




The correct completion of the blood components request form is the starting point to ensure good transfusion care. Many guidelines have been developed to search for hemoglobin values that trigger the need for transfusion and show the importance of Patient Blood Management, a scientific evidence-based approach in processes where transfusion is a possibility, such as in elective surgeries.
ObjectiveThe cross-sectional study aimed to analyze the transfusion requests at a complex orthopedic hospital over a one-year period.
MethodThe completion quality was classified as Good, Regular, Bad or Very Bad, according to the information given by the physician. Transfusion medicine professionals analyzed the transfusion indication reported on the request form and classified it as Correct, Not based on Patient Blood Management (PBM), in accordance or not with the institutional Maximum Surgical Blood Order Schedule, Impossible to evaluate due to lack of information on the form, and Incorrect.
ResultsThe study categorized the completion quality of 2011 requests as Good (8.80%), Regular (9.30%), Bad (72.75%) and Very Bad (9.15%). Analysis of the indications revealed that 54.90% of the requests were in accordance with the current blood transfusion recommendations, and on 23.12% of the forms this field had not been filled out.
ConclusionThe majority of blood components (63%) requests are in tune with current blood transfusion recommendations, despite the great number of incorrectly completed forms; nevertheless, it is mandatory to reach much better appropriateness rates.
The blood components request is the starting point for the transfusion process, which should culminate in the transfusion of the requested blood components. The person in charge of receiving the blood orders must pay attention to adequacy and completeness, since any failure in fulfilling the request may seriously affect the transfusion process and patient safety. The fields related to the patient identification and location are very important; errors in patient identification may bring serious consequences. The requests must be made by a physician, on a specific form, which must be correctly filled in and legible, in order to ensure patient safety.1
Medical teams frequently neglect some items on blood orders.1,2 In many places, the requests are filled out without a more detailed evaluation; identifying the most prevalent failures in fulfillment is paramount for process improvement.
The Brazilian Transfusion Medicine Standards establish blood orders requirements,3 stating that requests should be made exclusively by physicians, on specific forms that must contain sufficient information regarding the applicant's identification, patient's identification and location, as well as their diagnosis, transfusion indication and relevant laboratory results.
In recent years, several studies have highlighted the importance of evaluating the blood transfusion indication itself. Many guidelines have been developed and updated to continuously search for hemoglobin and hematocrit values that trigger the need for blood components, as well as more correct transfusion indications.4 Transfusion audits and transfusion committees can decisively improve the patient standard of care (related to blood transfusion).5,6
Rational use of blood is a main concern. Blood is a raw material, whose source is limited, as its availability depends on volunteer blood donation, which is an expensive process as well. Even if the blood inventory is not an issue, liberal blood transfusion can increase the risks for patients.4
More liberal blood transfusion policies have lost ground to the so-called restrictive blood-use policy. A liberal blood-transfusion policy implies, for example, in transfusing patients at higher hemoglobin levels, such as 9–10g/dL. On the other hand, restrictive blood-use strategies use lower transfusion triggers, such as hemoglobin between 6 and 7g/dL. The results of the studies comparing these strategies indicate that there is no difference in mortality.7
In recent years, Patient Blood Management (PBM) strategies have being developed by many countries. They consist of a scientific evidence-based approach to determine correct transfusion indications.8 Three pillars should be addressed preoperatively, intraoperatively and postoperatively: optimization of erythropoiesis, reduction of blood loss, and perception of individual tolerance to anemia. For the correct management of blood use and greater patient safety, several segments must be involved.9
The PBM aims to collaborate with the rational use of blood in a hospital, through educational actions, evaluations of transfusion indications and discussion of clinical cases related to the use of blood components.10
In addition to the analysis of the quality of the completion of the request form and indication for transfusion, other information can be audited, such as the sectors most in need and the profile of the patients being transfused.11
The main objective of this study was to analyze the completion quality of blood components request forms. The blood order completeness and adequacy were analyzed, in a retrospective manner, verifying which items had been left blank or were filled out incorrectly.
Secondary objectives included the analysis of blood components indications and the profile of transfusion requests at an orthopedic hospital.
It is noteworthy that we did not analyze the acceptance or rejection of the blood transfusion indication.
