
Heterogeneity regarding clinical and laboratory findings at diagnosis of acute lymphoblastic leukemia exists. The frequency of complete blood count abnormalities and its combinations, symptoms and physical findings were investigated in Hispanic children from an open population at the diagnosis of acute lymphoblastic leukemia.
MethodsThe patient charts and electronic records of under 16-year-old children diagnosed with acute lymphoblastic leukemia over 10 years at a regional hematology center of a university hospital were analyzed to retrieve data concerning the complete blood count at first evaluation. Type and distribution of abnormal data, frequency of symptoms and physical findings at presentation were documented.
ResultsThe records of 203 children aged 0–15 years diagnosed with acute lymphoblastic leukemia from 2006 to 2016 were revisited. The results of the blood workup showed a median white blood cell count of 7120×109/L (range: 450–600,000×109/L), and a median hemoglobin concentration of 7.5g/dL (range: 2.4–15.3g/dL), whereas the median platelet count was 47,400×109/L (range: 4000–544,000×109/L). Leukocytosis and leukopenia were present in 36.6% and 36.1% of cases, respectively; anemia was diagnosed in 82.9% children. The order of frequency for major clinical symptoms was fatigue 62%, fever 60%, bone and joint pain 39%, hyporexia 33% and weight loss 21%, while main physical findings were hepatomegaly 78%, splenomegaly 63%, lymphadenopathy 57%, pallor 48%, and purpura 30%.
ConclusionData differing from those classically expected at diagnosis of acute lymphoblastic leukemia in children were documented in a cohort of Hispanic children over one decade with a wide spectrum of complete blood count abnormalities, forms of presentation and frequency of physical findings.
Worldwide, around 240,000 new cases of childhood acute leukemia are diagnosed each year. Acute lymphoblastic leukemia (ALL) is the most common type of leukemia among pediatric patients with 75% of cases occurring in developing countries. It represents 76% of leukemias in under 15-year-old patients and 30% of all kinds of cancer in this age group.1 The survival rate of pediatric ALL patients in industrialized countries has improved to approximately 90% in recent years,2,3 with a 93% overall survival recently reported in the United States.4 However, in low- and middle-income nations overall survival varies from 50% to 75%.5 This difference is due to, among other reasons, a delay in the diagnosis and subsequently in the initiation of treatment.6
Risk stratification is pivotal for ALL prognosis and individualized therapy.7 According to the criteria of the National Cancer Institute (NCI), the following features are determinants of high-risk disease: age <1 year or >10 years, initial white blood cell (WBC) count >50×109/L, T-cell ALL (T-ALL), initial central nervous system leukemia (CNSL), slow response to induction chemotherapy, breakpoint cluster region-Abelson murine leukemia (BCR-ABL)/mixed-lineage leukemia (MLL)-AF4 positivity, testicular infiltration, lymphadenopathy, splenomegaly and hepatomegaly.8–12
Acute leukemia is frequently accompanied by anemia, a common clinical complication that is responsible for several symptoms such as fatigue.13 The typical textbook presentation of ALL consists of normocytic normochromic anemia, increased or, less frequently, decreased WBC count, neutropenia and/or the presence of blasts, and thrombocytopenia.10 Opportune diagnosis leads to fast treatment. Thus, it is of critical importance to recognize symptoms early, the presence of specific physical findings, and to interpret the CBC correctly. Studies that center exclusively on the initial findings at the diagnosis of leukemia are scarce. We were unable to find recent information focused on detailed analysis of CBC abnormalities, signs and symptoms, and physical findings in children with newly diagnosed ALL, therefore this report analyzed these data in patients treated at an academic institution over a 10-year period.
