
Anemia during childhood is one of the biggest public health problems worldwide, including Brazil. Insufficient or abnormal production of hemoglobin, loss of iron and excessive destruction of red blood cells are the most common causes of anemia. Among the reasons of anemia, iron deficiency accounts for 50% of anemia cases in developing countries. Affected individuals present a wide range of clinical problems, including delayed neuropsychomotor progression, impaired cellular immunity and reduction of intellectual capacity. This study aimed to evaluate the prevalence of anemia in children attending public schools in the metropolitan region of Curitiba, Paraná, Brazil.
MethodA retrospective study was conducted of 409 children aged 8–12 years old included in an extension project of the Universidade Federal do Paraná. The results of complete blood count and hemoglobin electrophoresis of all children were evaluated. Anemia was considered when the hemoglobin levels were <11.5g/dL.
ResultsThe prevalence of anemia was found to be 2.2% of the population studied, with hypochromic microcytic anemia being the most common type. Seven children had sickle cell trait and one had β-thalassemia.
ConclusionThe prevalence of anemia in this study was considered normal according the World Health Organization classification, which is different from the data found in other Brazilian regions.
Anemia is a common clinical condition characterized by decreased hematocrit or hemoglobin (Hb) levels, which are insufficient for the body's demand.1
Mechanisms related to the development of anemia are nutritional deficiencies and genetic or hemorrhagic conditions, leading to an inadequate production or exacerbated destruction of Hb.2,3
The main consequences of anemia are related to delayed psychomotor development, impaired cellular immunity, and low cognitive performance due to poor tissue oxygenation.4,5
The laboratory diagnosis of anemia can be achieved by a complete blood count (CBC), Hb electrophoresis, biochemical markers and genetic tests. The CBC is an important diagnostic tool for the morphological evaluation and Hb content of red blood cells. It directly measures erythropoiesis and, at low levels of Hb, it indicates insufficient essential nutrients in the bone marrow.2,3
Early diagnosis and, more importantly, identifying the etiology of anemia are fundamental not only for adequate treatment but also to design public policies aimed at the promotion and protection of health.6–9
This study aims to evaluate the prevalence of anemia in children attending public schools in the metropolitan region of Curitiba and to contribute to the epidemiological data of this population.
MethodsThis is a retrospective analytical study. A total of 409 children aged 8–12 years old (55.2% female and 44.7% male) who attend public schools in the metropolitan region of Curitiba participated in an extension project of the Pharmacy Course of the Universidade Federal do Paraná (UFPR). The study was approved by the Research Ethics Committee of UFPR (CAAE: 57571316.7.0000.0102). The following data were collected from all 409 children: age, gender, and the results of a CBC and Hb electrophoresis. Samples obtained by venipuncture were collected from March to December 2015 and processed using the ABX Micros 45 hematology analyzer. Anemia is characterized by an Hb level of <11.5g/dL according to the World Health Organization (WHO) criteria.1 Hb electrophoresis was performed at alkaline pH with qualitative results being based on the position of the electrophoretic bands. Solubility tests for Hb S and Hb A2 measurements by the elution method were used as complementary tests. Statistical analysis used the Statsoft software version 10.0 with data being expressed as means and standard deviation (SD) using a 95% confidence interval.
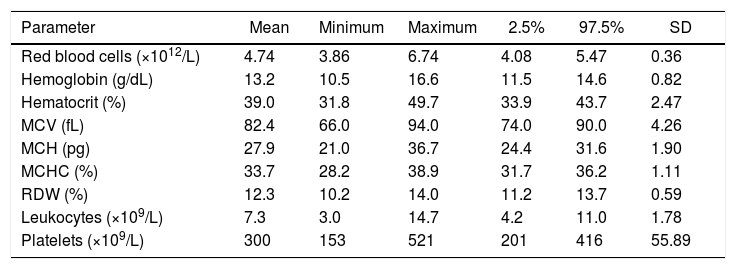
ResultsTable 1 describes the hematological parameters of the 409 children.
