

To present the results of the application of the Blood Donation Knowledge Questionnaire in a large and representative sample of users of primary care services in order to extend the evaluation of the metrics of the items and to assess knowledge about blood donation in association with sociodemographic variables.
MethodThe Blood Donation Knowledge Questionnaire is composed of 24 items based on blood donation requirements of the Brazilian Ministry of Health and on some popular beliefs and concepts of the Brazilian population regarding the blood donation process. Data collection was carried out in 12 healthcare facilities of Ribeirão Preto, São Paulo. The analysis of items was performed using classical test theory with associations being assessed using the multivariate Tobit regression model.
ResultsA total of 1055 individuals participated (79.7% females and a mean age of 40.6 years). Previous blood donation was reported by 246 (23.3%) participants, 669 (63.4%) had never donated, and 140 (13.3%) reported being ineligible to donate blood. This questionnaire is comprised of items considered easy-to-understand, with a facility level of medium to high and generally an adequate capability of discrimination. Higher means of correct answers were detected among females, individuals with more schooling, and subjects who had already donated blood.
ConclusionThe Blood Donation Knowledge Questionnaire is an instrument that aims to measure some general aspects of knowledge regarding blood donation and can be used in different contexts. There is evidence that knowledge of primary healthcare users regarding blood donation is correlated to sex, educational level, and previous blood donation.
While the number of blood transfusions in Brazil is increasing by around 6% per year, the prevalence of voluntary blood donors in Brazil has stabilized1 with approximately 1.8% of the Brazilian population donating blood in recent years.1 This rate, however, is far from the goal of the World Health Organization (WHO) which is 3% of the donor population.2 Reasons for the lack of blood donors in low- to middle-income countries are multifactorial and despite efforts to understand the perceptions, motivation and obstacles about voluntary blood donation, little is known about these factors in the Brazilian context.3,4
Knowledge of the general population about donation is considered a determining factor in the decision to donate blood, in particular, in countries where this action is voluntary.5,6 On the other hand, lack of knowledge about eligibility criteria, the need for blood, and the general blood donation process such as donor safety, quality of service, place of collection, blood usage, together with countless popular beliefs and misconceptions about the donation process, contribute to the low prevalence of voluntary blood donors worldwide.5,7 According to Kumari and Raina,6 it is common for individuals with little knowledge about blood donation to rate themselves as ineligible to donate and this misperception can be perpetuated for many years, reducing the percentage of donors. In addition, greater knowledge of the population on this subject contributes to greater security during the process and the quality of the service, motivating new donors and increasing return rates of those already recruited.8
The assessment of knowledge about blood donation in the Brazilian general population is still incipient. In addition to the low number of studies with large representative samples, there is no specific instrument to ascertain this knowledge considering the specificities of blood donation in Brazil. Thus, our research group developed a 24-item scale named the Blood Donation Knowledge Questionnaire (BDKQ-Brazil)9 based on an instrument proposed by Renzaho and Polonsky.10 BDKQ-Brazil includes questions based on some popular beliefs and notions common to the Brazilian population. Its objective is to evaluate knowledge about the donation process according to blood donation specificities in Brazil based on the requirements of the Brazilian Ministry of Health and some popular beliefs and concepts regarding the donation of blood. BDKQ-Brazil was first published in 2016 in the Brazilian Journal of Hematology and Hemotherapy in the format of a letter to the editor along with its content validity.9 Subsequently, the scale was applied to a large and representative sample of users of primary healthcare services in the municipality of Ribeirão Preto, São Paulo; the results of which are presented herein.
The Brazilian primary healthcare system focuses on actions for health promotion and disease prevention. Thus, the main reason to perform this study at public healthcare facilities is that many of the users have frequent or regular appointments for basic routine clinical, physical, and laboratorial examinations and preventive visits.11 Hence, most users are commonly invited to participate in actions to prevent disease and promote health and we believe that many of them could be suitable to donate blood.
The objective of this study is to present the results of the application of BDKQ-Brazil in users of primary healthcare services thereby extending the evaluation of the metrics of the items when applied to a large representative sample, and assess knowledge about blood donation and possible associations with sociodemographic and behavioral characteristics.
MethodsStudy design, sampling and data collectionA cross-sectional study was conducted of 1055 primary healthcare users at 12 facilities from September 2015 to May 2016. Randomized stratified sampling was adopted. The study was conducted in Ribeirão Preto, which is the eighth largest municipality in São Paulo State with an estimated population of 682,302 in 2017. Ribeirão Preto is considered a technology center and has a high human development index compared to the rest of the country. In addition, the municipality is an important center for health, education, research, business tourism and culture.12
To obtain a representative sample of users of primary healthcare services, the 41 healthcare facilities of the municipality were grouped into 12 strata according to two factors: (1) the district in which they are located; (2) the Paulista Social Vulnerability Index (IPVS)13 prevalent in their area of coverage. The IPVS classifies the census tract sectors in six groups of social vulnerability (very high to low vulnerability) considering socioeconomic dimensions and the family life cycle. Thus, one healthcare facility was selected randomly within each stratum, totaling 12 healthcare facilities in which data collection was performed.
The sample size was calculated considering a confidence coefficient of 95% and an absolute precision of 3% for the estimation of the proportion of blood donors. The number of interviews in each healthcare facility was proportional to the respective population size and number of consultations per month with the total sample size estimated for this study being 1054 interviews.
