
This study aimed to describe the incidence, microbiological profile, and risk factors associated with bacteremia in pediatric patients with hematopoietic stem cell transplantation (HSCT).
MethodsA retrospective cohort study was performed on patients under 18 years old who underwent HSCT due to any indication, between January 2012 and January 2017. The patient data were collected from the first 100 days post-HSCT. Bacteremia was defined as the isolation of bacteria from at least one blood culture. The relation between bacteremia and associated risk factors was evaluated using univariate and multivariate analysis.
ResultsWe enrolled a total of 111 pediatric patients who received HSCT during the period of study. The total number of patients who developed at least one episode of bacteremia was 46 (41.4%), and the total number of bacteremia episodes was 62. Rectal swabs were performed in 44 patients to detect prior colonization and this showed that 25% of them were positive, the main pathogen isolated being carbapenem-resistant enterobacteriaceae. The Gram-negative bacteria cases accounted for 60% of 62 events. The main Gram-negative bacteria isolated were Klebsiella pneumoniae and Escherichia coli and the majority were resistant strains. The mortality rate on day +100 for the whole cohort was 18% (n=20). Regarding the patients with bacteremia, the mortality rate on day +100 was 30% (n=14), and the cause of death was related to infection in 10 of them. We did not find any statistically significant risk factor for the development of bacteremia.
ConclusionBacteremia is common after HSCT, and there is a high frequency of resistant Gram-negative infections which is related to high mortality.
Hematopoietic stem cell transplantation (HSCT) is a potentially curative treatment for multiple malignant and non-malignant diseases. It has been in use for the past 50 years, and various aspects of the treatment have changed significantly over time, including the conditioning regimen, the source of stem cells and the general management strategies. Such evolution has reduced the morbidity and mortality rates associated with the procedure, which has led to an increase in the total number of patients undergoing HSCT every year. However, despite the advances achieved in this field, infections caused by viruses, fungi or bacteria are still frequent and associated with high mortality.1,2
Patients who have undergone HSCT are at a greater risk of presenting severe infections, with commensal and opportunistic microorganisms, caused by severe immunosuppression. The risk of bacterial infection in the post-transplant period depends on certain characteristics of the donor and the transplant. Transplantation from unrelated donors leads to a higher risk of infection than from related donors.3 Transplantation of umbilical cord cells is the most associated with infection, followed by bone marrow and peripheral blood.4 In pediatric patients, non-malignant pathologies are more related to bacterial infection than high-risk malignancies.5 Regarding the conditioning regimen used in the pre-transplant period, myeloablative conditioning is associated with higher rates of bacterial infection.6
Bacteremia is a frequent complication in the post-transplant period, with an estimated incidence of 20%–44% and a mortality rate between 10% and 50%, mainly related to resistant microorganisms.7–9 The diagnosis of infection after HSCT is a challenge, due to the complexity and the critical state of the patients, and because the signs and symptoms present in these patients are mostly non-specific. Early detection and treatment are essential in the reduction of morbidity and mortality.10 Bacteremia is the most common presentation of infection in patients treated by HSCT, increasing mortality rates and prolonging hospital stays.9 The Fundación Valle del Lili hospital is a reference health center in Colombia, which has performed an average of 20 transplants per year in pediatric patients since 2008. The aim of this study was to describe the incidence, microbiological profile and risk factors associated with bacteremia in pediatric patients treated with HSCT.
MethodsStudy subjects and designA retrospective study was conducted on patients aged <18 years who had undergone HSCT for any indication between January 2012 and January 2017. The patient data were collected for the first 100 days post-HSCT. This study was approved by the Fundación Valle del Lili Institutional Review Board Ethics Committee.