Complete blood counts of 409 children studying in municipal schools of the metropolitan region of Curitiba, Brazil.
| Parameter | Mean | Minimum | Maximum | 2.5% | 97.5% | SD |
|---|---|---|---|---|---|---|
| Red blood cells (×1012/L) | 4.74 | 3.86 | 6.74 | 4.08 | 5.47 | 0.36 |
| Hemoglobin (g/dL) | 13.2 | 10.5 | 16.6 | 11.5 | 14.6 | 0.82 |
| Hematocrit (%) | 39.0 | 31.8 | 49.7 | 33.9 | 43.7 | 2.47 |
| MCV (fL) | 82.4 | 66.0 | 94.0 | 74.0 | 90.0 | 4.26 |
| MCH (pg) | 27.9 | 21.0 | 36.7 | 24.4 | 31.6 | 1.90 |
| MCHC (%) | 33.7 | 28.2 | 38.9 | 31.7 | 36.2 | 1.11 |
| RDW (%) | 12.3 | 10.2 | 14.0 | 11.2 | 13.7 | 0.59 |
| Leukocytes (×109/L) | 7.3 | 3.0 | 14.7 | 4.2 | 11.0 | 1.78 |
| Platelets (×109/L) | 300 | 153 | 521 | 201 | 416 | 55.89 |
MCV: mean corpuscular volume; MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration; RDW: red cell distribution width or index of anisocytosis; SD: standard deviation.
The prevalence of anemia in the studied children was 2.20% (9/409), but none had severe anemia. There was no significant difference between genders.
Regarding the red blood cell count, 1.2% of the children (5/409) had values lower than the reference values (4.0–5.2×1012/L). On the other hand, 10.2% of the children (44/409) had counts above the upper limit.
Thirty-seven children (9.04%) had microcytosis (mean corpuscular volume <77.0fL). There were no cases of macrocytosis. Hypochromia was observed in 23 children (5.62%), characterized by mean corpuscular hemoglobin values <25.0pg. Hypochromia and microcytosis were found in 5.4% (22/409) of the children with one having an Hb value of <11.5g/dL (10.8g/dL).
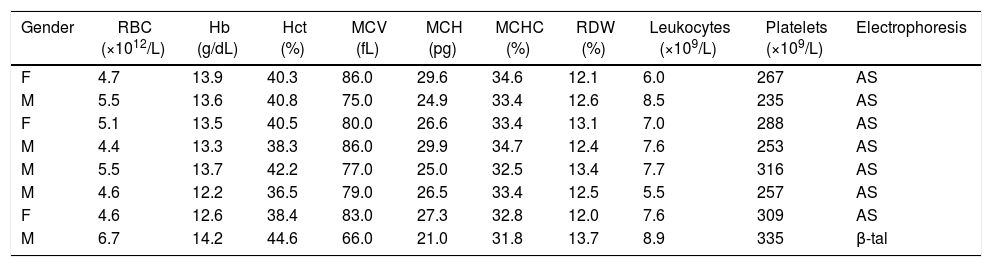
Screening by qualitative Hb electrophoresis at alkaline pH identified seven cases (1.7%) with sickle cell trait (Hb AS) all of which were confirmed using the solubility test and one case had β thalassemia trait, confirmed by a 4.8% Hb fraction using the elution method. Table 2 presents the hematological parameters of the eight children with altered electrophoretic patterns.
Results of complete blood count and qualitative hemoglobin electrophoresis of eight children with altered electrophoretic patterns.