Three trained interviewers were involved in data collection with the BDKQ-Brazil, a sociodemographic and behavioral questionnaire, and questions about previous donations being applied in a confidential face-to-face interview using paper forms. All potential participants were approached and invited to participate while they were waiting for medical consultations in the waiting rooms of healthcare facilities. The participants were informed about the objectives of the study, expected duration of the interview and the ethical aspects involved. The exclusion criteria adopted were related to age and mental/cognitive disability. Only over 18-year-old subjects, who did not present any impediment to answer the questions, participated in the study. Data were later entered in an online form by a trained member of the research staff with the database being revised routinely to avoid data entry errors.
Regarding blood donation, the participants were questioned about previous donations and ineligibility and were classified as ‘already donated’, ‘never donated’, or ‘unable to donate blood’ (self-declared). In addition, a questionnaire with sociodemographic questions including sex, age, marital status, socioeconomic class, educational level and self-perception of health was also applied. The participants were classified by socioeconomic levels – monthly family income (socioeconomic classes: A, B, C and D/E) and schooling (illiterate, elementary, middle school, high school, and higher education) according to the Brazilian Economic Classification Criteria (ABEP).14
Analysis of items of the BDKQ-Brazil and associationsThe classification of the participants regarding performance in the instrument was conducted according to the Kelley15 proposal that considers the top 27% and the bottom 27% of the participants in the instrument to estimate the cut-off points. In the case of the BDKQ-Brazil (24 items), the cut-off points adopted for the classification of participants with the best and worst performances were ≥19 correct answers and ≤13 correct answers, respectively. The quality of items of the BDKQ-Brazil was assessed using classical test theory taking the difficulty and discrimination index as parameters.16 For the facility index, the degree of facility of items was estimated by the proportion of correct answers; each item can be classified as ‘very easy’ (proportion of right answers from 80 to 100%), ‘easy’ (60–80%), ‘average difficulty’ (40–60%), ‘difficult’ (20–40%) and ‘very difficult’ (0–20%). The discrimination index allows an analysis of how effectively each item can discriminate the respondents who had the best and the worst performances when answering the instrument. In other words, the greater the difference in the proportion of correct answers among the participants with the best and the worst performance, the greater the power of discrimination of the item. Results from 0 to 30% in the discrimination index represent a weak discrimination, from 30 to 60% a moderate discrimination and from 60 to 100% a strong discrimination.17 Thus, the purpose of this analysis is to identify easy items (most likely to be answered correctly) that have a high discriminatory power.
The answers of each item in the BDKQ-Brazil were analyzed according to sex and previous blood donation using the chi-square test. The analysis of associations considering sociodemographic/behavioral variables, previous blood donation and the means of correct answers of the instrument was performed using a multivariate Tobit regression model.18 The Tobit model is a regression model in which the dependent variable is truncated from below or above or both. In this case, the number of correct answers in the instrument is a variable ranging from 0 to 24. All analyses were performed using the SAS software, version 9.4 (SAS Institute).
