
Coronavirus Disease 2019 (COVID-19) is a novel viral disease with person-to-person transmission that has spread to many countries since the end of 2019. Although many unknowns were resolved within a year and the vaccine is available, it is still a major global health problem.
ObjectiveCOVID-19 infection may present with a considerably wide spectrum of severity and host factors play a significant role in determining the course of the disease. One of these factors is blood groups. Based on previous experience, it is believed that the ABO blood group type affects prognosis, treatment response and length of stay in the hospital. In this study, our aim was to evaluate whether the blood group had an effect on the length of the hospital stay. To the best of our knowledge, no previous studies have assessed the effect of ABO blood groups, as well as age, on the length of the hospital stay in these settings.
MethodsIn this retrospective cohort study, 969 patients admitted to our hospital between March 15, 2020 and May 15, 2020 were evaluated. The patients were divided into 4 groups according to ABO blood groups. The effect of the ABO blood group by age on the course of the disease, need for intensive care, duration of hospitalization and mortality in patients with COVID-19 infection, especially in geriatric patients, was evaluated.
ResultsOf all the patients, 9.1% required admission to the intensive care unit (ICU), of whom 83% died. The average length of ICU stay was 11 days (0 - 59). The observed mortality rates in blood groups A, B, AB and 0 were 86.4%, 93.3%, 80.0% and 70.8%, respectively, indicating similar death rates in all ABO blood types. When the Rh phenotype was taken into consideration, no significant changes in results were seen.
ConclusionAs a result, we could not observe a significant relationship between blood groups and clinical outcomes in this study, which included a sample of Turkish patients with COVID-19.
The new coronavirus disease that started in Wuhan, China in December 2019 has rapidly become a pandemic that remains a major global health problem despite the scientific efforts to provide effective treatments. The COVID-19 infection may present with a considerably wide spectrum of severity and host factors play a significant role in determining the course of the disease.
While most patients have an asymptomatic or mild disease, older patients or those with comorbid conditions such as diabetes, hypertension, chronic lung disease, cardiac disorders or malignancy are known to have a more unfavorable disease course.1 In addition to comorbid conditions and host-related thrombo-inflammatory responses, genetic factors, such as the ABO blood group, are also believed to affect the prognosis, treatment response and length of hospital stay. A close link between blood groups and the predisposition to infectious disease has been previously described in H. pylori, Plasmodium falciparum, HBV, SARS-COV and MERS-COV.2-6 Again, while some investigators reported a significant correlation between the ABO type and acquisition, prognosis and mortality of the SARS-CoV-2 infection during the COVID-19 pandemic,7,8 others failed to observe an association between the course of the COVID-19 infection and blood groups.9,10
It is important to estimate the duration of the hospital stay in COVID-19 patients not only to predict the demand for patient beds, but also to plan the allocation of resources. Therefore, many studies have been performed to assess the risk factors that have an impact on the length of the hospital stay of these patients.11-13 In these studies, a prolonged hospital stay among COVID-19 patients was found to be associated with the female gender, high fever, presence of hepatic or renal disease at presentation, elevated creatinine levels, lymphopenia and presence of bilateral findings in chest CT scan.11,12 However, the effect of some other risk factors have been elusive until now.
In this study, our aim was to evaluate whether the blood group had an effect on the length of the hospital stay. To the best of our knowledge, no previous studies have assessed the effect of ABO blood groups, as well as age, on the length of the hospital stay in these settings.
MethodsIn this retrospective cohort study, patients admitted to our pandemic reference hospital between March 15, 2020 and May 15, 2020 were eligible if they had blood group data available. The 969 patients included in the study were categorized into the following 4 groups based on their ABO blood groups: A, B, O and AB. The ABO blood group distribution according to age, Rh status, demographic data, comorbid conditions, hematological and inflammatory parameters, PCR and imaging findings, treatments received, duration of hospital stay, need for intensive care unit admission and discharge and mortality rates were analyzed. Patients admitted to clinical wards or the intensive care unit were included if they presented a known blood group, positive PCR test, and/or suspected COVID-19 infection (PCR negative, but presenting with the following symptoms: high fever, sore throat, shortness of breath and/or typical bilateral ground-glass appearance in thoracic CT images consistent with pulmonary involvement of the COVID-19 disease). Patients under 18 years of age, treated on an outpatient basis or having missing data, were excluded.