MethodsCBC data, signs, symptoms and physical findings of 203 consecutive patients diagnosed with ALL attending the Hematology Department of Dr. José E. González University Hospital, School of Medicine, Universidad Autónoma de Nuevo León in Monterrey, México from 2006 to 2016 were retrospectively reviewed for this study. Both, patient charts and electronic databases were scrutinized. The variables included were age, gender, WBC count and differential leukocyte counts, platelet count and hemoglobin concentration, and their distributions in the context of clinical symptoms, physical findings, and final flow cytometry confirming ALL. The Statistical Package for the Social Sciences (IBM SPSS for Windows, Version 22.0. Armonk, NY: IBM Corp) was used for data analysis. Variables were stratified according to risk categories including age (≤1, 2–9 and ≥10 years), hemoglobin (Hb – <11, 11–14 and >14g/dL), WBC count (<4500×109/L, 4500–14,500×109/L and >14,500×109/L), and platelet count (<150,000×109/L and ≥150,000×109/L). Due to age heterogeneity, ranges of reference blood count values considered normal for each age group were used.14 The protocol of the study was approved by the Institutional Review Board.
ResultsData from 203 children with ALL were studied. Median age at diagnosis was six years (range: 0–15). The prevalent age group was 2–9 years (63%). Children <1 year and ≥10 years of age accounted for 7% and 30% of the cohort, respectively. Male gender predominated slightly at 52% of the total.
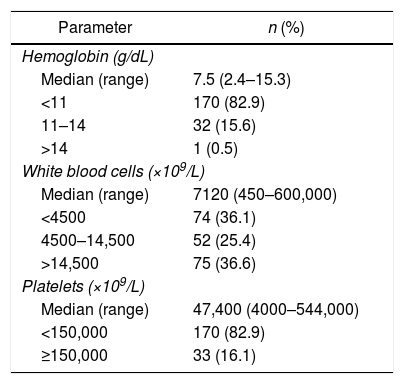
Median values for hematologic parameters were hemoglobin 7.5g/dL (range: 2.4–15.3g/dL); leukocytes: 7120×109/L (range: 450–600,000×109/L) and platelets: 47,400×109/L (range: 4000–544,000×109/L). Anemia (Hb <11.0g/dL) and thrombocytopenia (platelets <150,000×109/L) at diagnosis were each found in 83% (170) of the cases, leukocytosis (WBC >14,500×109/L) in 36.6% (75 cases) and leucopoenia in 36.1% (74 cases). Results are summarized in Table 1.
Initial complete blood count values in 203 children diagnosed with B-cell acute lymphoblastic leukemia at the Dr. José E. González University Hospital, in Monterrey, México.
| Parameter | n (%) |
|---|---|
| Hemoglobin (g/dL) | |
| Median (range) | 7.5 (2.4–15.3) |
| <11 | 170 (82.9) |
| 11–14 | 32 (15.6) |
| >14 | 1 (0.5) |
| White blood cells (×109/L) | |
| Median (range) | 7120 (450–600,000) |
| <4500 | 74 (36.1) |
| 4500–14,500 | 52 (25.4) |
| >14,500 | 75 (36.6) |
| Platelets (×109/L) | |
| Median (range) | 47,400 (4000–544,000) |
| <150,000 | 170 (82.9) |
| ≥150,000 | 33 (16.1) |
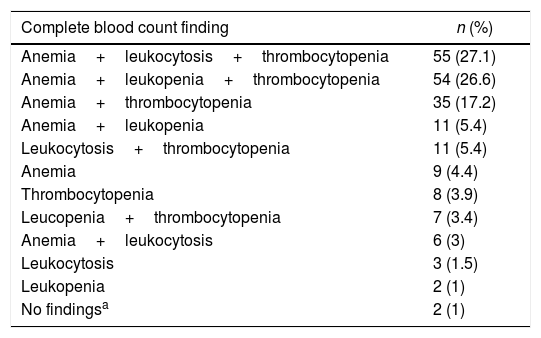
Bicytopenia plus leukocytosis was found in 27.1% of ALL children, whereas bicytopenia plus leucopoenia was present in 26.6%, and bicytopenia plus a normal leukocyte count in 17.2%; frequencies for additional isolated and combined CBC findings are shown in Table 2.