Ethical considerationsThis study was approved by the Ethics Committee on Human Research of the Hospital das Clínicas in Ribeirão Preto (CAAE: 38148814.2.0000.5440), and data collection in health facilities was approved by the Ribeirão Preto Municipal Health Department. Only adult individuals (≥18 years) who agreed and signed informed consent forms participated in the study. The questionnaires were stored separately from the informed consent terms to ensure participants’ anonymity during data processing.
ResultsA total of 1055 primary healthcare users (80.7% of the total invited) answered all the questions of the questionnaire and were included in the study. The sample was composed of 841 (79.7%) females with a mean age of 45.1 years [standard deviation (SD): 15.3] and 214 (20.3%) males with a mean age of 39.5 years (SD: 14.9). Of the participants, 669 (63.4%) had never donated blood, 246 (23.3%) had already donated blood, and 140 (13.3%) declared themselves unable to donate blood.
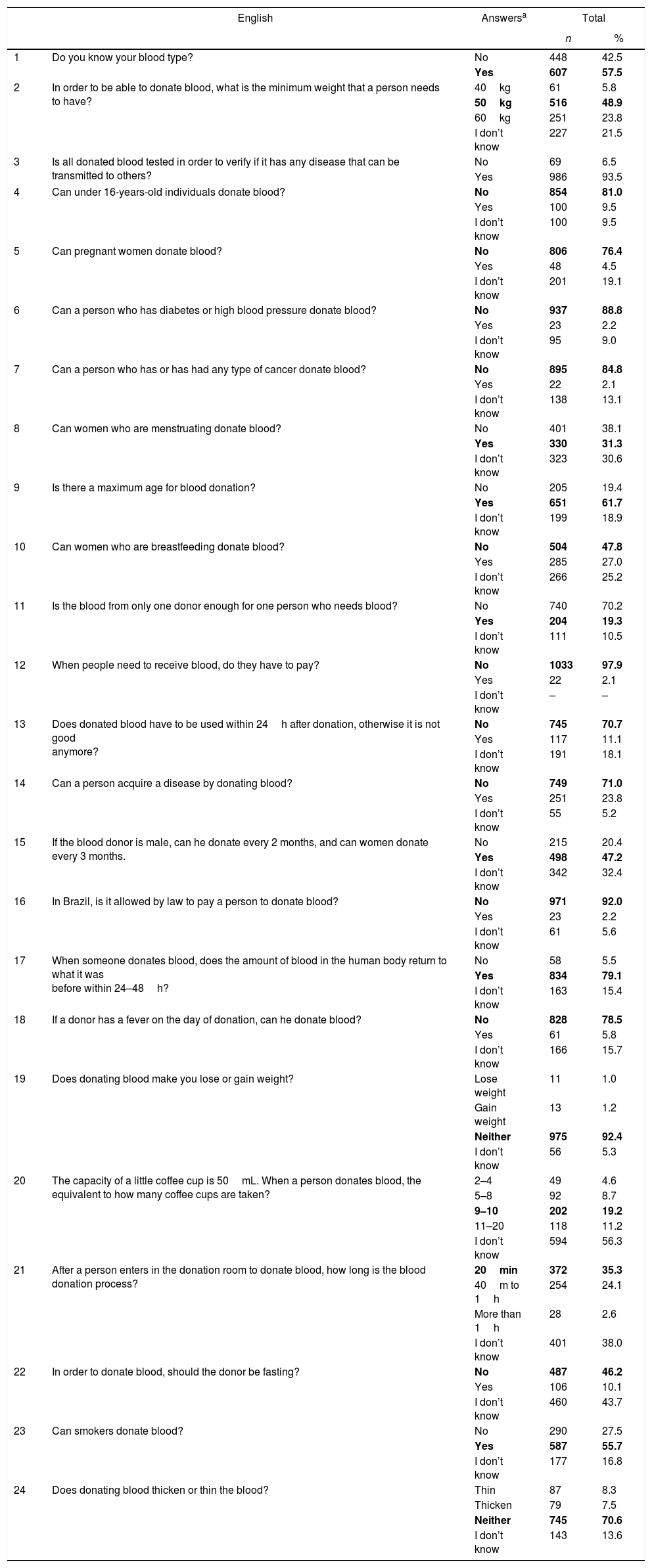
Table 1 shows the study participants’ answers of the BDKQ-Brazil. The vast majority of the participants (n=1003; 97.9%) replied that people do no pay to receive blood transfusions, 986 (93.5%) answered that all donated blood is tested for infectious diseases and only 607 (57.5%) declared to be aware of their blood type. In addition, a large number of participants (56.3%) stated that they did not know how much blood is taken in each blood donation and 38.0% did not know how long the blood donation process takes.
Answers to the Blood Donation Knowledge Questionnaire (BDKQ-Brazil) by 1055 primary healthcare users.
| English | Answersa | Total | ||
|---|---|---|---|---|
| n | % | |||
| 1 | Do you know your blood type? | No | 448 | 42.5 |
| Yes | 607 | 57.5 | ||
| 2 | In order to be able to donate blood, what is the minimum weight that a person needs to have? | 40kg | 61 | 5.8 |
| 50kg | 516 | 48.9 | ||
| 60kg | 251 | 23.8 | ||
| I don’t know | 227 | 21.5 | ||
| 3 | Is all donated blood tested in order to verify if it has any disease that can be transmitted to others? | No | 69 | 6.5 |
| Yes | 986 | 93.5 | ||
| 4 | Can under 16-years-old individuals donate blood? | No | 854 | 81.0 |
| Yes | 100 | 9.5 | ||
| I don’t know | 100 | 9.5 | ||
| 5 | Can pregnant women donate blood? | No | 806 | 76.4 |
| Yes | 48 | 4.5 | ||
| I don’t know | 201 | 19.1 | ||
| 6 | Can a person who has diabetes or high blood pressure donate blood? | No | 937 | 88.8 |
| Yes | 23 | 2.2 | ||
| I don’t know | 95 | 9.0 | ||
| 7 | Can a person who has or has had any type of cancer donate blood? | No | 895 | 84.8 |
| Yes | 22 | 2.1 | ||
| I don’t know | 138 | 13.1 | ||
| 8 | Can women who are menstruating donate blood? | No | 401 | 38.1 |
| Yes | 330 | 31.3 | ||
| I don’t know | 323 | 30.6 | ||
| 9 | Is there a maximum age for blood donation? | No | 205 | 19.4 |
| Yes | 651 | 61.7 | ||
| I don’t know | 199 | 18.9 | ||
| 10 | Can women who are breastfeeding donate blood? | No | 504 | 47.8 |
| Yes | 285 | 27.0 | ||
| I don’t know | 266 | 25.2 | ||
| 11 | Is the blood from only one donor enough for one person who needs blood? | No | 740 | 70.2 |
| Yes | 204 | 19.3 | ||
| I don’t know | 111 | 10.5 | ||
| 12 | When people need to receive blood, do they have to pay? | No | 1033 | 97.9 |
| Yes | 22 | 2.1 | ||
| I don’t know | – | – | ||
| 13 | Does donated blood have to be used within 24h after donation, otherwise it is not good anymore? | No | 745 | 70.7 |
| Yes | 117 | 11.1 | ||
| I don’t know | 191 | 18.1 | ||
| 14 | Can a person acquire a disease by donating blood? | No | 749 | 71.0 |
| Yes | 251 | 23.8 | ||
| I don’t know | 55 | 5.2 | ||
| 15 | If the blood donor is male, can he donate every 2 months, and can women donate every 3 months. | No | 215 | 20.4 |
| Yes | 498 | 47.2 | ||
| I don’t know | 342 | 32.4 | ||
| 16 | In Brazil, is it allowed by law to pay a person to donate blood? | No | 971 | 92.0 |
| Yes | 23 | 2.2 | ||
| I don’t know | 61 | 5.6 | ||
| 17 | When someone donates blood, does the amount of blood in the human body return to what it was before within 24–48h? | No | 58 | 5.5 |
| Yes | 834 | 79.1 | ||