| Gender | RBC (×1012/L) | Hb (g/dL) | Hct (%) | MCV (fL) | MCH (pg) | MCHC (%) | RDW (%) | Leukocytes (×109/L) | Platelets (×109/L) | Electrophoresis |
|---|---|---|---|---|---|---|---|---|---|---|
| F | 4.7 | 13.9 | 40.3 | 86.0 | 29.6 | 34.6 | 12.1 | 6.0 | 267 | AS |
| M | 5.5 | 13.6 | 40.8 | 75.0 | 24.9 | 33.4 | 12.6 | 8.5 | 235 | AS |
| F | 5.1 | 13.5 | 40.5 | 80.0 | 26.6 | 33.4 | 13.1 | 7.0 | 288 | AS |
| M | 4.4 | 13.3 | 38.3 | 86.0 | 29.9 | 34.7 | 12.4 | 7.6 | 253 | AS |
| M | 5.5 | 13.7 | 42.2 | 77.0 | 25.0 | 32.5 | 13.4 | 7.7 | 316 | AS |
| M | 4.6 | 12.2 | 36.5 | 79.0 | 26.5 | 33.4 | 12.5 | 5.5 | 257 | AS |
| F | 4.6 | 12.6 | 38.4 | 83.0 | 27.3 | 32.8 | 12.0 | 7.6 | 309 | AS |
| M | 6.7 | 14.2 | 44.6 | 66.0 | 21.0 | 31.8 | 13.7 | 8.9 | 335 | β-tal |
RBC: red blood cell count; Hb: hemoglobin; Hct: hematocrit; MCV: mean corpuscular volume; MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration; RDW: red cell distribution width or index of anisocytosis; F: female; M: male.
Anemia is one of the biggest public health problems in Brazil and the world. The prevalence of anemia in developing countries affects up to 50% of children, especially those in poorer neighborhoods and school-aged children.1 Iron deficiency is the most common cause of anemia in children; this may reflect an imbalance between the amounts of iron consumed and absorbed or loss of iron reserve, resulting to inadequate synthesis of Hb.1,3,4,10 This condition is very important because iron is required for the complete myelination of the sensory neurons, which are correlated to behavior and learning.11,12 Physiological damage from iron deficiency includes poor cognitive development, reduced psychomotor skills, and decreased immunity, which may lead to increased susceptibility to infections.4,12
Due to the influence of anemia on public health, the WHO proposed a classification based on the estimated prevalence of anemia. Severe prevalence refers to anemia in >40% of the population. Between 20% and 39.9% of anemia, the prevalence is considered moderate, while from 5.0 to 19.9% and <5.0% are classified as mild and normal prevalences, respectively.1 The prevalence of anemia found in this study (2.20%) corresponds to normal values according to the WHO classification. These data differ from higher prevalences observed in population surveys conducted in several regions of Brazil. A study of 754 children aged 0–12 years in Santa Maria reported a 29.17% prevalence of anemia.13 Santos et al.14 conducted a study with students (6–10 years) of public schools in Maceió and found a 9.9% prevalence of anemia. Another study conducted by Miglioranza et al.15 in the same region as this present work found a 41.3% prevalence of anemia in children and adolescents (n=526) aged 7–14 years using Hb <12.0g/dL as the main criterion. In Brazil, there is no national survey on the prevalence of anemia, only regional studies, which report variable prevalences of anemia depending on the region and socioeconomic conditions of the analyzed population.
The rate of malnutrition has improved considerably in recent decades; however, the prevalence of anemia is still high in populations on diets containing little iron, in patients with considerable blood loss and in those affected by intestinal parasites.1,8,12,16 These situations are common in childhood, where an increased nutritional need is observed, especially in under two-year-old children and those from the lower social classes. This condition probably lasts until school age, as anemia decreases with age.11,16,17 The socioeconomic situation of the population has been reported as the determining factor for the high prevalence of anemia in children and adolescents. The presence of anemia in children from low-income families is associated with low consumption of foods rich in iron, which is aggravated by the increased organic demand of minerals in this age group. In addition, precarious sanitation and housing conditions, and parasitic infections contribute to the occurrence of anemia.6,16–18 Although the population analyzed in this study resides in poor neighborhoods, the low prevalence of anemia found in this group indicates that lower socioeconomic conditions may not be a determining factor for anemia.