DefinitionsBacteremia was defined as the isolation of bacteria from at least one blood culture. For bacteria that colonize the skin, positive results from two consecutive blood cultures were required. All bacteremia cases occurring between the beginning of the conditioning regimen and +100 days were evaluated. Primary bacteremia was defined as a bloodstream infection confirmed by a laboratory result that was not secondary to an infection at another body site. Secondary bacteremia was defined as an infection thought to be seeded from a site-specific infection in another body site. Bacteremia was considered catheter-related when the causative agent isolated in the blood was also recovered from a catheter hub or tip.11
Prior antibiotic therapy was defined as the receipt of any systemic antibiotic for >48h during the month prior to the conditioning regimen. In the case of fever or other signs or symptoms of infection, prophylactic antibiotics were interrupted, and the patients were treated with broad-spectrum intravenous antibiotics. However, this treatment was modified according to the susceptibility of the isolated bacteria.
The antimicrobial susceptibilities of the isolations were interpreted according to current Clinical Laboratory Standard Institute (CLSI) criteria.12 Screening for multidrug-resistant organisms was performed with rectal and nasal swabs prior to the administration of the conditioning regimen, in search of phenotypes that included methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococci, extended-spectrum β-lactamase production and carbapenemase production. Since 2014, surveillance cultures have been routinely obtained prior to HSCT at our institution.
The conditioning regimen and graft-versus-host disease (GvHD) prophylactic approach varied according to the diagnosis and type of transplantation. Conditioning regimens were classified according to their intensity as myeloablative and non-myeloablative.13 Acute and chronic GvHD were defined according to standard criteria.14 The patients received ciprofloxacin (20–30mg/kg/day, max. 500mg) as antimicrobial prophylaxis, fluconazole (5mg/kg/day, max. 400mg) or voriconazole (4mg/kg/day, max. 200mg) as antifungal prophylaxis and acyclovir (1500mg/m2/day) as antiviral prophylaxis, which continued until the engraftment. Following engraftment, the patients received prophylaxis for Pneumocystis jiroveci and Toxoplasma gondii with trimethoprim–sulfamethoxazole (5mg/kg/day three times per week). Mucositis was evaluated according to the World Health Organization criteria.15