| I don’t know | 163 | 15.4 | ||
| 18 | If a donor has a fever on the day of donation, can he donate blood? | No | 828 | 78.5 |
| Yes | 61 | 5.8 | ||
| I don’t know | 166 | 15.7 | ||
| 19 | Does donating blood make you lose or gain weight? | Lose weight | 11 | 1.0 |
| Gain weight | 13 | 1.2 | ||
| Neither | 975 | 92.4 | ||
| I don’t know | 56 | 5.3 | ||
| 20 | The capacity of a little coffee cup is 50mL. When a person donates blood, the equivalent to how many coffee cups are taken? | 2–4 | 49 | 4.6 |
| 5–8 | 92 | 8.7 | ||
| 9–10 | 202 | 19.2 | ||
| 11–20 | 118 | 11.2 | ||
| I don’t know | 594 | 56.3 | ||
| 21 | After a person enters in the donation room to donate blood, how long is the blood donation process? | 20min | 372 | 35.3 |
| 40m to 1h | 254 | 24.1 | ||
| More than 1h | 28 | 2.6 | ||
| I don’t know | 401 | 38.0 | ||
| 22 | In order to donate blood, should the donor be fasting? | No | 487 | 46.2 |
| Yes | 106 | 10.1 | ||
| I don’t know | 460 | 43.7 | ||
| 23 | Can smokers donate blood? | No | 290 | 27.5 |
| Yes | 587 | 55.7 | ||
| I don’t know | 177 | 16.8 | ||
| 24 | Does donating blood thicken or thin the blood? | Thin | 87 | 8.3 |
| Thicken | 79 | 7.5 | ||
| Neither | 745 | 70.6 | ||
| I don’t know | 143 | 13.6 | ||
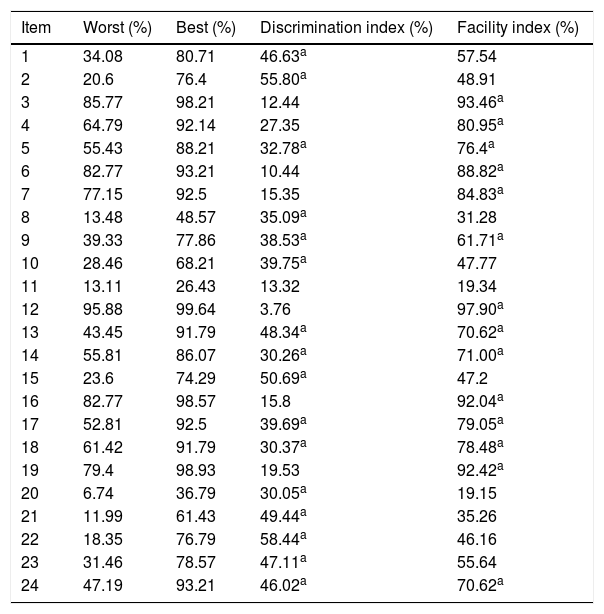
The quality of items of the BDKQ-Brazil according to facility and discrimination indices obtained in classical test theory are shown in Table 2. Items 5, 9, 13, 14, 17, 18, and 24 were distinguished by the two indices as easy to very easy results with a power of discrimination from moderate to strong.
Quality of items of BDKQ-Brazil according to facility and discrimination indexes obtained using classical test theory for the sample of primary healthcare users (n=1055).
| Item | Worst (%) | Best (%) | Discrimination index (%) | Facility index (%) |
|---|---|---|---|---|
| 1 | 34.08 | 80.71 | 46.63a | 57.54 |
| 2 | 20.6 | 76.4 | 55.80a | 48.91 |
| 3 | 85.77 | 98.21 | 12.44 | 93.46a |
| 4 | 64.79 | 92.14 | 27.35 | 80.95a |
| 5 | 55.43 | 88.21 | 32.78a | 76.4a |
| 6 | 82.77 | 93.21 | 10.44 | 88.82a |
| 7 | 77.15 | 92.5 | 15.35 | 84.83a |
| 8 | 13.48 | 48.57 | 35.09a | 31.28 |
| 9 | 39.33 | 77.86 | 38.53a | 61.71a |
| 10 | 28.46 | 68.21 | 39.75a | 47.77 |
| 11 | 13.11 | 26.43 | 13.32 | 19.34 |
| 12 | 95.88 | 99.64 | 3.76 | 97.90a |
| 13 | 43.45 | 91.79 | 48.34a | 70.62a |
| 14 | 55.81 | 86.07 | 30.26a | 71.00a |
| 15 | 23.6 | 74.29 | 50.69a | 47.2 |
| 16 | 82.77 | 98.57 | 15.8 | 92.04a |
| 17 | 52.81 | 92.5 | 39.69a | 79.05a |
| 18 | 61.42 | 91.79 | 30.37a | 78.48a |
| 19 | 79.4 | 98.93 | 19.53 | 92.42a |
| 20 | 6.74 | 36.79 | 30.05a | 19.15 |
| 21 | 11.99 | 61.43 | 49.44a | 35.26 |
| 22 | 18.35 | 76.79 | 58.44a | 46.16 |
| 23 | 31.46 | 78.57 | 47.11a | 55.64 |
| 24 | 47.19 | 93.21 | 46.02a | 70.62a |
The distribution of answers of the primary healthcare users varied depending on sex and previous blood donations (Table 3). A higher frequency of correct answers to questions such as blood type, donor weight, blood donation during the menstrual period, disease acquired from blood donation, and payment to receive blood transfusion was observed among females. On the other hand, men tended to have a higher frequency of correct answers to the questions evaluating the amount of blood donated, duration of the blood collection process and blood donation by smokers. Participants who had already donated blood had a higher frequency of correct answers to the questions evaluating blood type, minimum weight, time interval between donations, weight gain or loss with blood donation, volume of donated blood, time spent for blood donation, fasting before donation, and thickness or thinness of the blood after donation. The participants who described themselves as unable to donate blood had a higher frequency of correct answers to the question of maximum donation age. Finally, among those who never donated blood, the frequency of correct answers on acquiring disease from blood donation was higher.
