
The establishment of regional development poles in the State of Pernambuco, Brazil was characterized by industrial expansion and consequent concerns about the increase in the occurrence of diseases, specifically those having long latency periods, as is the case of Chronic Myeloid Leukemia.
MethodsThe study included 367 patients diagnosed with Chronic Myeloid Leukemia over a ten-year period at a reference treatment center. Records of patient charts and the TerraView software were used, respectively, for data collection and geographic mapping of the cases from the twelve established State development regions.
ResultsA total incidence of 3.4 cases per 100,000 inhabitants was found, with a predominance of the disease among males, a median age of 47 years, a mestizo ethnicity, with elementary schooling and residence in urban area. Microregional incidence varied, but there was no significant variation in numbers over the years, and no relevant socio-environmental determinants were identified.
ConclusionThe present study determined the incidence and characterized the spatial distribution of Chronic Myeloid Leukemia cases over a decade in a northeastern Brazilian state. The variation in the incidence rate by region of development is compatible with a homogeneous distribution of the cases. The work is a baseline study to be used for present and future analyses of the impact of the state economic development poles and the occurrence of this chronic malignant disease.
Chronic Myeloid Leukemia (CML) is a malignant hematological disease characterized by a clonal disturbance, which originates from a single abnormal hematopoietic stem cell line.1,2 The incidence of CML is approximately 1.5 cases per 100,000 inhabitants per year, with a predominance in men3 and a median age of 55 years at diagnosis.4 The etiology and role of genetic and environmental factors in CML are not fully understood. The hereditary predisposition does not seem to exist, nor do geographic or ethnic characteristics predisposing the development of the disease.4 The only well-characterized risk factor is the exposure to ionizing radiation.
In the State of Pernambuco, Brazil, the deployment of regional development poles was characterized by industrial expansion. Thus, there is concern about the consequences of this type of development and thus, the need for studies that establish a baseline for the existence of diseases, specifically chronic malignancies having long periods of latency. In Brazil, there are few data on the occurrence of CML, the distribution of cases and possible correlations with risk factors. The geographic mapping emerges in this context as a tool to assist professionals and scholars in the health field with epidemiological studies, as well as to construct thematic maps as useful instruments for spatial analysis of a specific disease.5