National policies have been implemented to meet the nutritional needs of the population and to increase the intake of micronutrients, such as iron. The “National Program for the Supplementation of Iron and Folic Acid” using wheat and cornmeal implemented by the Ministry of Health in 1999 and, the “National School Meals Program” implemented by the Ministry of Education in 1955 are examples of national policies that may contribute to the prevention of iron deficiency.16,19,20
In this study, hematological reference values were established. Data analysis showed a higher mean Hb value of 13.2g/dL (range: 11.5–14.6g/dL) than those reported in other studies.17,19,21 Heijblom and Santos19 in Brasília found an Hb reference value of 12.6g/dL in children aged from 6 to 11 years (n=424), without gender distinction. In the city of São Paulo, the reference value of Hb was 12.1g/dL for female and 12.2g/dL for male schoolchildren (n=86) aged 7–15 years.21 In Salvador, a study conducted by Borges et al. found an Hb value of 12.2g/dL (7–14 years old) for both genders (n=1013).17 Variances are related to diet, ethnicity, gender and the age of the different populations. The hematological profile in the different regions of the country should be evaluated to trace the prevalence of anemia, aiming to contribute with epidemiological data and, thus, to assist future interventions or prevention policies.6,8,20,22
Similar to this study, statistical differences were not observed between the genders in other studies.15,16,19,21 Testosterone causes significant statistical differences in relation to hematocrit and Hb values in the 15- to 50-year age group. Differences attributed to hormones are not observed in under 15-year olds and over 50-year olds.23
Hereditary anemia represents 1–2% of heterozygotes of Hb S and 3% of β thalassemia, constituting the most prevalent hereditary diseases worldwide.9,24 In this study, Hb electrophoresis showed that 1.7% of the children had the sickle cell trait (Hb AS); the children with the sickle cell trait had normal Hb values. In general, patients with the sickle cell trait are asymptomatic and their hematimetric indices are within normal limits. Hb AS individuals do not develop sickle cell anemia; however, genetic counseling on the awareness of the autosomal recessive inheritance of anemia should be conducted.7,9 In one case, β thalassemia was suspected based on a red blood cell count above the reference value, microcytosis, hypochromia, and the presence of basophilic stippling seen in a blood smear. This case was diagnosed as β thalassemia trait based on Hb A2 levels >3.5%.9,24,25
The differential diagnosis of anemia is complex, and its laboratory investigation is costly. Screening tests, such as Hb electrophoresis, are important to show the altered protein fractions. The use of hematimetric indices in diagnosing anemia may help in the initial investigation, because testing is fast, effective and low-cost.2,5,26,27 However, the use of the CBC alone is not sensitive or specific enough for the definitive diagnosis and complementary tests are necessary to clarify the hematological status.25,27,28
Diagnosing iron-deficiency anemia first requires confirmation of iron deficiency so that the cause or etiology can be determined. The onset of anemia is the last of a series of steps in which severe iron deficiency affects the concentration of Hb. In most cases, this phase is diagnosed by the presence of microcytic hypochromic anemia and biochemical evidence using standard biochemical markers, such as the transferrin (transport), transferrin receptor (use) and ferritin (storage) variables.5,25–28
Other tests, such as vitamin B12, folic acid, hemolysis markers, and reticulocyte counts, aid the elucidation and classification of anemia.3,10 The new hematological analyzers, in addition to providing automated reticulocyte counts, evaluate other reticulocyte parameters, such as Hb content and immature reticulocyte fractions, which are early markers of erythropoiesis.10,29
More studies should be performed to evaluate the profile of the general population with a larger number of participants. This work highlights the need that each laboratory should establish its own reference values based on the population served in order to interpret the CBC correctly.
Using Hb concentration as a single criterion for anemia with insufficient data on the dietary or socioeconomic status of the participants may be a limitation of this study. Children included in the analysis probably come from backgrounds with better socioeconomic conditions compared to other regions of the country, and therefore, the study subjects may not be representative of the wider population.
ConclusionThis study showed a normal prevalence of anemia in children from public schools in the metropolitan region of Curitiba according to the WHO classification. Factors such as the diet and socioeconomic conditions may contribute to these findings. Preventive or therapeutic measures should be carried out for children with anemia to avoid or reduce the physiological damage caused by this condition.
Conflicts of interestThe authors declare no conflicts of interest.


