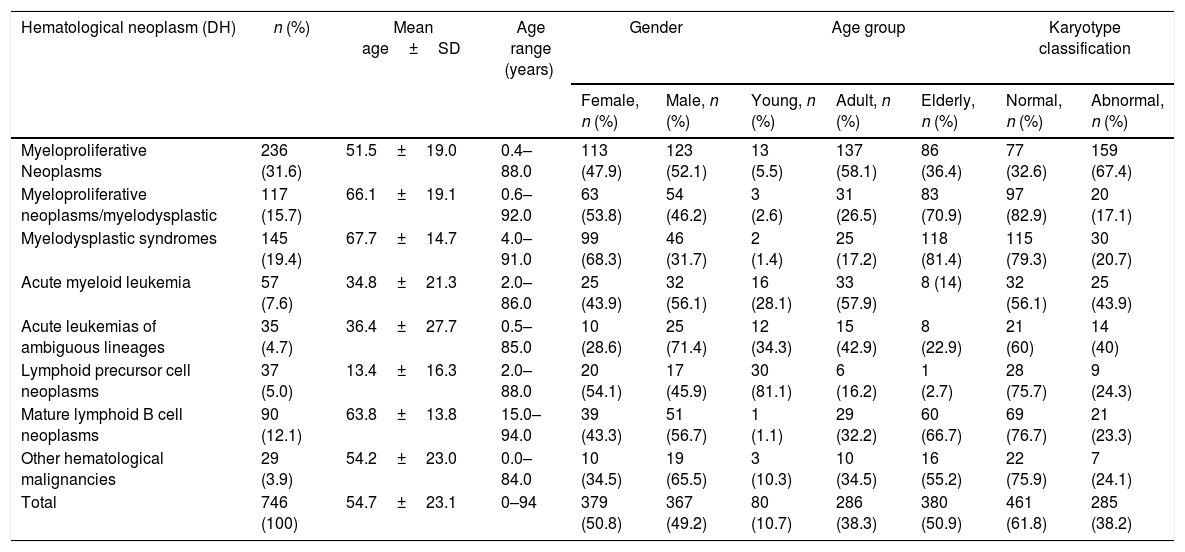
In this study, there were more normal (46,XX/46,XY: 461 – 61.8%) than abnormal karyotypes (285 – 38.2%). Myelodysplastic neoplasms, myelodysplastic syndromes, mature lymphoid B neoplasms, and acute lymphoid leukemia (ALL) had normal karyotypes in 82.9%, 79.3%, 76.7%, and 75.7% of the cases, respectively. However, myeloproliferative neoplasms presented 67.4% of abnormal karyotypes (Table 2).
Distribution of demographic variables and karyotype classification of patients with hematological malignancies evaluated by Cytogenetic Lab of FAMEMA from 1998 to 2016.
| Hematological neoplasm (DH) | n (%) | Mean age±SD | Age range (years) | Gender | Age group | Karyotype classification | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Female, n (%) | Male, n (%) | Young, n (%) | Adult, n (%) | Elderly, n (%) | Normal, n (%) | Abnormal, n (%) | ||||
| Myeloproliferative Neoplasms | 236 (31.6) | 51.5±19.0 | 0.4–88.0 | 113 (47.9) | 123 (52.1) | 13 (5.5) | 137 (58.1) | 86 (36.4) | 77 (32.6) | 159 (67.4) |
| Myeloproliferative neoplasms/myelodysplastic | 117 (15.7) | 66.1±19.1 | 0.6–92.0 | 63 (53.8) | 54 (46.2) | 3 (2.6) | 31 (26.5) | 83 (70.9) | 97 (82.9) | 20 (17.1) |
| Myelodysplastic syndromes | 145 (19.4) | 67.7±14.7 | 4.0–91.0 | 99 (68.3) | 46 (31.7) | 2 (1.4) | 25 (17.2) | 118 (81.4) | 115 (79.3) | 30 (20.7) |
| Acute myeloid leukemia | 57 (7.6) | 34.8±21.3 | 2.0–86.0 | 25 (43.9) | 32 (56.1) | 16 (28.1) | 33 (57.9) | 8 (14) | 32 (56.1) | 25 (43.9) |
| Acute leukemias of ambiguous lineages | 35 (4.7) | 36.4±27.7 | 0.5–85.0 | 10 (28.6) | 25 (71.4) | 12 (34.3) | 15 (42.9) | 8 (22.9) | 21 (60) | 14 (40) |
| Lymphoid precursor cell neoplasms | 37 (5.0) | 13.4±16.3 | 2.0–88.0 | 20 (54.1) | 17 (45.9) | 30 (81.1) | 6 (16.2) | 1 (2.7) | 28 (75.7) | 9 (24.3) |