MethodsThis cross-sectional study was conducted to discover the profile of blood components transfusion requests at a public reference hospital for highly complex orthopedic surgeries, from January 1, 2017 to December 31, 2017.
The following variables were analyzed on blood components request forms: patient identification, location at the hospital, gender, age, weight and diagnosis; transfusion indication, type of transfusion (non-urgent, urgent, extreme urgency, scheduled, surgical reserve), laboratory results (including date), type and amount of requested blood component, presence or absence of the prescribing physician identification and signature, date and time.
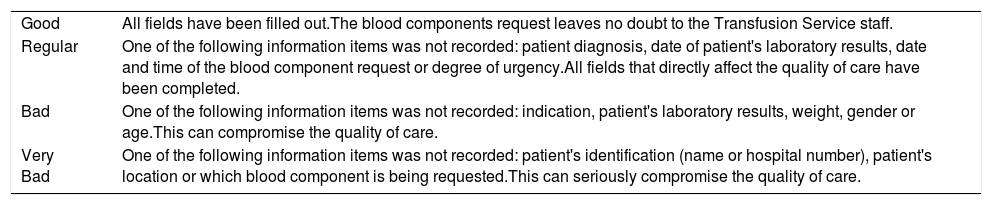
The completion quality was classified as Good, Regular, Bad or Very Bad. The classification is described in Table 1.
Classification of blood request: definitions.
| Good | All fields have been filled out.The blood components request leaves no doubt to the Transfusion Service staff. |
| Regular | One of the following information items was not recorded: patient diagnosis, date of patient's laboratory results, date and time of the blood component request or degree of urgency.All fields that directly affect the quality of care have been completed. |
| Bad | One of the following information items was not recorded: indication, patient's laboratory results, weight, gender or age.This can compromise the quality of care. |
| Very Bad | One of the following information items was not recorded: patient's identification (name or hospital number), patient's location or which blood component is being requested.This can seriously compromise the quality of care. |
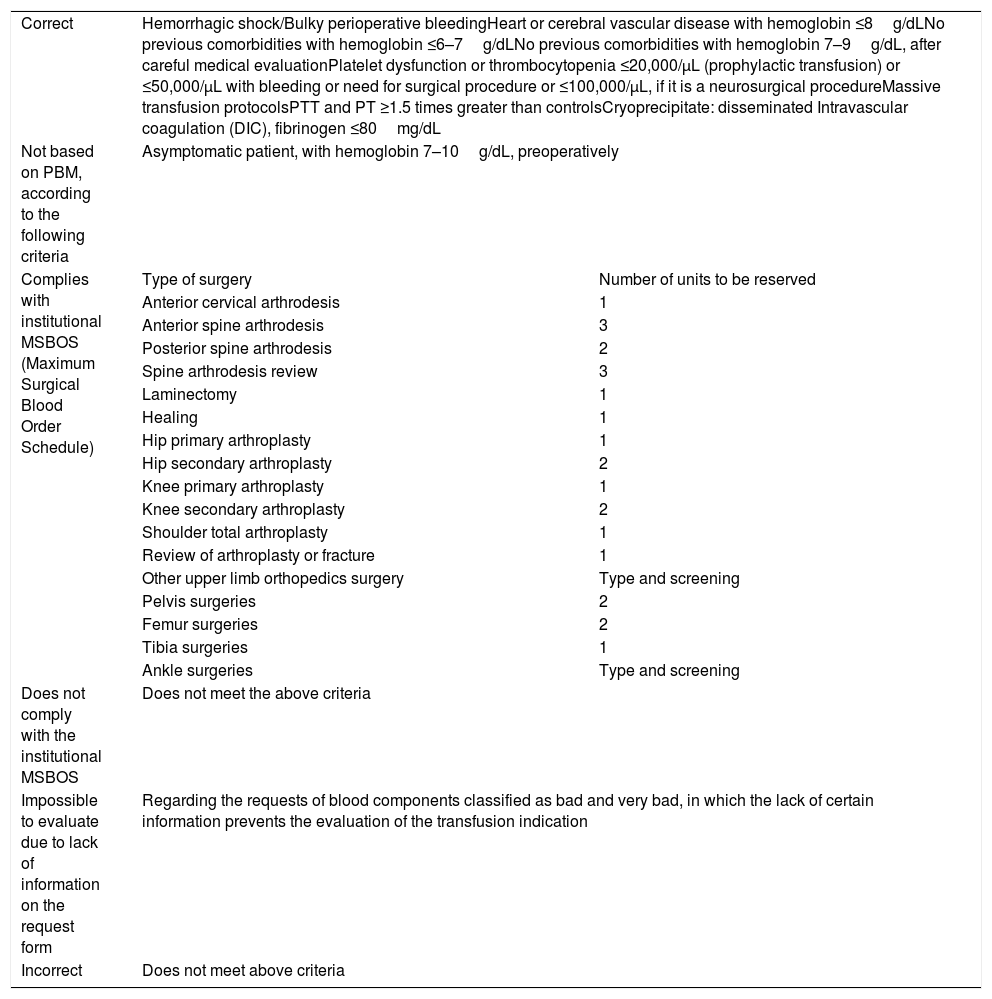
Transfusion medicine professionals retrospectively analyzed the transfusion indication on the blood order form and classified it as Correct, Non-PBM-based, according to the institutional Maximum Surgical Blood Order Schedule (MSBOS), Does not Comply with the institutional MSBOS, Impossible to evaluate due to lack of information on the form, and Incorrect. The classification described in Table 2 was created based on the pertinent medical literature.12–14
Classification of transfusion requests according to the quality of the completion.