The Hemope Foundation is the primary public reference center for diagnosis and treatment of adult leukemia patients in Pernambuco, Brazil, which has an estimated population of nine million inhabitants. The objective of the present study was to determine the incidence and to characterize the spatial distribution of CML cases over a decade and throughout twelve state regional poles of development.
MethodsThis case series-type study was based on hospital demand and included patients over 18 years old of both sexes, diagnosed with CML from January 2004 to December 2015 at the Hemope Foundation in Recife, Brazil.
The study was approved by the Institutional Research Ethics Committee (No. 020/09). The variables studied included age, sex, ethnicity, schooling, professional occupation, exposure to toxic substances, distribution by area of residence and counties grouped in 12 development regions. Data were collected from patient charts and the information system of the Institution.
The occurrence rate of CML cases was calculated by development region of the State of Pernambuco and the Brazilian Institute of Geography and Statistics (IBGE) population-based 2010 census and estimates for 2015.6 The identification of the distribution frequency of CML cases was based on the codification for counties of the State of Pernambuco, provided by the IBGE. The results were expressed in absolute and relative values of the CML population coefficient per year and the data were stored and analyzed in the TerraView7 software for the compilation of the geographic maps.
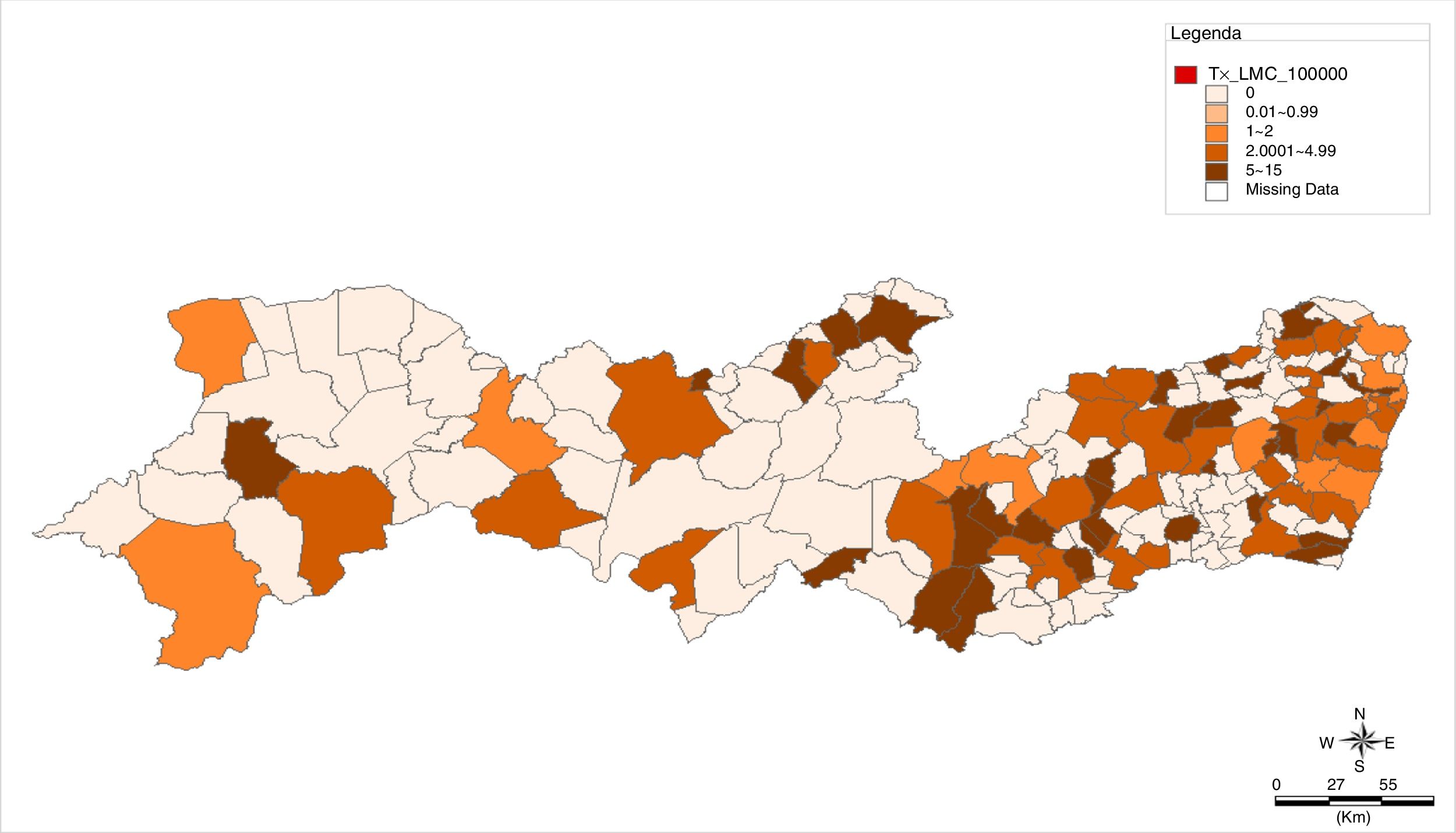
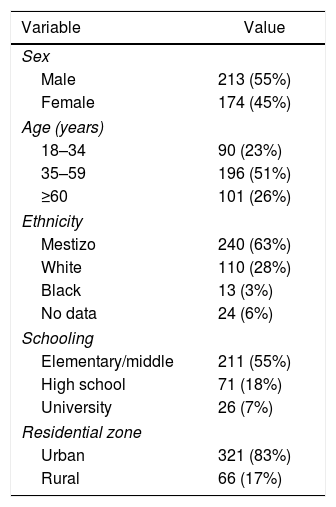
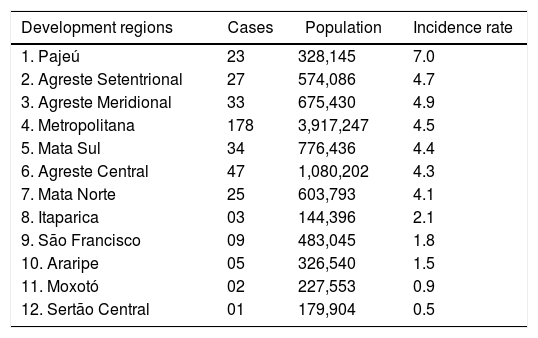
ResultsThe main sociodemographic variables of the CML cases analyzed are presented in Table 1. The incidence rate of 3.4 CML cases per 100,000 inhabitants per development region of the State of Pernambuco was found, showing variations among the microregions (Table 2). Figure 1 shows the spatial distribution of cases and incidence by microregion of the CML cases per 100,000 inhabitants.
Sociodemographic variables of 387 patients diagnosed with Chronic Myeloid Leukemia between January 2004 and December 2015 at the Hemope Foundation.
| Variable | Value |
|---|---|
| Sex | |
| Male | 213 (55%) |
| Female | 174 (45%) |
| Age (years) | |
| 18–34 | 90 (23%) |
| 35–59 | 196 (51%) |
| ≥60 | 101 (26%) |
| Ethnicity | |
| Mestizo | 240 (63%) |
| White | 110 (28%) |
| Black | 13 (3%) |
| No data | 24 (6%) |
| Schooling | |
| Elementary/middle | 211 (55%) |
| High school | 71 (18%) |
| University | 26 (7%) |
| Residential zone | |
| Urban | 321 (83%) |
| Rural | 66 (17%) |
Distribution and incidence rate per 100,000 inhabitants of 387 CML cases diagnosed between January 2004 and December 2015 at the Hemope Foundation.