Distribution of answer to the BDKQ-Brazil of primary healthcare users according to sex and blood donation practice.
| Item/subject | Answersa | Females | Males | p | Never donated | Unable to donate | Already donated | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |||||
| 1 | Blood type | No | 337 | 40.1 | 111 | 51.9 | <0.01 | 324 | 48.4 | 65 | 46.4 | 59 | 24.0 | <0.01 |
| Yes | 504 | 59.9 | 103 | 48.1 | 345 | 51.6 | 75 | 53.6 | 187 | 76.0 | ||||
| 2 | Weight | 40kg | 44 | 5.2 | 17 | 7.9 | 0.04 | 30 | 4.5 | 10 | 7.1 | 21 | 8.5 | <0.01 |
| 50kg | 429 | 51.0 | 87 | 10.7 | 308 | 46.0 | 65 | 46.4 | 143 | 58.1 | ||||
| 60kg | 193 | 23.0 | 58 | 27.1 | 145 | 21.7 | 45 | 32.1 | 61 | 24.8 | ||||
| I don’t know | 175 | 20.8 | 52 | 24.3 | 186 | 27.8 | 20 | 14.3 | 21 | 8.5 | ||||
| 3 | Blood tests | No | 55 | 6.5 | 14 | 6.5 | 0.99 | 52 | 7.8 | 6 | 4.3 | 11 | 4.5 | 0.10 |
| Yes | 786 | 93.5 | 200 | 93.5 | 617 | 92.2 | 134 | 95.7 | 235 | 95.5 | ||||
| 4 | Minimum age for donation | No | 684 | 81.4 | 170 | 79.4 | 0.80 | 550 | 82.4 | 108 | 77.2 | 196 | 79.7 | 0.07 |
| Yes | 78 | 9.3 | 22 | 10.3 | 51 | 7.6 | 17 | 12.1 | 32 | 13.0 | ||||
| I don’t know | 78 | 9.3 | 22 | 10.3 | 67 | 10.0 | 15 | 10.7 | 18 | 7.3 | ||||
| 5 | Pregnancy | No | 650 | 77.3 | 156 | 72.9 | 0.13 | 505 | 75.5 | 110 | 78.6 | 191 | 77.6 | 0.79 |
| Yes | 33 | 3.9 | 15 | 7.0 | 32 | 4.8 | 4 | 2.9 | 12 | 4.9 | ||||
| I don’t know | 158 | 18.8 | 43 | 20.1 | 132 | 19.7 | 26 | 18.6 | 43 | 17.5 | ||||
| 6 | Diabetes and high blood pressure | No | 752 | 89.4 | 185 | 86.4 | 0.35 | 594 | 88.8 | 123 | 87.9 | 220 | 89.4 | 0.51 |
| Yes | 16 | 1.9 | 7 | 3.3 | 15 | 2.2 | 1 | 0.7 | 7 | 2.9 | ||||
| I don’t know | 73 | 8.7 | 22 | 10.3 | 60 | 9.0 | 16 | 11.4 | 19 | 7.7 | ||||
| 7 | Cancer | No | 719 | 85.5 | 176 | 82.2 | 0.45 | 576 | 86.1 | 122 | 87.2 | 197 | 80.1 | 0.14 |
| Yes | 16 | 1.9 | 6 | 2.8 | 13 | 1.9 | 1 | 0.7 | 8 | 3.2 | ||||
| I don’t know | 106 | 12.6 | 32 | 15.0 | 80 | 12.0 | 17 | 12.1 | 41 | 16.7 | ||||
| 8 | Menstruation | No | 287 | 34.2 | 114 | 53.3 | <0.01 | 253 | 37.9 | 52 | 37.2 | 96 | 39.0 | 0.54 |
| Yes | 291 | 34.6 | 39 | 18.2 | 210 | 31.4 | 38 | 27.1 | 82 | 33.3 | ||||
| I don’t know | 262 | 31.2 | 61 | 28.5 | 205 | 30.7 | 50 | 35.7 | 68 | 27.7 | ||||
| 9 | Maximum age for donation | No | 169 | 20.1 | 36 | 16.8 | 0.12 | 138 | 20.6 | 20 | 14.3 | 47 | 19.1 | <0.01 |
| Yes | 506 | 60.2 | 145 | 67.8 | 382 | 57.1 | 103 | 73.6 | 166 | 67.5 | ||||