| Correct | Hemorrhagic shock/Bulky perioperative bleedingHeart or cerebral vascular disease with hemoglobin ≤8g/dLNo previous comorbidities with hemoglobin ≤6–7g/dLNo previous comorbidities with hemoglobin 7–9g/dL, after careful medical evaluationPlatelet dysfunction or thrombocytopenia ≤20,000/μL (prophylactic transfusion) or ≤50,000/μL with bleeding or need for surgical procedure or ≤100,000/μL, if it is a neurosurgical procedureMassive transfusion protocolsPTT and PT ≥1.5 times greater than controlsCryoprecipitate: disseminated Intravascular coagulation (DIC), fibrinogen ≤80mg/dL | |
| Not based on PBM, according to the following criteria | Asymptomatic patient, with hemoglobin 7–10g/dL, preoperatively | |
| Complies with institutional MSBOS (Maximum Surgical Blood Order Schedule) | Type of surgery | Number of units to be reserved |
| Anterior cervical arthrodesis | 1 | |
| Anterior spine arthrodesis | 3 | |
| Posterior spine arthrodesis | 2 | |
| Spine arthrodesis review | 3 | |
| Laminectomy | 1 | |
| Healing | 1 | |
| Hip primary arthroplasty | 1 | |
| Hip secondary arthroplasty | 2 | |
| Knee primary arthroplasty | 1 | |
| Knee secondary arthroplasty | 2 | |
| Shoulder total arthroplasty | 1 | |
| Review of arthroplasty or fracture | 1 | |
| Other upper limb orthopedics surgery | Type and screening | |
| Pelvis surgeries | 2 | |
| Femur surgeries | 2 | |
| Tibia surgeries | 1 | |
| Ankle surgeries | Type and screening | |
| Does not comply with the institutional MSBOS | Does not meet the above criteria | |
| Impossible to evaluate due to lack of information on the request form | Regarding the requests of blood components classified as bad and very bad, in which the lack of certain information prevents the evaluation of the transfusion indication | |
| Incorrect | Does not meet above criteria | |
PTT=partial thromboplastin time
TP->PT
PT=prothrombin time
The indication for transfusion classified as correct leaves no doubt as to the patient's actual transfusion needs, such as transfusing red blood cells in patients with hemorrhagic shock. The non-PBM classification refers to situations traditionally accepted as a transfusion indication, such as transfusing a patient in the preoperative period with about 8.0–9.0g/dL hemoglobin, which PBM practices consider inadequate. The indications classified as incorrect are those that leave no doubt as to their inadequacy, such as transfusing red blood cells in patients with more than 10.0g/dL of hemoglobin or platelets in patients with more than 20,000platelets/μL who are not bleeding.
The institutional Maximum Surgical Blood Order Schedule was developed by the Hospital Transfusion Committee and is available in the hospital's internal computer system. Resident doctors who are recently engaged at the hospital also receive training in Transfusion Medicine.