Statistical analysisThe categorical variables were summarized in proportions, and the continuous variables were expressed as median and interquartile range (IQR). The p value was calculated using the chi-square test, Fisher’s exact test or the Mann–Whitney test, as appropriate. The data were stratified according to the type of HSCT and the presence or absence of bacteremia.
Clinically significant variables or those with p<0.20 in the univariate analysis were included in a multivariate Cox regression analysis, which yielded hazard rates (HR) and confidence intervals (CI). Because some subjects had more than one episode of bacteremia, only the first event was used for this analysis. Values of p<0.05 were considered statistically significant. All statistical analyses were performed using the statistical software package STATA 12.
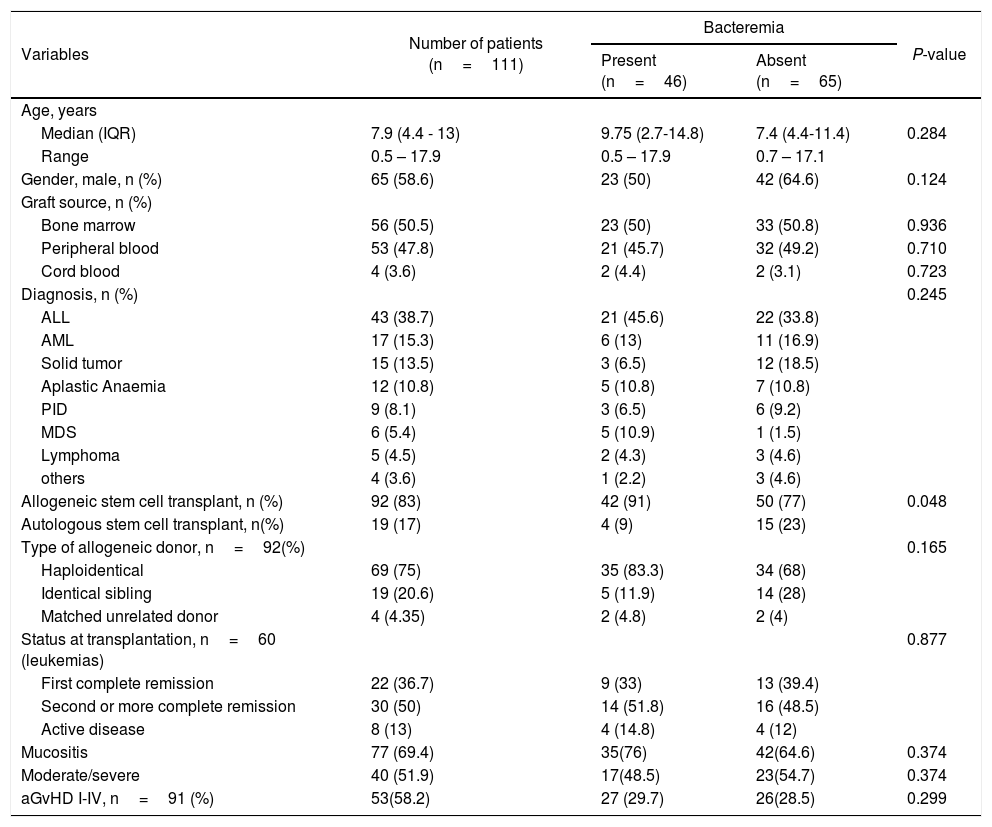
ResultsWe enrolled a total of 111 pediatric patients who received HSCT over the course of the study. The total number of patients who developed at least one episode of bacteremia was 46 (41.4%). The total number of bacteremia episodes was 62. The patient and transplant features are outlined in Table 1. Primary bacteremia was present in 63% (n=29) of the patients, and the secondary form was present in 36% (n=17) of the patients. The median age of the patients who received HSCT was 7.9 years (IQR 4.4–13). Most patients were male (58.6%) and were affected by acute lymphoblastic leukemia (38.7%). Other underlying diseases were myeloid leukemia (15.3%), solid tumors (13.5%), aplastic anemia (10.8%), followed by primary immunodeficiency, myelodysplastic syndrome and lymphoma. Allogeneic and autologous HSCT were performed in 83% and 17% of the patients, respectively, and the allogeneic donor types were: haploidentical, identical sibling or matched unrelated donor. Half of the infected patients presented moderate to severe mucositis and 30% presented acute graft vs. host disease (aGvHD).
Characteristics of patients with and without bacteremia.
| Variables | Number of patients (n=111) | Bacteremia | P-value | |
|---|---|---|---|---|
| Present (n=46) | Absent (n=65) | |||
| Age, years | ||||
| Median (IQR) | 7.9 (4.4 - 13) | 9.75 (2.7-14.8) | 7.4 (4.4-11.4) | 0.284 |
| Range | 0.5 – 17.9 | 0.5 – 17.9 | 0.7 – 17.1 | |
| Gender, male, n (%) | 65 (58.6) | 23 (50) | 42 (64.6) | 0.124 |
| Graft source, n (%) | ||||
| Bone marrow | 56 (50.5) | 23 (50) | 33 (50.8) | 0.936 |
| Peripheral blood | 53 (47.8) | 21 (45.7) | 32 (49.2) | 0.710 |
| Cord blood | 4 (3.6) | 2 (4.4) | 2 (3.1) | 0.723 |
| Diagnosis, n (%) | 0.245 | |||
| ALL | 43 (38.7) | 21 (45.6) | 22 (33.8) | |
| AML | 17 (15.3) | 6 (13) | 11 (16.9) | |
| Solid tumor | 15 (13.5) | 3 (6.5) | 12 (18.5) | |
| Aplastic Anaemia | 12 (10.8) | 5 (10.8) | 7 (10.8) | |
| PID | 9 (8.1) | 3 (6.5) | 6 (9.2) | |
| MDS | 6 (5.4) | 5 (10.9) | 1 (1.5) | |