| I don’t know | 166 | 19.7 | 33 | 15.4 | 149 | 22.3 | 17 | 12.1 | 33 | 13.4 | ||||
| 10 | Breast-feeding | No | 414 | 49.2 | 90 | 42.1 | 0.17 | 299 | 44.7 | 74 | 52.9 | 131 | 53.2 | 0.07 |
| Yes | 222 | 26.4 | 63 | 29.4 | 189 | 28.2 | 31 | 22.1 | 65 | 26.4 | ||||
| I don’t know | 205 | 24.4 | 61 | 28.5 | 181 | 27.1 | 35 | 25.0 | 50 | 20.3 | ||||
| 11 | Volume demand | No | 585 | 69.6 | 155 | 72.4 | 0.70 | 464 | 69.4 | 94 | 67.1 | 182 | 74.0 | 0.44 |
| Yes | 165 | 19.6 | 39 | 18.2 | 133 | 19.9 | 27 | 19.3 | 44 | 17.9 | ||||
| I don’t know | 91 | 10.8 | 20 | 9.4 | 72 | 10.8 | 19 | 13.6 | 20 | 8.1 | ||||
| 12 | Pay for transfusion | No | 825 | 98.1 | 208 | 97.2 | 0.41 | 654 | 97.8 | 138 | 98.6 | 241 | 98.0 | 0.83 |
| Yes | 16 | 1.9 | 6 | 2.8 | 15 | 2.2 | 2 | 1.4 | 5 | 2.0 | ||||
| 13 | Blood durability | No | 587 | 70.0 | 158 | 73.8 | 0.17 | 459 | 68.7 | 99 | 70.7 | 187 | 76.3 | 0.21 |
| Yes | 101 | 12.0 | 16 | 7.5 | 81 | 12.1 | 13 | 9.3 | 23 | 9.4 | ||||
| I don’t know | 151 | 18.0 | 40 | 18.7 | 128 | 19.2 | 28 | 20.0 | 35 | 14.3 | ||||
| 14 | Acquire disease in blood donation | No | 619 | 73.6 | 130 | 60.8 | <0.01 | 494 | 73.9 | 89 | 63.6 | 166 | 67.5 | <0.01 |
| Yes | 176 | 20.9 | 75 | 35.0 | 134 | 20.0 | 46 | 32.9 | 71 | 28.9 | ||||
| I don’t know | 46 | 5.5 | 9 | 4.2 | 41 | 6.1 | 5 | 3.5 | 9 | 3.6 | ||||
| 15 | Period between donations | No | 167 | 19.9 | 48 | 22.4 | 0.09 | 133 | 19.9 | 25 | 17.8 | 57 | 23.2 | <0.01 |
| Yes | 388 | 46.1 | 110 | 51.4 | 278 | 41.5 | 74 | 52.9 | 146 | 59.3 | ||||
| I don’t know | 286 | 34.0 | 56 | 26.2 | 258 | 38.6 | 41 | 29.3 | 43 | 17.5 | ||||
| 16 | Payment for blood donors | No | 784 | 93.2 | 187 | 87.4 | <0.01 | 610 | 91.2 | 130 | 92.8 | 231 | 93.9 | 0.15 |
| Yes | 11 | 1.3 | 12 | 5.6 | 12 | 1.8 | 5 | 3.6 | 6 | 2.4 | ||||
| I don’t know | 46 | 5.5 | 15 | 7.0 | 47 | 7.0 | 5 | 3.6 | 9 | 3.7 | ||||
| 17 | Blood volume replacement | No | 39 | 4.6 | 19 | 8.9 | 0.05 | 31 | 4.6 | 7 | 5.0 | 20 | 8.1 | <0.01 |
| Yes | 669 | 79.6 | 165 | 77.1 | 520 | 77.7 | 107 | 76.4 | 207 | 84.2 | ||||
| I don’t know | 133 | 15.8 | 30 | 14.0 | 118 | 17.6 | 26 | 18.6 | 19 | 7.7 | ||||
| 18 | Fever | No | 662 | 78.7 | 166 | 77.6 | 0.94 | 521 | 77.9 | 111 | 79.3 | 196 | 79.7 | 0.69 |
| Yes | 48 | 5.7 | 13 | 6.1 | 38 | 5.7 | 6 | 4.3 | 17 | 6.9 | ||||
| I don’t know | 131 | 15.6 | 25 | 16.3 | 110 | 16.4 | 23 | 16.4 | 33 | 13.4 | ||||
| 19 | Gain or lose weight | Lose weight | 7 | 0.8 | 4 | 1.9 | 0.05 | 8 | 1.2 | 3 | 2.1 | 0 | - | 0.03 |