The profile of blood components requests included patient gender, age and weight, number of requests made in 2017, prevalence by hospital sector and degree of urgency, frequency of blood component types requested, requests ordering more than one unit of packed red blood cells and finally, which were the most frequent indications.
The request for blood components made in the ward, surgical center or emergency room uses a printed form, manually filled out by the prescribing physician. The requests made at the Intensive Care Units use a software which automatically fills out some fields, such as patient name, hospital number, gender, age, location and date of the request. In this case, the prescriber just needs to fill out the remaining items, before printing the form.
It is noteworthy that any bad or very bad blood order completion imposes immediate actions, which generally entail the necessary contacting of the prescribing physicians, requesting that they correct or complete the form, or the on-call transfusion medicine physician, if the indications are thought to be inadequate, as these non-conformity requests are not allowed to be accepted.
In this study we did not address the question of how many requests were completely adjusted by the prescribers, we just audited the initial form arriving at the blood bank.
Statistical analysis was performed using the χ2 test for categorical variables of the EpiIinfo® 7th version software.
ResultsThere were 2011 blood components requests sent to the hospital transfusion service over the one-year period, which represented, on average, 153.69 requests per month.
Regarding the quality forms completion analysis, 8.80% were classified as Good, 9.30% as Regular, 72.75% as Bad and 9.15% as Very Bad (Figure 1). Considering only the forms coming from Intensive Care Units (ICUs), the ones partially filled out by the computer software, the study showed that 16.78% were classified as Good, 10.23% as Regular, 70.64% as Bad and only 2.35% as Very Bad. There was a reduction of very bad forms when they were partially filled out by the computer system (2.35% versus 12.01%), p<0.01.

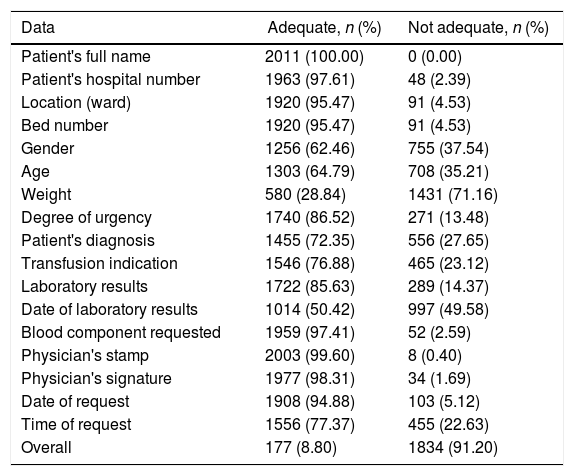
Among the forms classified as bad, the lack of weight information was the most frequent (87.42%) non-conformance, followed by lack of gender information (44.63%), age (41.97%), indication (28.16%) and laboratory results (16.68%). On 91.20% of the forms, more than one of those fields were not filled out. The overall assessment of completeness of all the information on the forms is found in Table 3.
Analysis of blood components request forms.
| Data | Adequate, n (%) | Not adequate, n (%) |
|---|---|---|
| Patient's full name | 2011 (100.00) | 0 (0.00) |
| Patient's hospital number | 1963 (97.61) | 48 (2.39) |
| Location (ward) | 1920 (95.47) | 91 (4.53) |
| Bed number | 1920 (95.47) | 91 (4.53) |
| Gender | 1256 (62.46) | 755 (37.54) |
| Age | 1303 (64.79) | 708 (35.21) |
| Weight | 580 (28.84) | 1431 (71.16) |
| Degree of urgency | 1740 (86.52) | 271 (13.48) |
| Patient's diagnosis | 1455 (72.35) | 556 (27.65) |
| Transfusion indication | 1546 (76.88) | 465 (23.12) |
| Laboratory results | 1722 (85.63) | 289 (14.37) |
| Date of laboratory results | 1014 (50.42) | 997 (49.58) |
| Blood component requested | 1959 (97.41) | 52 (2.59) |
| Physician's stamp | 2003 (99.60) | 8 (0.40) |
| Physician's signature | 1977 (98.31) | 34 (1.69) |
| Date of request | 1908 (94.88) | 103 (5.12) |
| Time of request | 1556 (77.37) | 455 (22.63) |
| Overall | 177 (8.80) | 1834 (91.20) |
Whether forms considered as bad or very bad were accepted was not analyzed. In the blood components request form there is no field to inform whether the transfusion was actually performed. The control of orders not accepted or not attended to, for example due to the temporary unavailability of blood components, was registered at another location.