| Lymphoma | 5 (4.5) | 2 (4.3) | 3 (4.6) | |
| others | 4 (3.6) | 1 (2.2) | 3 (4.6) | |
| Allogeneic stem cell transplant, n (%) | 92 (83) | 42 (91) | 50 (77) | 0.048 |
| Autologous stem cell transplant, n(%) | 19 (17) | 4 (9) | 15 (23) | |
| Type of allogeneic donor, n=92(%) | 0.165 | |||
| Haploidentical | 69 (75) | 35 (83.3) | 34 (68) | |
| Identical sibling | 19 (20.6) | 5 (11.9) | 14 (28) | |
| Matched unrelated donor | 4 (4.35) | 2 (4.8) | 2 (4) | |
| Status at transplantation, n=60 (leukemias) | 0.877 | |||
| First complete remission | 22 (36.7) | 9 (33) | 13 (39.4) | |
| Second or more complete remission | 30 (50) | 14 (51.8) | 16 (48.5) | |
| Active disease | 8 (13) | 4 (14.8) | 4 (12) | |
| Mucositis | 77 (69.4) | 35(76) | 42(64.6) | 0.374 |
| Moderate/severe | 40 (51.9) | 17(48.5) | 23(54.7) | 0.374 |
| aGvHD I-IV, n=91 (%) | 53(58.2) | 27 (29.7) | 26(28.5) | 0.299 |
aGvHD, acute graft-versus-host disease; ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; IQR, interquartile range; MDS, myelodysplastic syndrome; PID, primary immunodeficiency diseases.
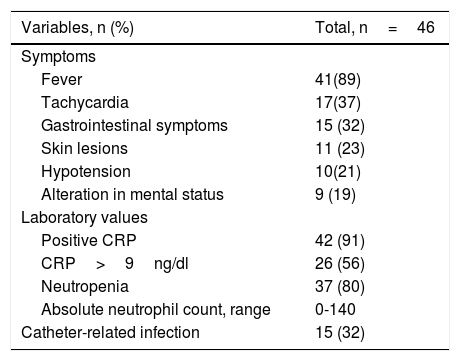
Table 2 lists the symptoms and laboratory values for the first bacteremia, for which blood cultures were performed the same day. The primary infection sign was fever, which was present in 89% (n=41) of the subjects. Most patients presented positive C-Reactive protein (CRP) (91%, n=42) at the time of diagnosis. Neutropenia was present in 80% (n=37) of the patients, with an absolute neutrophil count in the range of 0–140/mm3. Furthermore, 15 (32%) of the bacteremic episodes were catheter-related infections.
Clinical characteristics of the first bacteremia episode.
| Variables, n (%) | Total, n=46 |
|---|---|
| Symptoms | |
| Fever | 41(89) |
| Tachycardia | 17(37) |
| Gastrointestinal symptoms | 15 (32) |
| Skin lesions | 11 (23) |
| Hypotension | 10(21) |
| Alteration in mental status | 9 (19) |
| Laboratory values | |
| Positive CRP | 42 (91) |
| CRP>9ng/dl | 26 (56) |
| Neutropenia | 37 (80) |
| Absolute neutrophil count, range | 0-140 |
| Catheter-related infection | 15 (32) |
CRP: C-reactive protein.
Rectal swabs were obtained from 44 patients to detect prior colonization, 25% of which were positive. The main pathogens were carbapenem-resistant Enterobacteriaceae (n=9). Nasal swabs were obtained from 45 patients, but none were positive. Furthermore, 4 of the patients with bacteremia had previous positive swabs. However, 2 patients had bacteremia due to another type of bacteria (Streptococcus mitis). The other 2 patients had bacteraemia caused by the same colonization pathogen (carbapenem-resistant Klebsiella pneumoniae and extended spectrum beta-lactamase (ESBL)-producing Escherichia coli).
