
We received a blood grouping request for a 25-year-old primigravida diagnosed with ruptured ectopic pregnancy. She had no previous history of transfusion. Blood grouping was done by the tube technique and column agglutination technology (Diaclon ABO/D+ Reverse grouping, BioRad, Cressier, Switzerland). Forward grouping showed no agglutination with anti-A, anti-B and anti-A,B (Monoclonal antisera, Tulip Diagnostics, Goa, India) and 4+ agglutination was seen with anti-D (Monoclonal antisera, Tulip Diagnostics, Goa, India). Cell grouping was O RhD positive and serum grouping was AB group (Table 1). Tube grouping results were further confirmed by gel technology. Thus, a blood group discrepancy was observed as the results of cell grouping and serum grouping were discordant. The patient's red cells were evaluated for the presence of the H antigen using commercial anti-H lectin (Tulip Diagnostics, Goa, India) and serum from a Bombay phenotype individual (in-house). The H antigen was not detected on patient's red cells. Further tests were performed to detect weak antigens and antibodies. When the tubes were incubated at 4°C, there was no variation in the grade of agglutination with the cell grouping whereas the serum grouping tubes showed grade 1+ agglutination. Adsorption of patient's red cells with polyclonal antisera anti-A and anti-B at 4°C and elution of the antibodies at 56°C were performed to sense trace amounts of A and B antigens, respectively. Eluate was non-reactive with A cells and B cells, showing that there were no A and B antigens on patient's red cells. Furthermore, a saliva secretor test using hemagglutination inhibition was performed as described in the American Association of Blood Banks (AABB) technical manual, 17th edition.1 She was a secretor of ABH substances in saliva. A red cell antibody screen using a commercial three-cell panel was negative.
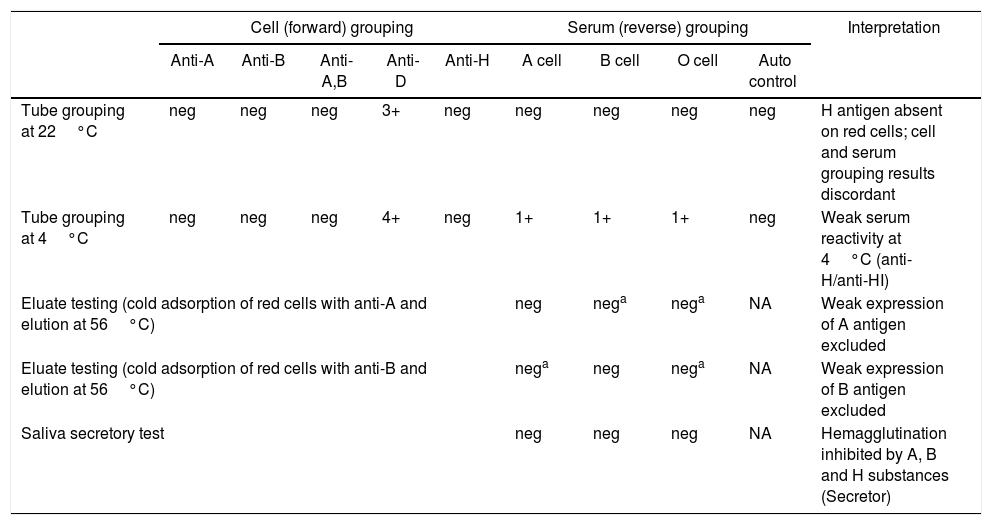
Results of serological investigations performed and their interpretation.
| Cell (forward) grouping | Serum (reverse) grouping | Interpretation | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Anti-A | Anti-B | Anti-A,B | Anti-D | Anti-H | A cell | B cell | O cell | Auto control | ||
| Tube grouping at 22°C | neg | neg | neg | 3+ | neg | neg | neg | neg | neg | H antigen absent on red cells; cell and serum grouping results discordant |
| Tube grouping at 4°C | neg | neg | neg | 4+ | neg | 1+ | 1+ | 1+ | neg | Weak serum reactivity at 4°C (anti-H/anti-HI) |
| Eluate testing (cold adsorption of red cells with anti-A and elution at 56°C) | neg | nega | nega | NA | Weak expression of A antigen excluded | |||||
| Eluate testing (cold adsorption of red cells with anti-B and elution at 56°C) | nega | neg | nega | NA | Weak expression of B antigen excluded | |||||
| Saliva secretory test | neg | neg | neg | NA | Hemagglutination inhibited by A, B and H substances (Secretor) | |||||
neg: negative; NA: not applicable.
a Control cells for adsorption and elution.