| Mature lymphoid B cell neoplasms | 90 (12.1) | 63.8±13.8 | 15.0–94.0 | 39 (43.3) | 51 (56.7) | 1 (1.1) | 29 (32.2) | 60 (66.7) | 69 (76.7) | 21 (23.3) |
| Other hematological malignancies | 29 (3.9) | 54.2±23.0 | 0.0–84.0 | 10 (34.5) | 19 (65.5) | 3 (10.3) | 10 (34.5) | 16 (55.2) | 22 (75.9) | 7 (24.1) |
| Total | 746 (100) | 54.7±23.1 | 0–94 | 379 (50.8) | 367 (49.2) | 80 (10.7) | 286 (38.3) | 380 (50.9) | 461 (61.8) | 285 (38.2) |
DH: diagnostic hypothesis; SD: standard deviation.
On evaluating diagnostic hypotheses in different age groups, it was observed that neoplasms of lymphoid precursor cells, such as ALL, were more frequent among young patients, with a mean age of 13.4 years in 81.1% of the cases. While myelodysplastic neoplasms, myelodysplastic syndromes and mature B cell lymphoproliferative neoplasms were predominant in elderly patients with percentages of 70.9%, 81.4% and 66.7%, respectively and mean ages of 66.1, 67.7, and 63.8 years. In adult patients, myeloproliferative neoplasms and acute myeloid leukemia (AML) predominated in 58.1% and 57.9% of the cases, respectively (Table 2).
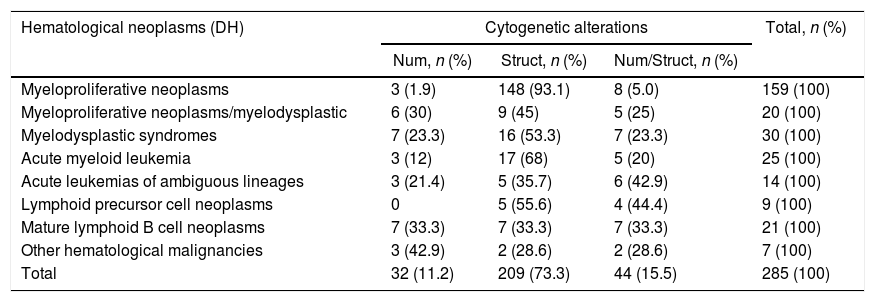
The most common cytogenetic alterations, observed in 73.3% of the cases (209 karyotypes), were structural. About 15.5% of the cases had both structural and numerical alterations (44 karyotypes) (Table 3). Among the hematologic neoplasms with structural cytogenetic alterations were myeloproliferative neoplasms (93.1%), myelodysplastic neoplasms (45%), myelodysplastic syndromes (53.3%) and AML (68%). However, acute leukemias presented a higher frequency of numerical/structural cytogenetic alterations (42.9%) (Table 3).
Frequency and classification of cytogenetic alterations in hematological malignancies (DH) between 1998 and 2016.