The study protocol was approved by the local ethics committee at the SBU Bursa Yuksek Ihtisas Research and Training Hospital (date, 10.06.2020; no, 2011-KAEK-25 2020/06-06) and the study was conducted in accordance with the principles of the Declaration of Helsinki. In addition, the study protocol was approved by the Turkish Ministry of Health for COVID-19 research. This study used the data collected during the routine clinical practice for COVID-19 patients and the data were handled anonymously.
Statistical analysisThe IBM SPSS Statistics version 21.0 software (SPSS Inc., Chicago, IL) was used for the analysis of the data. The descriptive data are presented in number (percentage), median (min-max) or mean ± standard deviation, where appropriate. Categorical variables were compared using the Pearson's chi-square test or Fisher's exact test. The ANOVA or Kruskal-Wallis was used, where appropriate, in comparing demographics, comorbidities and medications across blood types. A univariate screen between the blood type and demographics, comorbidities and the outcomes of interest were performed using the Chi-square test for categorical variables and the Student's t-test or the Wilcoxon rank-sum for continuous variables, as appropriate. The blood type, sex, age, comorbidities, inflammatory markers and length of stay in the hospital were determined for adjustment, as these covariates were thought to be potential confounders. The model was run for each blood type against all others. Logistic regression was performed for univariate analysis of hematological/inflammatory parameters and blood types for their association with mortality. Two-sided p-values < 0.05 were considered an indication of statistical significance.
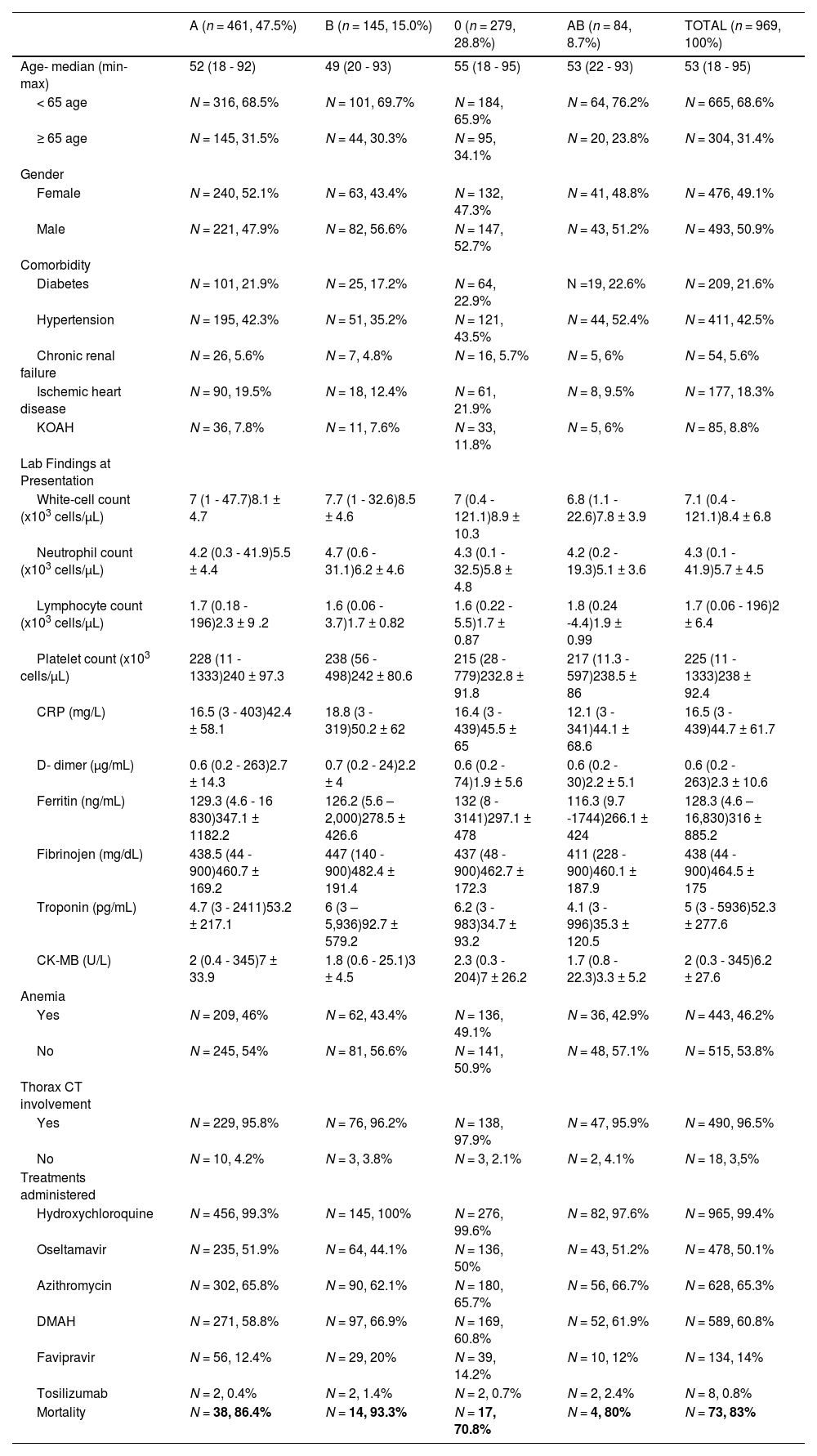
ResultsThere were 969 participants with a mean age of 53.4 ± 19 years. Fifty percent of the patients were female and approximately one-third were over 65 years of age. The ABO blood group type distribution was as follows: type A, 461 subjects (47.6%); type O, 279 patients, (28.8%); type B, 145 subjects (15 %), and; type AB (8.6%). The most common comorbidity was hypertension (HT), which was present in 42.5% of the patients. The ABO groups were comparable with respect to the distribution of comorbid conditions. Of all the patients, 81.4% had no lymphopenia, while 18.6% had lymphopenia and 3.3%, severe lymphopenia. Again, hematologic/inflammatory parameters at presentation did not differ significantly among the ABO blood groups. Of the 508 patients in whom thorax CT results were available, 96.5% had imaging findings consistent with the COVID-19 infection. Additionally, there were no significant differences in terms of pulmonary involvement among the patients with different ABO types. The most commonly utilized agent for treatment was hydroxychloroquine in 99.4%, followed by oseltamivir in 50.1%. Additional enoxaparin was administered to 60.8% of the patients during the course of the treatment (Table 1).
Demographic characteristics according to blood type.
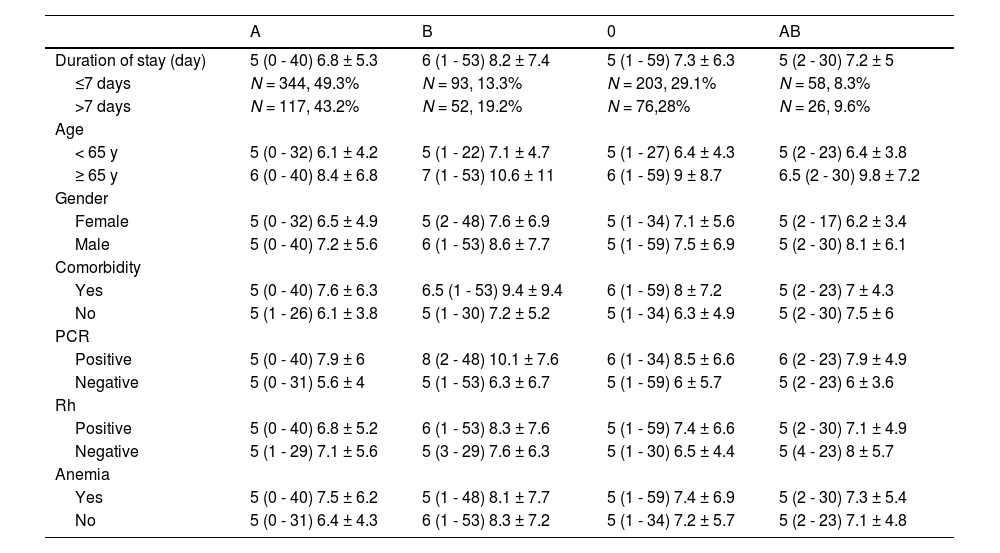
The mean duration of the hospital stay was 7.2 ± 5.9 days, with 28% of the patients staying more than 7 days in the hospital. The duration of the hospital stay in blood groups A, B, AB, and 0 was 5 (0 - 40), 6 (1 - 53), 5 (2 - 30) and 5 (1 - 59) days, respectively, with the differences being insignificant (Table 2). Age was an important determinant for the duration of the hospital stay. Accordingly, the length of the hospital stay in those ≥ 65 years of age vs. < 65 years of age was significantly different for the blood groups A (p = 0.002), AB (p = 0.013) and 0 (p = 0.008), while no difference were found for the blood group B (p = 0.161). The presence of a comorbidity was associated with significant differences in the length of the hospital stay among blood group 0 patients, while no such difference was observed in other blood groups. In addition, significant differences in the length of the hospital stay were found for PCR-positive patients with blood groups A, B and O, while no difference was found in the AB blood group patients (p = 0.000 and p = 0.074, respectively). Gender, presence of anemia and Rh status were not associated with significant differences in the length of the hospital stay.