Complete blood count abnormalities in 203 Hispanic children newly diagnosed with acute lymphoblastic leukemia.
| Complete blood count finding | n (%) |
|---|---|
| Anemia+leukocytosis+thrombocytopenia | 55 (27.1) |
| Anemia+leukopenia+thrombocytopenia | 54 (26.6) |
| Anemia+thrombocytopenia | 35 (17.2) |
| Anemia+leukopenia | 11 (5.4) |
| Leukocytosis+thrombocytopenia | 11 (5.4) |
| Anemia | 9 (4.4) |
| Thrombocytopenia | 8 (3.9) |
| Leucopenia+thrombocytopenia | 7 (3.4) |
| Anemia+leukocytosis | 6 (3) |
| Leukocytosis | 3 (1.5) |
| Leukopenia | 2 (1) |
| No findingsa | 2 (1) |
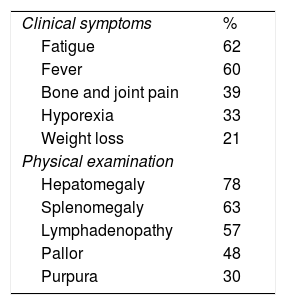
The most frequent symptoms were fatigue in 62%, fever 60%, bone and joint pain 39%, hyporexia 33% and weight loss in 21%. Physical examination at diagnosis revealed hepatomegaly in 78%, splenomegaly in 63%, lymphadenopathy in 57%, pallor in 48%, and purpura in 30%. These results are shown in Table 3.
Symptoms and physical findings in 203 children diagnosed with acute lymphoblastic leukemia at the Dr. José E. González University Hospital, in Monterrey, México.
| Clinical symptoms | % |
| Fatigue | 62 |
| Fever | 60 |
| Bone and joint pain | 39 |
| Hyporexia | 33 |
| Weight loss | 21 |
| Physical examination | |
| Hepatomegaly | 78 |
| Splenomegaly | 63 |
| Lymphadenopathy | 57 |
| Pallor | 48 |
| Purpura | 30 |
The aim of this study was to document the initial data that hematologists find in children diagnosed with ALL. Our hypothesis was that findings differ from those traditionally expected. Interestingly, there is a lack of studies in contemporary literature specifically dealing with type and frequency of CBC variables, symptoms and physical examination findings identified at this early stage in the course of ALL.
The correct interpretation of CBC results, knowledge of early symptoms and detection of key signs during physical examination are essential for a timely diagnosis of childhood ALL, maximizing the opportunity for cure, and thus it is considerably relevant to be aware of the variable spectrum of these data.
There are interesting findings in this study of over 200 children with a confirmed diagnosis of ALL. More frequently expected CBC findings, consisting of leukocytosis plus bicytopenia,10 were found in only about 1 in 4 cases (27%); interestingly, anemia, present in 83% of the current cohort, was one of the most frequent CBC abnormalities. This was the same percentage as for thrombocytopenia, although in different patients. Leukocytosis, alone or combined with another abnormality, was considerably less frequent, in only 37% of the children and almost the same as its opposite, leucopenia, which was found in 36.5% of the cases.
On the other hand, positive physical findings were present in almost 4 of every 5 children, emphasizing the importance of these in the diagnostic process, essential for suspicion and for initiating confirmatory clinical and laboratory work-ups.
Median age at diagnosis was six years and males predominated slightly; studies in Pakistan and Brazil reported similar results.3,15 Age at diagnosis differed significantly from that observed in high-income countries, including the United States, with a peak incidence of children from 1 to 4 years of age.16 Germany, where the peak age is between 1 and 5 years17 and Korea, with a mean age of 3.8±2.3 years.18
The relationship between Hb at diagnosis and prognosis of ALL is controversial and there is scarce information on this particular point. At the beginning of the 1980s a group of hematologists reported that a high WBC count accompanied by a high Hb concentration was associated with a poorer outlook, apparently because this group of children had a rapidly multiplying leukemic clone, presenting clinical manifestations before the Hb concentration had time to drop.19 Recently, however, another group found that precursor B-cell leukemia has a more favorable prognosis if a higher Hb level is present. The investigators suggested that patients with a high Hb concentration were diagnosed at an early stage of disease and were, therefore, more susceptible to successful early chemotherapeutic interventions.20 This apparent discrepancy appears to reflect both a greater awareness of the diagnosis of ALL and the increase in the success rate of curing ALL with contemporary chemotherapy regimens reached in the period spanning over two and a half decades between these reports.