| Hematological neoplasms (DH) | Cytogenetic alterations | Total, n (%) | ||
|---|---|---|---|---|
| Num, n (%) | Struct, n (%) | Num/Struct, n (%) | ||
| Myeloproliferative neoplasms | 3 (1.9) | 148 (93.1) | 8 (5.0) | 159 (100) |
| Myeloproliferative neoplasms/myelodysplastic | 6 (30) | 9 (45) | 5 (25) | 20 (100) |
| Myelodysplastic syndromes | 7 (23.3) | 16 (53.3) | 7 (23.3) | 30 (100) |
| Acute myeloid leukemia | 3 (12) | 17 (68) | 5 (20) | 25 (100) |
| Acute leukemias of ambiguous lineages | 3 (21.4) | 5 (35.7) | 6 (42.9) | 14 (100) |
| Lymphoid precursor cell neoplasms | 0 | 5 (55.6) | 4 (44.4) | 9 (100) |
| Mature lymphoid B cell neoplasms | 7 (33.3) | 7 (33.3) | 7 (33.3) | 21 (100) |
| Other hematological malignancies | 3 (42.9) | 2 (28.6) | 2 (28.6) | 7 (100) |
| Total | 32 (11.2) | 209 (73.3) | 44 (15.5) | 285 (100) |
DH: diagnostic hypothesis; Num: numerical alteration; Struct: structural alteration.
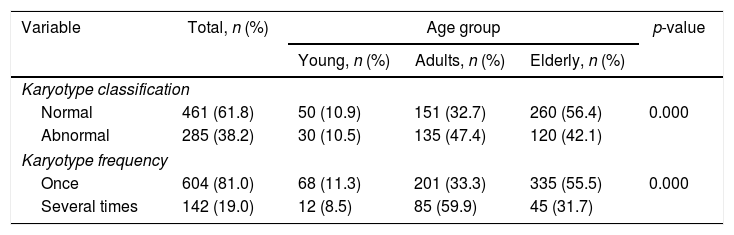
Significant differences were observed in the number of normal (46,XX/46,XY) compared to abnormal karyotypes (numerical and structural chromosomal alterations) for all age groups (p<0.0001). The adult age group had the highest percentage of abnormal karyotypes (47.4%), followed by the elderly population (42.1%) and the young population (10.5%) (Table 4).
Association between studied variables and age group of patients with hematological malignancies.
| Variable | Total, n (%) | Age group | p-value | ||
|---|---|---|---|---|---|
| Young, n (%) | Adults, n (%) | Elderly, n (%) | |||
| Karyotype classification | |||||
| Normal | 461 (61.8) | 50 (10.9) | 151 (32.7) | 260 (56.4) | 0.000 |
| Abnormal | 285 (38.2) | 30 (10.5) | 135 (47.4) | 120 (42.1) | |
| Karyotype frequency | |||||
| Once | 604 (81.0) | 68 (11.3) | 201 (33.3) | 335 (55.5) | 0.000 |
| Several times | 142 (19.0) | 12 (8.5) | 85 (59.9) | 45 (31.7) | |
p<0.0001.
On correlating the frequency of karyotype examinations with age group, there was a significant difference (p<0.0001). Among the elderly, the number of patients who performed a single cytogenetic analysis was higher (88.2%) than the number of patients who underwent karyotype examinations on several occasions (11.8%) (Table 4).
DiscussionThe results of this study corroborate the literature by highlighting the elderly as the population most affected by hematological malignancies. According to the HAEMACARE project developed in Europe between 2000 and 2002 the incidence of lymphoid malignancies and myeloid neoplasms tends to increase with age, peaking between 75 and 99 years.13 Similar studies have shown that the probability of being diagnosed with some hematological malignancy increases in over 65-year-old individuals.14
Aging is associated with physiological structural and functional alterations that favor the predominance of chronic diseases and cancers in the elderly. The prevalence in the number of hematological malignancies in older patients results from associations of three main factors: physiological impairment specific to age, modern lifestyle and genetic aspects.5
Hematological malignancies are more aggressive in the elderly population with impairment of the bone marrow and immune system. Alterations associated with ineffective hematopoiesis include deficiencies in the innate immune system (decreased natural killer cell activity and phagocytosis) and in the adaptive immune system (reductions of B and T lymphocytes).15 Typical cell alterations of hematopoiesis in the elderly favor the appearance of abnormal clones in the bone marrow of these individuals. Among the associated factors are: genomic mutations secondary to oxidative stress, inadequate production of cytokines, impairment of modulation and inappropriate response to physiological and external stimuli.16 Indeed, somatic mutations of some pre-leukemic genes (TET2, DNMT3A, ASXL1 and PPM1D) are strongly associated with clonal hematopoiesis in the elderly.17
The results of this study demonstrated a predominance of hematological malignancies, especially in elderly women (209 cases – 55.0%); one reason is that women live longer than men. Life expectancy for men at age 60 is 8.4 years and for women it is 9.1 years, and cancer-related death is also higher for men compared to women (207.9 per 100,000 men/145.4 per 100,000 women).18
