

XIV Eurasian Hematology Oncology Congress
More infoFactor X deficiency (FXd) is a rare coagulation disorder that can be either hereditary or acquired.
Case reportWe characterized patients with FXd and evaluated their bleeding patterns and treatment strategies.
MethodologyThis retrospective review includes patients with FXd managed at Ege University Medical Faculty Hospital Ege Adult Hemophilia and Thrombosis Center.
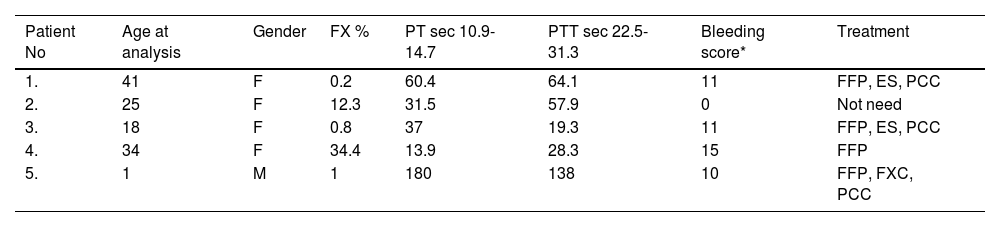
We analyzed demographic characteristics, laboratory results, bleeding scores, and treatments of five patients with FXd (Table).
Patient 1 was admitted for further evaluation of menometrorrhagia and prolonged postpartum bleeding. She required treatment following birth, tooth extraction, and fractional curettage during follow-up. Coagulation tests were run as a part of in vitro fertilization in patient 2 and were abnormal. Family history was significant for a history of thrombosis in her mother. Blood tests were positive for Prothrombin 20210 G/A heterozygous mutation and lupus anticoagulants. The patient has never had any bleeding episodes in the follow-up. Patient 3 has a history of menometrorrhagia, gingival bleeding, and prolonged bleeding after an abortion. The sister of the patient has FXd. In follow-up, she was treated for subcutaneous hematoma, gingival, and post-cesarean bleeding. Patient 4 presented for evaluation of menometrorrhagia. She was treated for polypectomy, two cesarean sections, tooth extraction, intermittent recurrent ecchymosis, and epistaxis. Patient 5 was diagnosed at age one and was referred to us for further management of his condition. His initial presentation was consistent with subdural hematoma. In the follow-up, he was treated for epistaxis, hematuria, subcutaneous hematoma, and gastrointestinal and gingival bleeding. He continues to take Factor X concentrate prophylactically. All the patients are currently healthy and regularly follow up in our center.
Results
ConclusionSince there is no FX concentrate in our country yet, FFP is used. Patients should be treated with the appropriate FX preparation and a prophylactic approach should be applied in necessary patients.
Table. Patient Characteristics and Diagnostic Laboratory Results
*- International Society for Thrombosis and Hemostasis/Scientific and Standardization Committee Bleeding Assessment Tool (ISTH-BAT), FFP- fresh frozen plasma, ES- erythrocyte suspension, PCC- prothrombin complex concentrate, FXC- Factor X concentrate, F-female, M-Male