Anemia at diagnosis was present in most of our patients. This finding could be related to late diagnosis, since it is considerably higher than that reported in studies from developed countries. In this respect, in a recent study, anemia was diagnosed in 85% of cases, almost the same proportion as the present research, but with a higher mean hemoglobin concentration of 8.4g/dL vs. 7.5g/dL in this cohort.3 The normal range of the WBC count during childhood is considered to be 4.0–14.5×109/L14; almost 30% of the children in our group had values within this range. This could delay early diagnosis of ALL if physicians expect to find considerably higher or lower WBC counts.
Few studies report the frequency of physical findings. In the current cohort, physical findings were present in 8 of every 10 children, underscoring the critical importance of a detailed physical examination as an essential part of ALL diagnosis. Interestingly hepatomegaly was the most common abnormality in almost 80%, predominating over lymphadenopathy and splenomegaly, both present in about 60%. Physical abnormalities reported in a previous study were hepatomegaly and splenomegaly, in about two-thirds, and lymphadenopathy in only one quarter of cases15; similar findings were reported recently in which hepatomegaly and splenomegaly predominated in about 60% of cases.2 One important challenge for the hematologist is that lymphadenopathy is a non-specific sign. In one study, it was the most common reason for urgent referral to assess malignancy, but often without supporting clinical symptoms and signs or abnormal CBC results. None of the children in that study were ultimately found to have cancer; then in the absence of high-risk features, a rigorous approach to evaluating lymphadenopathy in primary care including an urgent CBC to investigate leukemia is recommended.21 Importantly, this study found lymphadenopathy in almost 60% of children newly diagnosed with ALL.
Fatigue and fever were the most common symptoms in our cohort. In a recent study, signs and symptoms were analyzed in 128 cases before the diagnosis of ALL. The most frequent finding was pallor (83% vs. 42% in this cohort), followed by hyporexia (73% vs. 33%), weight loss (62% vs. 21%), purpura (39% vs. 30%), fever (27% vs. 60%), and fatigue (23% vs. 62%), among other less common findings.22 This demonstrates the considerable heterogeneity in the initial findings at the diagnosis of ALL, probably reflecting the biological variability of the disease.23
Concern over misdiagnosis or delayed diagnosis of children later found to have ALL has recently been raised,24 particularly with respect to those cases presenting with musculoskeletal signs and symptoms, especially those masquerading as arthritis.25 Misdiagnosis or delayed diagnosis was not assessed in the patients of this study; however, it is reasonable to assume that these factors were present in a proportion of our cases, as suggested by the fact that almost 40% reported musculoskeletal pain.
Limitations in the present report include, but are not limited to, its relatively small sample size and the fact that the cross-sectional retrospective design did not allow for collection of additional data, including percentage of blasts in the CBC at the diagnosis of ALL, preventing further analysis of its association with other important clinical and laboratory variables.
In conclusion, there was remarkable heterogeneity in the initial CBC data, symptoms and physical examination findings in children with ALL. In some cases these data differed considerably from those traditionally expected; this heterogeneity is more probably multifactorial and can be a surrogate for other aspects affecting the clinical course of ALL, including time to diagnosis, different mutations and/or polymorphisms involved in its pathogenesis, as well as geographic and other biological influences. It is important to be aware of this heterogeneity, as delayed diagnosis favors disease extension and organ infiltration by leukemic cells, considerably decreasing the chance for curing this, the most curable of childhood hematologic cancers.
Conflicts of interestThe authors declare no conflicts of interest.
The authors gratefully acknowledge Dr. Sergio Lozano for his review of the manuscript.