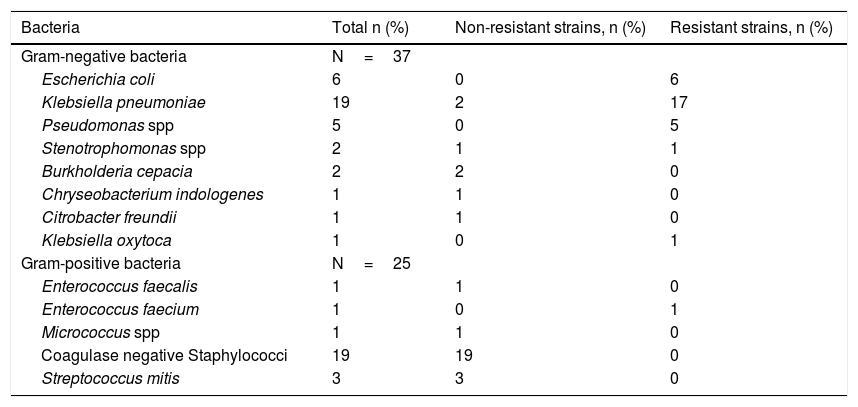
The organisms isolated in the blood cultures of patients with bacteraemia are summarized in Table 3. A total of 62 cultures were evaluated, in which the main gram-negative bacteria isolated was K. pneumoniae (51%, n=19), 90% of which were resistant strains, 14, carbapenem-resistant and 3, ESBL-producing strains. The second most common gram-negative bacteria isolated was E. coli (16%, n=6), of which all strains were ESBL-producing. All Pseudomonas spp. isolated from the bloodstream were resistant, with 1 being classified as multi-drug resistant (MDR) and 4 as carbapenem-resistant. Gram-positive bacteria were isolated from 25 of the blood cultures, all of which were vancomycin-sensitive. Coagulase-negative staphylococci was the most common bacteria in this group (76%, n=19).
Microorganisms causing bacteremia.
| Bacteria | Total n (%) | Non-resistant strains, n (%) | Resistant strains, n (%) |
|---|---|---|---|
| Gram-negative bacteria | N=37 | ||
| Escherichia coli | 6 | 0 | 6 |
| Klebsiella pneumoniae | 19 | 2 | 17 |
| Pseudomonas spp | 5 | 0 | 5 |
| Stenotrophomonas spp | 2 | 1 | 1 |
| Burkholderia cepacia | 2 | 2 | 0 |
| Chryseobacterium indologenes | 1 | 1 | 0 |
| Citrobacter freundii | 1 | 1 | 0 |
| Klebsiella oxytoca | 1 | 0 | 1 |
| Gram-positive bacteria | N=25 | ||
| Enterococcus faecalis | 1 | 1 | 0 |
| Enterococcus faecium | 1 | 0 | 1 |
| Micrococcus spp | 1 | 1 | 0 |
| Coagulase negative Staphylococci | 19 | 19 | 0 |
| Streptococcus mitis | 3 | 3 | 0 |
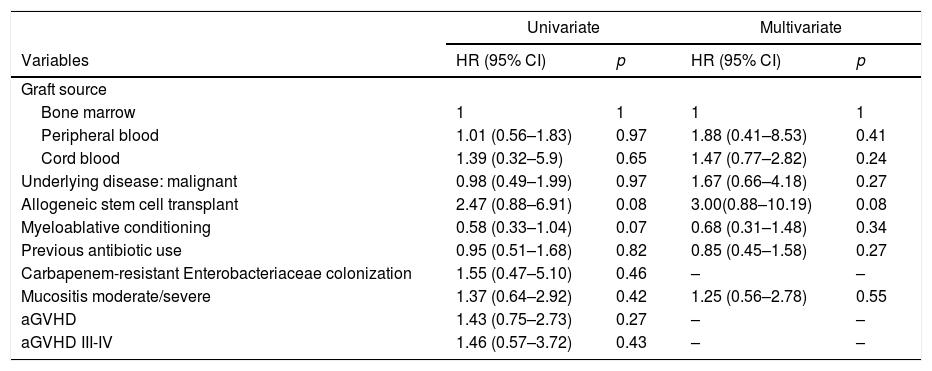
The bacteraemia-associated risk factors were evaluated in all patients and univariate and multivariate analyses were performed. Some HSCT characteristics such as graft source, underlying malignant disease (HR=0.98; CI=0.49–1.99), allogeneic stem cell transplant (HR=2.47; CI=0.88–6.91) and myeloablative conditioning (HR=0.58; CI=0.33–1.04) were studied. The infectious medical histories of patients, such as previous antibiotic use (HR=0.95; CI=0.51–1.68) and colonization with resistant bacteria (HR=1.55; CI=0.47–5.1), were analyzed. The HSCT complications, such as mucositis and aGvHD, were also included, but none were statistically significant risk factors for bacteraemia (Table 4).