Concerning the transfusion indications, 54.90% of the forms were classified as Correct, 20.34%, as Not based on the PBM, 8.11% of surgical reservations complied with the Institution protocol, 4.67% of surgical reservations were not in accordance with the Institution protocol, 9.50% were impossible to evaluate due to lack of information on the form and 2.49% were incorrect (Figure 2A).
 Classification of the blood components indication. (1) Correct; (2) Not based on PBM; (3) Complies with the institutional MSBOS; (4) Does not Comply with the institutional MSBOS; (5) Impossible to evaluate due to lack of information on the form; (6) Incorrect. (B) Profile of transfusion indications, according to prescription, described as: (1) Not Informed; (2) Anemia; (3) Perioperative excessive bleeding, Perioperative hemodynamic instability; (4) Acute or symptomatic anemia; (5) Informed the diagnosis instead of transfusion indication; (6) Surgical reserve; (7) Preoperative anemia, need to increase hematocrit for surgery; (8) Hypotension, Tachycardia, Cardiorespiratory arrest; (9) Bleeding/Anemia in the postoperative period; (10) Other: Delirium, pancytopenia, worsening of renal function, infection, denervation, replacement, sepsis, poor evolution in physiotherapy; (11) Anemia in a coronary patient, pneumothorax, patient with ventilator support; (12) Acute coagulopathy; (13) Bleeding at a non-surgical site: digestive hemorrhage, hemothorax, venous injury, arterial lesion.")
Transfusion indications on blood request forms. (A) Classification of the blood components indication. (1) Correct; (2) Not based on PBM; (3) Complies with the institutional MSBOS; (4) Does not Comply with the institutional MSBOS; (5) Impossible to evaluate due to lack of information on the form; (6) Incorrect. (B) Profile of transfusion indications, according to prescription, described as: (1) Not Informed; (2) Anemia; (3) Perioperative excessive bleeding, Perioperative hemodynamic instability; (4) Acute or symptomatic anemia; (5) Informed the diagnosis instead of transfusion indication; (6) Surgical reserve; (7) Preoperative anemia, need to increase hematocrit for surgery; (8) Hypotension, Tachycardia, Cardiorespiratory arrest; (9) Bleeding/Anemia in the postoperative period; (10) Other: Delirium, pancytopenia, worsening of renal function, infection, denervation, replacement, sepsis, poor evolution in physiotherapy; (11) Anemia in a coronary patient, pneumothorax, patient with ventilator support; (12) Acute coagulopathy; (13) Bleeding at a non-surgical site: digestive hemorrhage, hemothorax, venous injury, arterial lesion.
On 23.12% of the forms, the indication field was not filled out. Anemia was the most frequent indication, with 14.2%, followed by excessive bleeding in the perioperative period with hemodynamic repercussion (13.28%) and by the terms anemia/symptomatic anemia (11.83%). The authors analyzed possible variations in the indications filled out by the prescribing physicians and brought them together in the topics described in Figure 2B. For example, anemia associated with dizziness and anemia associated with tachycardia were classified as symptomatic anemia.
Nearly a quarter of the forms did not have the diagnostic or indication field filled out. There was also some confusion between diagnosis and indication.
The most requested blood component was Red Blood Cell Concentrates (RBC) (86.19%), as seen in Figure 3A. The hemoglobin value triggering RBC transfusion was less than or equal to 7.0g/dL in 24.73% of the cases (Figure 3B). The request for one or more RBCs in the same request is described in Figure 3C. The request for one unit of RBC, either for immediate transfusion (67.17%) or for elective surgery (55.51%), was more prevalent than the request for two or more.
 Prevalence of the blood components requests. (B) Hemoglobin values recorded on the blood components requests form. (C) Number of units of packed red blood cells requested per form.")