Performing cytogenetic examinations repeatedly at different ages is essential in assessing the temporal origin and stability of genetic abnormalities.7 However, the literature, as well as the results presented in this study (Table 4), show that more patients perform exams once (81.0%) than on several occasions (19.0%). A cross-sectional study of 3100 over 19-year-old people in Pelotas, Brazil, showed that of 4167 medical consultations, 67.6% had only one set of exam results. Being female and old age were the most prevalent demographic factors in the examination request.19
Although this study demonstrates a higher frequency of normal karyotypes among the elderly, some studies point to an increase in the number of karyotypes with chromosomal abnormalities with aging. A study conducted by researchers at the National Cancer Institute (NCI) as well as the Gene Environment Association Study (GENEVA) linked to the National Institute of Health (NIH) show that chromosomal abnormalities related to aging, including genetic mosaicism, may predispose this group to the development of hematological cancers (leukemia, lymphoma, myeloma).7,20 The GENEVA study, which investigated blood samples from more than 50,000 participants with clonal mosaicism (duplications, deletions and uniparental disomy) in 404 patients, reported a frequency of clonal mosaicism of <0.5% in under 50-year-old subjects and of 2–3% among the elderly.7 The high frequency of chromosome abnormalities in old age may be associated with an increase in the number of cell divisions of lymphocytes and the number of somatic cells with mutations resulting from the progressive decline of the maintenance of genomic mechanisms in this phase of life.21–23
The results observed correlating hematological malignancies with patients’ age resemble other studies. According to the SEER Cancer Statistics Review, using data from 1975 to 2013, ALL is the most common neoplasm in children, adolescents and young adults and myelodysplastic syndrome is the most common disease in elderly people aged 60–69 years and 70–79 years. Contrary to the results presented, of the myeloproliferative neoplasms, CML is known to be diagnosed in the elderly population of 65–74 years, and AML in patients with a mean age of 67 years.24
With respect to AML, three hypotheses differentiate this neoplasm between the young and the elderly. In young people, it occurs due to the restricted number of mutational events limiting the diversity of subclones that are responsible for keeping cellular functions intact. In the elderly, mutational events cause multiple leukemic subclones with mechanisms of chemical resistance. The latter hypothesis states that the nature of the neoplasm is determined by the age of the hematopoietic stem cell.25
Some authors suggest that the number of mature cells produced by each hematopoietic stem cell declines with age.26 In fact, specific leukemia in the elderly is molecularly and functionally different from that found among young adults. Overexpression of Bcr-Abl in stem cells of the elderly alters the kinetics of the disease in a different way to overexpression in young stem cells.27 Therefore, failures in the ability of aged hematopoietic stem cells to respond appropriately to cell self-renovation and differentiation may predispose individuals to the appearance of hematological disorders.26
Research on cytogenetic and epidemiological etiology of hematological malignancies is scarce in the scientific literature and the presented results highlight the importance of studying patient profiles to gain knowledge of risk and genetic mechanisms related to these neoplasms. With the increase in life expectancy and consequently the elderly population worldwide, a substantial increase in multiple hematological cancers is expected in coming decades.26
ConclusionThe results suggest a high frequency of hematological malignancies among the elderly and a possible association of aging with the origin of cytogenetic alterations in respect to neoplasms. Errors in gene maintenance mechanisms and failures in the production of blood cells by hematopoiesis linked to deficiencies of the immune system of the elderly can lead to the formation of cells with mutations in genes favoring the appearance of chromosomal alterations and hematological malignancies.
Conflicts of interestThe authors declare no conflict of interest.
The authors would like to thank CAPES (Coordination for the Improvement of Higher Education Personnel), the staff of the Genetics Laboratory of the Blood Center for their collaboration in processing and analyzing samples: Jamile Lopes, Kênia Patrícia dos Santos do Carmo, Fernanda Miller and for the help in bureaucratic procedures: Cristielle Azevedo Santos. The Faculdade de Medicina de Marilia (FAMEMA) supported this research.