Risk factors associated with first bacteremia episode.
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p | HR (95% CI) | p |
| Graft source | ||||
| Bone marrow | 1 | 1 | 1 | 1 |
| Peripheral blood | 1.01 (0.56–1.83) | 0.97 | 1.88 (0.41–8.53) | 0.41 |
| Cord blood | 1.39 (0.32–5.9) | 0.65 | 1.47 (0.77–2.82) | 0.24 |
| Underlying disease: malignant | 0.98 (0.49–1.99) | 0.97 | 1.67 (0.66–4.18) | 0.27 |
| Allogeneic stem cell transplant | 2.47 (0.88–6.91) | 0.08 | 3.00(0.88–10.19) | 0.08 |
| Myeloablative conditioning | 0.58 (0.33–1.04) | 0.07 | 0.68 (0.31–1.48) | 0.34 |
| Previous antibiotic use | 0.95 (0.51–1.68) | 0.82 | 0.85 (0.45–1.58) | 0.27 |
| Carbapenem-resistant Enterobacteriaceae colonization | 1.55 (0.47–5.10) | 0.46 | – | – |
| Mucositis moderate/severe | 1.37 (0.64–2.92) | 0.42 | 1.25 (0.56–2.78) | 0.55 |
| aGVHD | 1.43 (0.75–2.73) | 0.27 | – | – |
| aGVHD III-IV | 1.46 (0.57–3.72) | 0.43 | – | – |
aGvHD: Acute graft-versus-host disease.
The mortality rate on day +100 for the whole cohort was 18% (n=20). The etiologies of these deaths were: infection (13 patients), relapse (2 patients), GvHD (2 patients), major bleeding (1 patient) and multi-organ failure (2 patients). The mortality rate on day +100 in the group presenting bacteremia was 30% (14 patients) and the cause of death in 9 patients was related to bacteremia. The isolated bacteria that produced bacteremia and death were 4 cases of carbapenem-resistant K. pneumoniae, 3 cases of carbapenem-resistant P. aeruginosa, 1 case of ESBL-producing E. coli and 1 case of vancomycin-resistant Enterococcus faecium.
DiscussionThis study shows an overall bacteremia incidence of 41% during the first 100 days following HSCT. Most isolations resulted in resistant Gram-negative bacilli, and we did not find any associated risk factors.