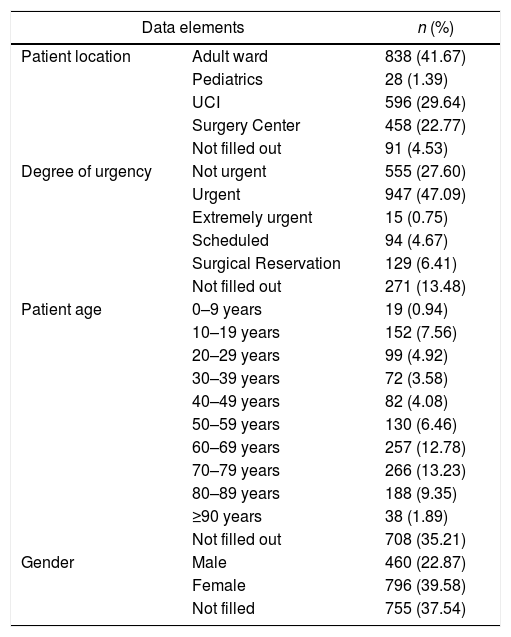
Another analysis of the blood components request profile at a predominantly orthopedic hospital is shown in Table 4.
Profile analysis of blood requests.
| Data elements | n (%) | |
|---|---|---|
| Patient location | Adult ward | 838 (41.67) |
| Pediatrics | 28 (1.39) | |
| UCI | 596 (29.64) | |
| Surgery Center | 458 (22.77) | |
| Not filled out | 91 (4.53) | |
| Degree of urgency | Not urgent | 555 (27.60) |
| Urgent | 947 (47.09) | |
| Extremely urgent | 15 (0.75) | |
| Scheduled | 94 (4.67) | |
| Surgical Reservation | 129 (6.41) | |
| Not filled out | 271 (13.48) | |
| Patient age | 0–9 years | 19 (0.94) |
| 10–19 years | 152 (7.56) | |
| 20–29 years | 99 (4.92) | |
| 30–39 years | 72 (3.58) | |
| 40–49 years | 82 (4.08) | |
| 50–59 years | 130 (6.46) | |
| 60–69 years | 257 (12.78) | |
| 70–79 years | 266 (13.23) | |
| 80–89 years | 188 (9.35) | |
| ≥90 years | 38 (1.89) | |
| Not filled out | 708 (35.21) | |
| Gender | Male | 460 (22.87) |
| Female | 796 (39.58) | |
| Not filled | 755 (37.54) | |
UCI=Intensive Care Unit
In all analyzed requests, the patient name was filled out, even though it was often replaced by a printed identification tag with patient information containing the patient's name and hospital number.
The adult ward (41.67%) was the most frequent location, followed by the ICU (29.64%). The type of transfusion classified as urgent, for transfusion within 3h after being requested, was the most prevalent (47.09%), followed by 27.60% of non-urgent transfusions (transfusion to be performed up to 24h upon the receipt of the request).
Regarding the gender, 39.58% of the patients were female, 22.87% were male and 37.54% had no gender identification on the requests. The non-completion was also high in the field age, reaching 35.21%. Most of the transfused patients were older than 60 years (37.25%).
On 96.6% of the forms, the requesting physician identification medical stamp was present and on 98.31%, his or her signature. Some doctors placed the signature in a field other than the indicated one, as for example, in the field for transfusion authorization, without the completion of compatibility tests.
DiscussionWe verified that 81.9% of request forms classified as bad or very bad, 9.3%, regular, and only 8.8%, good completion. Even if we assume regular classification as an acceptable one, the vast majority of blood requests does not fulfill any quality standard. We believe that most prescribing doctors still do not realize the importance of correctly filling out blood requests. These results are very different from the ones previously published, which teaches us that we need quick and effective interventions to change this situation. For example, a paper published by Quaranta et al., in France, showed that only 10% of blood requests at French hospitals did not inform the patient's diagnosis, versus 27.5% at our hospital. However, this French study also showed that many prescribers confounded diagnosis and transfusion indication, as we observed in our study.15 Therefore, there is considerable space for improvement in the medical education related to Transfusion Medicine at our hospital (and probably elsewhere). A similar multicentric study was conducted in Spain which aimed to evaluate the appropriateness of blood transfusion in emergency rooms and it found that only 21.4% of transfusion requests were adequate in terms of a transfusion indication.16 A study conducted in Alagoas, Brazil, published in 2013, found only 14.07% of appropriate transfusion in an emergency room.17
These figures are not nor very different from ours, showing that this is neither a negligible nor a local problem. An interesting strategy to help prescribers to comply with transfusion medicine regulations is the use of a computerized request form. The electronic prescription can improve the completion quality, since fields such as identification, laboratory results and date can be completed automatically.18
Moreover, the software can be configurated to block the on-line blood order transfer to the transfusion service if all the required fields are not correctly filled out. At our hospital, this system was implemented only for the ICU department. Consequently, the blood requests coming from ICU were better than the requests coming from all other hospital departments. This experience should be expanded to all the hospital departments, as soon as possible.