Length of hospital stay according to blood type and clinical characteristic.
Of all the patients, 9.1% required admission to the intensive care unit (ICU), of whom 83% died. The average length of ICU stay was 11 days (0 - 59). The observed mortality rates in blood groups A, B, AB and 0 were 86.4%, 93.3%, 80.0% and 70.8%, respectively, indicating similar death rates in all ABO blood types (Table 1). When the Rh phenotype was taken into consideration, no significant changes in results were seen.
In patients admitted to the ICU, there were no age, gender, laboratory, anemia or CT finding differences according to the blood type (Table 1). Again, the length of the hospital stay and mortality did not differ significantly among the blood groups (Table 2).
DiscussionIn this study, the effect of the ABO blood type on the course of disease, need for intensive care, length of the hospital stay and mortality according to the age of patients with the COVID-19 infection, particularly in respect to geriatric patients.
In previous studies, the ABO blood type has been found to be directly or indirectly related to certain diseases and individuals with a particular blood type were found to have an increased predisposition for certain cardiovascular and metabolic disorders or infections. For example, increased incidence of thrombotic events and myocardial infarction were reported for blood types A, B and AB, while blood group O presented with hypertensive conditions. Furthermore, the presence of the A antigen appears to be a predisposing factor for thromboembolism, hyperlipidemia, hypercholesterolemia and diabetes mellitus.14,15
Moreover, the link between infections and ABO blood groups was explored, with particular attention to SARS coronavirus (SARS-CoV). The original SARS outbreak, occurring in the 2002 - 2003 winter months, affected more than 8,000 individuals globally, with a mortality rate of 10%.5 Similar to other human coronaviruses, the SARS-CoV infects the mucosal epithelium and leads to an acute respiratory disease, frequently accompanied by gastroenteritis. Guillon et al. proposed that blood group O individuals were more resistant to SARS-CoV due to the presence of ABO antibodies and this could lead to reduced infection rates in the population, based on both epidemiologic and in vitro studies.5 Cheng et al. reported a significant link between the ABO type and the risk of acquiring the infection and subjects with blood group O were less likely to be infected with the SARS coronavirus.16 Similarly, multiple studies showed a significantly higher SARS-CoV-2 infection risk for blood group A, while blood group O was associated with a lower risk level.7,8,17
The ABO and Rh blood type distribution may vary according to the ethnicity and geographical region.18 In the Turkish blood group, A, O, B and AB have a prevalence of 42.84%, 32.67%, 16.46% and 8.03%, respectively, with an overall Rh positivity of 88.54%.19 The corresponding figures reported by Gül et al. in 2005 for the Istanbul Province were 43.44%, 33.02%, 15.00%, and 8.54%, respectively.20 Again, Salduz et al. reporting on a population in Istanbul, observed prevalence rates of 44.3%, 35.7%, 12.5% and 7.5%, for blood groups A, O, B and AB, respectively, with 84.9% of the individuals having Rh positivity.21 In a 2018 study by Cekdemir et al., the reported figures were 44.3%, 35.7%, 12.5% and 7.5% for these respective blood types, and Rh positivity was detected in 84.9% of the participants.22 Eren et al., in their 2019 study based on a population in Istanbul, did not study the Rh factor, but most individuals had blood group A (43.81%), followed by blood group O (33.79%), B (15.21%) and AB (7.16%).23 In our study involving 969 patients with the COVID-19 infection, similar to the figures above, most patients had blood group A and a lower number of patients had blood group AB, with 47.6%, 28.8%, 15% and 8.6% of the subjects having blood group A, O, B and AB, respectively, while Rh positivity was observed in 86.3%. When consideration to previous studies in our region is given, it appears that more patients with blood group A had the COVID-19 infection, and a reduced frequency of infection was found in subjects with blood group O in our sample.