Our incidence rate is similar to that of studies involving heterogeneous populations for whom rates ranging from 15% to 41% were reported. In European studies, the incidence rate reported has been 20%–39%,16–18 whereas Asiatic and some Latin American countries have reported much lower figures (15%–23%).19–23 A study in the United States found an incidence rate very similar to that found in our population.24 These differences could be explained, to some extent, by differences in supportive care, antibiotic prophylaxis, prior colonization, healthcare protocols, such as catheter maintenance and differences in follow-up timing. This study only characterized bacteremia occurring in the first 100 days after transplantation, which includes significant risk of bacterial and catheter-related infections.10
Colonization with resistant bacteria has been identified as an important risk factor for developing infections and is associated with a high mortality rate.25 Nasal and rectal swabs were only obtained for 39% of our patients, as swabbing only began to be routinely performed in 2014. As demonstrated in other studies, the most important pathogens causing colonization were carbapenem-resistant Enterobacteriaceae. These pathogens have been associated with severe infections in patients undergoing stem cell transplantation, with a reported mortality rate of up to 60%.26–28 Half of the patients previously colonized presented bacteremia with the same pathogens, demonstrating the importance of routine swabs in patients undergoing HSCT, to facility at early directed antimicrobial therapy.29
The predominant bacteremia-causing organisms in this population were Gram-negative resistant bacilli. These findings can be explained by the antibacterial prophylaxis used. In most European registries,16,24,30,31 both adults and children show a high prevalence of Gram-positive bacteria, whereas in Latin American records, Gram-negative bacteria predominate.23 The prophylaxis with quinolones may have been responsible for the high incidence of resistant Gram-negative bacilli. Rangar et al. found that fluoroquinolone use was significantly associated with the emergence of methicillin-resistant S. aureus (p=0.04), MDR E. coli (p<.001) and MDR P. aeruginosa (p=0.05).32 Garnica M et al. found that the rate of ESBL-producing Enterobacteriaceae was slightly higher in patients receiving quinolone prophylaxis (1.27 vs. 0.38 per 1000 patient-days, p= 0.26).33,34 These data suggest that probably the use of ciprofloxacin at our hospital was associated with the increased isolation of resistant Gram-negative bacilli.
The principal symptom of infection in our patients was fever, which occurred in 89% of the cases. This frequency is comparable to previous studies showing that almost all pediatric HSCT recipients developed fever.35 Although fever is not specific to infection, body temperature must be strictly evaluated in these patients. A total of 91% of the patients with bacteremia had a positive CRP the day the symptoms began. It has been demonstrated that CRP elevation is associated with bacterial infection.36,37 Some studies have demonstrated a high CRP specificity value >9mg/dL for detecting invasive bacterial infections.37,38 In our study, only half of the patients had a CRP >9mg/dL. The CRP is an important laboratory test for the early detection of bacteremia and an elevated value in an immunocompromised patient should alert physicians of a possible invasive bacterial infection.
In the risk factor analysis, none of them was related to bacteremia. For Allison M. Bock et al., allogeneic transplantation, myeloablative conditioning and development of aGvHD were identified as risk factors for bacteremia.25 Although Garnica et al. only evaluated the risk factors for Gram-negative bacteremia, they did not identify any statistically significant variable related to bacteremia.34
Most of the transplants performed at our Institution were T cell-replete unmanipulated haploidentical bone marrow with high-dose post-transplantation cyclophosphamide, a strategy which may provide a choice for patients without an HLA-matched sibling donor. In our country, volunteer donor registries do not exist and the cord blood transplant is expensive. The haploidentical transplant was an independent factor associated with bacteremia, compared to identical donor transplants.39,40 However, in the risk analysis for our cohort, this variable was not statistically significant.
The development of bacteremia in patients undergoing HSCT was related to increased mortality, and in our cohort, the mortality rate on day +100 was 18%, the majority of which was related to infection. The mortality rate could be related to the high proportion of resistant bacteria isolated in our patients. Oliveira et al., found that the mortality in their hospital was similar to ours, and the mortality rate among patients infected with Gram-negative MDR bacteria was higher, compared to that of other patients.41
Several limitations should be considered when interpreting our data. These include a retrospective design and a single-institution setting, coupled with the change in the susceptibility test of microorganisms across time. Furthermore, we consider that not having the results of swabs for all patients limits the analysis of the impact of resistant microorganisms.
ConclusionThe results of this study indicate that the incidence of bacteremia in the first 100 days following the HSCT is high in the pediatric population, but we did not find any associated risk factor. The most relevant finding was that many infections were caused by resistant bacteria. Therefore, it is important to be cautious when choosing the most appropriate empirical therapy and to base it on the institution-specific antimicrobial profile.
Conflicts of interestThe authors declare no conflicts of interest.