| Development regions | Cases | Population | Incidence rate |
|---|---|---|---|
| 1. Pajeú | 23 | 328,145 | 7.0 |
| 2. Agreste Setentrional | 27 | 574,086 | 4.7 |
| 3. Agreste Meridional | 33 | 675,430 | 4.9 |
| 4. Metropolitana | 178 | 3,917,247 | 4.5 |
| 5. Mata Sul | 34 | 776,436 | 4.4 |
| 6. Agreste Central | 47 | 1,080,202 | 4.3 |
| 7. Mata Norte | 25 | 603,793 | 4.1 |
| 8. Itaparica | 03 | 144,396 | 2.1 |
| 9. São Francisco | 09 | 483,045 | 1.8 |
| 10. Araripe | 05 | 326,540 | 1.5 |
| 11. Moxotó | 02 | 227,553 | 0.9 |
| 12. Sertão Central | 01 | 179,904 | 0.5 |

The Hemope hospital receives around 40 new cases of CML per year, referred by the public and private health services. Based on data from the Hospital Registry of Cancer of the State Department of Health (Personal Communication), the number of cases reported in the present study is representative of the occurrence of CML in Pernambuco. This high level of recruitment may be due in part to the fact that the institution offers free treatment to patients, including those from the private sector.
The distribution of the patients by place of residence is similar to that of the population of the State of Pernambuco, with a predominance in the urban area. The variation in the incidence rate by development pole and county is compatible with a homogeneous distribution of CML cases in the State. Some regions had an even higher incidence of CML cases, compared to the average, however, there was no significant variation of this number over the years, and no relevant socioenvironmental determinants were identified.
The incidence of CML is low in young adults,8 increases at 40 years of age and has a peak occurrence between the ages of 55 and 60 years.9 The results of the present study, with a median age at diagnosis of 47 years and extremes of 18 and 93 years, confirm the increase of cases after 40 years, with a peak incidence between the ages of 40 and 50 years, previously described for Brazilian patients.10,11 In general, CML patients in developing countries are younger than those in developed countries.12 In this sense, the age of CML presentation seems to be determined by a complex interaction of factors such as ethnicity, life expectancy, country development and improvements in diagnostic capacity, but may also reflect genetic and environmental heterogeneity.
Epidemiological data on gender, ethnicity, schooling and occupational profile are essential for the evaluation of possible occupational exposures. In the present study, there was a slight predominance of male patients, in a proportion of 1.2:1, high miscegenation, low schooling and diversified occupation, which is in accordance with the general profile of the State population determined in the last IBGE demographic census. Theoretically, groups with low schooling would be more vulnerable, due to the precariousness in the identification of possible risk factors, however, the study type utilized does not allow for the determination of a causal relationship.
In CML, socioeconomic conditions were associated with lower survival.13 Nevertheless, income and education variables did not have an impact on the prognosis in countries with small socioeconomic disparities, regular access to health care, low drug costs and high adherence rates.14 A Brazilian study with 103 patients showed that a low education level impairs the achievement of a complete cytogenetic response, while income or distance from the home to the health service does not influence the same.11 These data show the need for additional health information to promote a better understanding by patients of the importance of their adherence to treatment, as the disease requires daily and rigorous use of oral medication. On the other hand, the ability to work proved to be an essential component in the quality-of-life of CML patients.15
A long exposure time to toxic substances, such as the occupational exposure in agriculture, was considered a potential etiologic factor for CML, however, no firm association was found.16,17 Similarly, a meta-analysis by Turner et al.18 observed a positive interaction between childhood leukemia and exposure to residential pesticides. Of the 387 patient charts analyzed, 94% did not present information on exposure to toxic substances, so the analysis of this variable was impaired. In the present study, the occupational profile of patients was also evaluated, however, a large part of medical records did not report this. The lack of data was noted in the patient charts of active workers, as well as in those of the unemployed and retired.
Only 10% of the patient records included data on exposure to industrial toxicants, which reinforces the need for qualified data/information for health surveillance, mainly diseases that are not part of the epidemiological surveillance system or have no tradition of notification, such as the hematologic, and that may be related to occupational or environmental risk conditions. The latter is related to the exposure of populations to pollution caused by productive processes in both urban and rural areas.
There is a need for greater awareness among professionals in the registering of patient data regarding situations of vulnerability, risks and injuries to improve the CML health information system. This interface between professional and public health service is essential in the recognition of, and response to, concerns about changes in the epidemiological profile of chronic diseases such as CML, in light of economic development scenarios.
Finally, the present study did not contemplate the analysis of possible clusters, however, the use of geographic mapping allowed for the visualization and analysis of the spatial distribution of cases in the context of the development of the economic regions in the State of Pernambuco.
ConclusionThe incidence rate of CML in Pernambuco was higher than expected. The collected data allowed for a geographic mapping of the spatial distribution of the disease over a decade. Both can be used as a baseline study for epidemiological monitoring and investigation.
Conflicts of interestThe authors declare no conflicts of interest.