A recent Failure Mode and Evaluation Analysis (FMEA) applied to transfusion risks by a Hong Kong team showed that insufficient and/or incorrect clinical information on the request form was the fifth (out of 20 possible risks) most important risk in the blood transfusion process. The investigators implemented an electronic application form to replace the traditional paper form.19
A good aspect, probably reflecting the efforts of the transfusion service to disseminate one of the most important PBM guidelines – “transfuse one Red Blood Cell Concentrate (RBC), then re-evaluate the patient to assess if he or she needs a second RBC” – was the fact that the majority (60%) of blood order forms received just requested one unit of RBC. This result was in accordance with the Choosing Wisely initiative of the American Board of Internal Medicine Foundation, in partnership with the American Association of Blood Banks. One of their recommendations was not to transfuse more blood units than absolutely necessary.20
A second recommendation of this initiative suggests avoiding transfusion of an RBC for iron-deficiency patients without hemodynamic instability, especially in preoperative assessments. The large percentage of non-PBM indications may be due to patients with anemia prior to surgical hospitalization not being investigated and treated for possible iron deficiency.20
Regarding the quality assessment of transfusion triggers described on blood order forms, 63% could be considered as correct and PBM-based. This means that 37% of the requests did not correspond to a rational blood use. Moreover, 23.1% of the requests did not contain any information regarding a transfusion indication. This high prevalence of non-conformances indicates an immediate need for corrective and preventive actions; those measures must be undertaken by the transfusion service (training and education) and by the hospital transfusion committee. The indiscriminate use of surgical reservation may cause overloading for transfusion services and overexposure to tests. Transfusion committees should create tables with the maximum surgical blood ordering schedule (MSBOS) for the different types of surgery performed, based on literature data and the hospital experience. At our hospital, this MSBOS does exist and it can be accessed by any institutional computer; thanks to that, two-thirds of surgical reservations comply with our MSBOS, but again, we still need to improve, as it is totally feasible to attain zero non-conformance in this regard.
Since the MSBOS is approved by all our stakeholders, one possible intervention is to leave to the blood bank the decision about how many RBCs should be reserved, according to the specific patient's surgery.
Two recent studies have shown that blood transfusion in patients submitted to elective orthopedic surgeries was associated with an increased risk of infection, especially at the surgical site.21,22 Other studies highlight the increase in mortality among patients submitted to orthopedic surgeries who received a blood transfusion, mainly elderly patients.23,24
One of the limitations of this study was the non-observance of blood components requests that were not attended to by contraindication of the transfusion medicine professionals. Furthermore, the study did not evaluate the percentage of RBCs requested for surgical reserve that were actually used.
ConclusionThe analysis of 2011 requests for blood components made at a high-complexity orthopedic hospital in the year 2017 showed that 81.90% were classified in the Bad and Very Bad category. There is a large margin for improvement in form completion, which can be obtained through awareness campaigns directed at prescribing physicians, as well as the adoption of computerized systems for completing and issuing forms. A similar system is already employed in the ICU sector of the same hospital, with good results.
The majority of blood components (Correct and Complies with the institutional MSBOS – 63%) requests are in tune with current blood transfusion recommendations, despite the great number of incorrectly completed forms; nevertheless, it is mandatory to obtain much better appropriateness rates. Our study showed an urgent need for interventions focused on decreasing the rates of non-conformances in the blood order completion. Those interventions should include intensive educational and training actions, dissemination of PBM concepts and guidelines and, if possible, preemptive analysis of the adequacy of the indication before any blood component is issued for transfusion.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Conflicts of interestThe authors declare no conflicts of interest.
The authors thank Danilo Sarcinelli for his help in statistical analysis, graphs and language.