She had no H antigen on red cells but secreted A, B and H substances in saliva. Based on these observations, her blood group was found to be AB para-Bombay phenotype (ABh – secretor). The specificity of the antibodies in the patient's serum is likely to be anti-HI (reacting at 4°C only), as the serum did not react with group O cord cells (cord cells lack I antigen but carry H antigen) and was not inhibited by group O secretor saliva (anti-H would be inhibited by H substance).2 Her biological sister's blood group was A1B RhD positive.
The H antigen is synthesized by α-(1,2)-fucosyltransferases encoded by two distinct but closely linked genes, FUT1 and FUT2. H antigen expression on red cells is dependent on FUT1 (the H gene). The FUT2 gene (Secretor gene) is responsible for the formation of the H antigen in secretions (salivary glands) and gastrointestinal/genitourinary tissues. Bombay and para-Bombay phenotypes arise due to the homozygous inheritance of non-functional FUT1 genes (hh allele). The two entities are distinguished by the presence or absence of the FUT2/Secretor gene. Bombay phenotype individuals are red cell H deficient non-secretors (hh, se/se), while para-Bombay individuals are red cell H-deficient secretors (hh, Se/Se or Se/se).3 Para-Bombay individuals may occasionally have A and B antigens on red cells due to passive adsorption of A and B blood group substances from plasma.4 Based on previous studies, the incidence of the Bombay phenotype in our population ranges from 1:2500 to 1:13,000.5 When compared to the Bombay phenotype, the para-Bombay phenotype is more infrequent, occurring in a ratio of 1:15.6 However, the exact incidence of para-Bombay phenotype is not known in our population. The incidence of the para-Bombay phenotype in the Chinese population has been documented to be 1:12,000.2
Para-Bombay individuals can develop anti-H, anti-HI or both in addition to naturally occurring anti-A/anti-B. These antibodies have a wide thermal amplitude reacting at 4°C, 22°C and 37°C (predominantly at 4°C and 22°C).2,4 These individuals should be transfused with Bombay or para-Bombay blood if allo-anti-H or anti-HI in their serum is clinically significant (i.e., reacting at 37°C). It is also evident that anti-HI is clinically insignificant. For patients with anti-H/anti-HI reacting at lower temperatures (4°C-22°C), in case of non-availability of the para-Bombay blood group, AHG compatible units of ABO blood groups can be transfused.7 In our patient, the anti-HI reacted weakly at 4°C only. One unit of A1B RhD positive packed red cells was cross-matched for this patient using LISS/Coombs gel card and found compatible, although she did not require a transfusion during this admission. In addition, this rare phenotype demands attention with respect to solid organ transplantation. Since the secretor gene is active in these individuals, salivary glands, gastrointestinal and genitourinary tissues would still express ABH antigens despite the antigens being absent on red cells. Townamchai et al. reported a case of successful ABO-incompatible renal transplantation in a group O recipient who underwent pre-transplant desensitization as the donor's blood group had the AB para-Bombay phenotype.8 Para-Bombay phenotype and its variants would be explored further in the event of performing a simple saliva secretor test, in addition to the use of anti-H lectin in blood grouping. Hence, it should be borne in mind that thorough analysis of any blood group discrepancy is warranted as it has significant clinical implications.
Conflicts of interestThe author declares no conflicts of interest.
I sincerely thank Lab Technologists Ms. Tamilselvi, Ms. Alli and Ms. Sivakami for performing the technical aspects involved in this study.