| Gain weight | 7 | 0.8 | 6 | 2.8 | 7 | 1.0 | 2 | 1.4 | 4 | 1.6 | ||||
| Neither | 784 | 93.3 | 191 | 89.2 | 608 | 90.9 | 131 | 93.6 | 236 | 95.9 | ||||
| I don’t know | 43 | 5.1 | 13 | 6.1 | 46 | 6.9 | 4 | 2.9 | 6 | 2.4 | ||||
| 20 | Volume of blood donated | 2–4 | 37 | 4.4 | 12 | 5.6 | <0.01 | 34 | 5.1 | 3 | 2.1 | 12 | 4.9 | <0.01 |
| 5–8 | 66 | 7.8 | 26 | 12.1 | 39 | 5.8 | 12 | 8.6 | 41 | 16.7 | ||||
| 9–10 | 152 | 18.1 | 50 | 23.4 | 84 | 12.6 | 26 | 18.6 | 92 | 37.4 | ||||
| 11–20 | 84 | 10.0 | 34 | 15.9 | 72 | 10.8 | 14 | 10.0 | 32 | 13.0 | ||||
| I don’t know | 502 | 56.7 | 92 | 43.0 | 440 | 65.8 | 85 | 60.7 | 69 | 28.0 | ||||
| 21 | Time spent during donation | 20min | 262 | 31.1 | 110 | 51.4 | <0.01 | 160 | 23.9 | 40 | 28.6 | 172 | 69.9 | <0.01 |
| 40m to 1 hour | 214 | 25.5 | 40 | 18.7 | 176 | 26.3 | 31 | 22.1 | 47 | 19.1 | ||||
| More than 1h | 25 | 3.0 | 3 | 1.4 | 22 | 3.3 | 4 | 2.9 | 2 | 0.8 | ||||
| I don’t know | 340 | 40.4 | 61 | 28.5 | 311 | 46.5 | 65 | 46.4 | 25 | 10.2 | ||||
| 22 | Fasting before donation | No | 399 | 47.5 | 88 | 41.3 | 0.09 | 265 | 39.6 | 65 | 46.4 | 157 | 64.3 | <0.01 |
| Yes | 88 | 10.5 | 18 | 8.5 | 318 | 47.5 | 61 | 43.6 | 81 | 33.2 | ||||
| I don’t know | 353 | 42.0 | 107 | 50.2 | 86 | 12.9 | 14 | 10.0 | 6 | 2.5 | ||||
| 23 | Smokers and blood donation | No | 248 | 29.5 | 42 | 19.6 | <0.01 | 223 | 33.4 | 35 | 25.0 | 32 | 13.0 | <0.01 |
| Yes | 439 | 52.3 | 148 | 69.2 | 330 | 49.4 | 77 | 55.0 | 180 | 73.2 | ||||
| I don’t know | 153 | 18.2 | 24 | 11.2 | 115 | 17.2 | 28 | 20.0 | 34 | 13.8 | ||||
| 24 | Thicken or thin the blood | Thin | 66 | 7.9 | 21 | 9.8 | 0.72 | 55 | 8.2 | 17 | 12.1 | 15 | 6.1 | <0.01 |
| Thicken | 61 | 7.2 | 18 | 8.4 | 48 | 7.2 | 10 | 7.1 | 21 | 8.5 | ||||
| Neither | 599 | 71.3 | 146 | 68.2 | 451 | 67.5 | 101 | 72.2 | 193 | 78.5 | ||||
| I don’t know | 114 | 13.6 | 29 | 13.6 | 114 | 17.1 | 12 | 8.6 | 17 | 6.9 | ||||
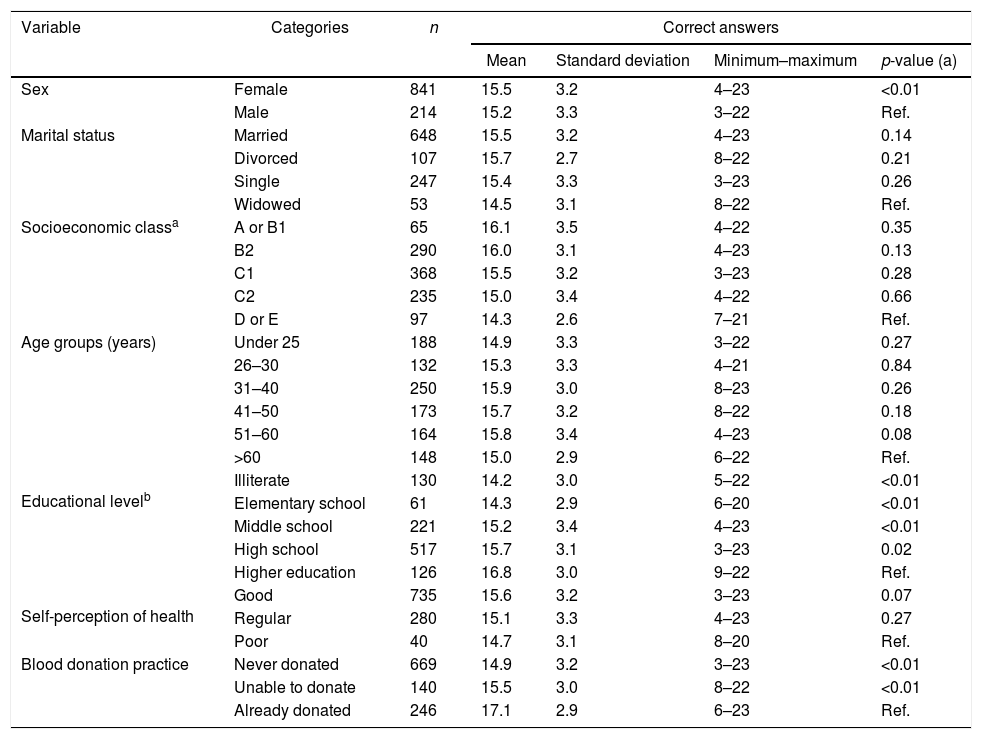
The study of associations considering the mean numbers of correct answers in the BDKQ-Brazil and sociodemographic and behavioral variables are presented in Table 4. Differences in mean numbers were associated with sex, educational level and previous blood donations. Females, study participants with more schooling and those who had already donated blood presented higher numbers of correct answers. No associations of mean numbers of correct answers were found for marital status, socioeconomic class, age group and self-perception of health.