Zeng et al. found a higher risk for COVID-19 infection in people with blood group A, although they failed to confirm a protective effect of blood group O against COVID-19.10 In a meta-analysis, Wu et al. found a higher risk for COVID-19 infection for blood group A and a lower risk for blood group O, although ABO blood groups overall were not significantly associated with the severity and mortality of COVID-19 infections.24 Boudin et al., examining a group of young and healthy subjects with no significant comorbidities trapped in a aircraft carrier, found that the ABO and Rh (D) blood types were not associated with an increased or decreased risk for the SARS-CoV-2 infection. The ABO groups were only potentially associated with severe forms of COVID-19 and comorbidity.25 In a retrospective analysis by Latz et al., there were no significant associations between the ABO blood groups and the need for hospital admission, as well as the rates of intubation and mortality in patients with COVID-19.26 This was corroborated by Dizk et al., who showed no associations between the ABO blood group polymorphisms and death rate due to COVID-19.9 Similarly, we also failed to detect any significant predictive value of blood groups and Rh type for the need for intubation or ICU admission and mortality. The ABO blood group type is thought to play a facilitating role in the acquisition of the COVID-19 infection, although blood groups do not have an impact on the course of the disease and the major determinants of the disease course include other underlying comorbid and thromboinflammatory processes, rather than the blood type itself.
In some previous studies, an association and an effect of blood group types have been proposed in COVID-19. The spike (S) protein of SARS-CoV-2, which is a transmembrane protein, has been found to bind to the human ACE II receptor with high affinity and use this as an entry route to invade the target cells.27 Attachment of the spike protein to the ACE II receptor on the surface of the host cell may be inhibited by the presence of anti-A antibodies.
The COVID-19 infection remains a major public health threat in many countries and it is currently not possible to estimate when the pandemic will terminate. Therefore, proactive strategies based on the current status of the population characteristics and health resources carry a major significance for successful management of the pandemic and to prevent the failure of the health systems. In this regard, predicting the possible length of the hospital stay and associated risk factors may prove to be valuable. It has been previously reported in many studies that patient characteristics, such as age and comorbidity, have an impact on the duration of the hospital stay.28-30 In this study involving a sample of Turkish patients with COVID-19, we investigated whether age and ABO blood type were among the factors associated with a prolonged hospital stay and we failed to observe significant associations between blood groups and clinical outcomes.
LimitationsOne limitation of this study was its single-center design. Inclusion of more centers and patients could better elucidate the association between blood groups and clinical outcomes, as well as the length of hospital stay according to age. These data relate to the initial first months of the pandemic in our country. Therefore, changes in the patient profile and treatment protocols could have an effect on the length of the hospital stay. Furthermore, an optimal control group was not included to compare the blood group distribution. While performing the comparisons, previous studies in our region were also taken into consideration. These factors could have introduced an element of bias into our results.
ConclusionsIn summary, although the blood group type may represent a factor in the acquisition of the COVID-19 infection, it does not seem to have a major impact on the treatment course and disease prognosis, when it was taken into consideration together with the overall clinical characteristics of the patients. Additionally, the ABO blood group type did not have an effect on the course of the disease and the length of the hospital stay among elderly patients. In conclusion, further prospective and molecular studies are warranted to shed more light on the link between blood groups and the course of the COVID-19 infection.
All authors declare no conflict of interest.