Mean numbers of correct answers of primary healthcare users (n=1055) by sociodemographic and behavioral variables (BDKQ-Brazil).
| Variable | Categories | n | Correct answers | |||
|---|---|---|---|---|---|---|
| Mean | Standard deviation | Minimum–maximum | p-value (a) | |||
| Sex | Female | 841 | 15.5 | 3.2 | 4–23 | <0.01 |
| Male | 214 | 15.2 | 3.3 | 3–22 | Ref. | |
| Marital status | Married | 648 | 15.5 | 3.2 | 4–23 | 0.14 |
| Divorced | 107 | 15.7 | 2.7 | 8–22 | 0.21 | |
| Single | 247 | 15.4 | 3.3 | 3–23 | 0.26 | |
| Widowed | 53 | 14.5 | 3.1 | 8–22 | Ref. | |
| Socioeconomic classa | A or B1 | 65 | 16.1 | 3.5 | 4–22 | 0.35 |
| B2 | 290 | 16.0 | 3.1 | 4–23 | 0.13 | |
| C1 | 368 | 15.5 | 3.2 | 3–23 | 0.28 | |
| C2 | 235 | 15.0 | 3.4 | 4–22 | 0.66 | |
| D or E | 97 | 14.3 | 2.6 | 7–21 | Ref. | |
| Age groups (years) | Under 25 | 188 | 14.9 | 3.3 | 3–22 | 0.27 |
| 26–30 | 132 | 15.3 | 3.3 | 4–21 | 0.84 | |
| 31–40 | 250 | 15.9 | 3.0 | 8–23 | 0.26 | |
| 41–50 | 173 | 15.7 | 3.2 | 8–22 | 0.18 | |
| 51–60 | 164 | 15.8 | 3.4 | 4–23 | 0.08 | |
| >60 | 148 | 15.0 | 2.9 | 6–22 | Ref. | |
Educational levelb | Illiterate | 130 | 14.2 | 3.0 | 5–22 | <0.01 |
| Elementary school | 61 | 14.3 | 2.9 | 6–20 | <0.01 | |
| Middle school | 221 | 15.2 | 3.4 | 4–23 | <0.01 | |
| High school | 517 | 15.7 | 3.1 | 3–23 | 0.02 | |
| Higher education | 126 | 16.8 | 3.0 | 9–22 | Ref. | |
Self-perception of health | Good | 735 | 15.6 | 3.2 | 3–23 | 0.07 |
| Regular | 280 | 15.1 | 3.3 | 4–23 | 0.27 | |
| Poor | 40 | 14.7 | 3.1 | 8–20 | Ref. | |
| Blood donation practice | Never donated | 669 | 14.9 | 3.2 | 3–23 | <0.01 |
| Unable to donate | 140 | 15.5 | 3.0 | 8–22 | <0.01 | |
| Already donated | 246 | 17.1 | 2.9 | 6–23 | Ref. | |
(a) Multivariate Tobit regression model.
The BDQK-Brazil is an original instrument that aims to measure and validate general blood donation knowledge among primary healthcare users.9 The results of this study show that the instrument is comprised of easy-to-understand questions with an adequate discrimination capability, which suggests that it can be used in many settings, including for donors and non-donors, and in different social and educational levels. Higher mean numbers of correct answers were associated with being female, having a higher educational level and previously donating blood.
Higher mean numbers of correct answers were observed among participants who had already donated blood. Donors presented greater knowledge on the blood donation process and lower mean numbers for answers about misconceptions compared to non-donors. It was expected that blood donors would present better knowledge regarding blood donation compared to non-donors,8 and the results of this study have provided evidence for this. If this had not happened, the discrimination power of the BDKQ-Brazil would have been dubious.
Although a higher prevalence of males among blood donors is characteristic in Brazil,3,19 females presented higher mean numbers of correct answers in this study. However, it can be observed that women had more correct answers for questions related to health and general knowledge such as blood type, donor weight, blood donation during menstrual, acquiring disease from blood donation and payment to receive blood. On the other hand, male donors had more correct answers for questions related to the blood donation process and eligibility, such as the volume of blood donated, the duration of the blood donation process and the eligibility of smokers. The results of this study corroborate the concept that blood donors have more knowledge about the donation process.5,20 Previous studies in the Brazilian population showed that individuals with high educational levels are more likely to donate blood,4,21,22 which justifies the number of correct answers according to the educational level of the participants.
In the current sample, levels of blood donation knowledge varied from moderate to high; most items were answered correctly by many participants. However, nearly one third of the study participants incorrectly answered the item on acquiring disease through blood donation. This information as well as other common misconceptions observed in this study are very important and should be discussed in respect to donor recruitment strategies in future campaigns promoted by blood banks.
A limitation of this study is regarding the higher number of women in the sample of primary healthcare users. However, this is a characteristic of the population who seek healthcare services in Brazil.23 Although, in this study the rate of women was higher than expected, we understand that this is an important opportunity to increase knowledge about blood donation among individuals who have never been to a blood bank, an under-studied population in the field of transfusion epidemiology.
The BDKQ-Brazil is an original instrument that aims to measure general aspects of knowledge about blood donation that can be used in many contexts. There is evidence that greater knowledge regarding blood donation is associated with sex, educational level and previous blood donation in primary healthcare users. We strongly suggest that BDKQ-Brazil should be applied aiming to improve the instrument and its adaptation for distinct populations, as well as to fill the gap in the scientific literature in the field of blood donation epidemiology.
Financial supportThis study was supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) under grant # 2014/14020-6 and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
Conflicts of interestThe authors declare no conflicts of interest.


