

Diversity in Classical Hematology Research
More infoThe data on the pattern of primary hematologic malignancies in Bahrain is sparse, although previously published studies suggested rising trends in their incidence. This study aimed to compare with regional and world data and identify any changing trends.
MethodsA retrospective cross-sectional chart analysis study was done on all cases of primary hematologic malignancies of bone marrow origin of Bahraini nationals presenting during the 10-year period from January 2005 to December 2014 at the sole oncology referral center in Bahrain during the study period.
ResultsIn a total of 272 cases, the primary hematologic malignancies in decreasing order of frequency with respective median ages at diagnosis were: acute myeloid leukemia (AML; 26.1%, 39 years), acute lymphoblastic leukemia (ALL; 22.8%, 9 years), multiple myeloma (MM, 16.2%, 57 years), chronic myeloid leukemia (CML, 14%, 39.5 years), myelodysplastic syndromes (MDS; 12.5%, 56 years) and chronic lymphocytic leukemia (CLL; 5.5%, 65 years). The overall crude annual incidence rate of these malignancies was 4.8/105 population. Age-specific incidence rates were found to increase dramatically with age, except for ALL, for which it peaked in the pediatric age group. The age-standardized incidence rates (ASIRs) per 105 per year were 1.47 (AML), 1.13 (MM), 0.93 (ALL), 0.85 (MDS), 0.81 (CML) and 0.44 (CLL).
ConclusionThe pattern of primary hematologic malignancies in Bahrain shows unique features that distinguish it from trends reported in Eastern and Western world populations. Compared to previously published reports, ASIR trends decreased in CML and ALL but increased in MDS and MM.
Hematologic malignancies are a heterogenous group of disorders that are distinguished from each other, not only by the cell of origin, but also by variations in their incidence, pathogenesis and clinical course. The Salmaniya Medical Complex (SMC) was the sole referral oncology center in the country during the present study period. To the best of our knowledge, there is only one published report from this center describing the incidence of hematologic malignancies in Bahrain.1 That study suggested a three-fold increase in the incidence of these neoplasms between 1986 and 1995. This and other published studies from Bahrain documented rising trends in the overall incidence of cancer, including hematologic malignancies.1-3 Therefore, the present study was carried out to compare the incidence and demographic characteristics of these neoplasms with previously published data from Bahrain, to identify any changing trend and to compare the emerging pattern with the regional and world data.
MethodsStudy design and data collectionThis was a retrospective descriptive cross-sectional chart review of all cases of primary hematopoietic cell neoplasms in bone marrow aspirates that presented during the 10-year period from January 2005 to December 2014 at SMC. Data were extracted from archived marrow biopsy reports. Demographic and laboratory data were accessed from archived records in the hospital information system. The diagnosis was based on morphology, flowcytometry and molecular analysis. Bahrain population statistics were accessed in the Bahrain open data portal.
Study subjectsInclusion criteriaAll Bahraini patients diagnosed with a primary hematologic malignancy in the bone marrow at the first presentation during the period from January 2005 to December 2014 were included.
Exclusion criteriaNon-Bahraini patients diagnosed with a primary hematologic malignancy were excluded. In addition, cases of nodal lymphomas, cases of follow-up marrow aspirates of hematologic neoplasia and cases of malignancies with metastatic secondary marrow involvement were excluded from the study.
Statistical analysisThe crude incidence rate, age-specific incidence rates and age-standardized incidence rates (ASIRs) were calculated. The crude incidence rate was calculated based on the mid-time of the total Bahraini population denominator for the period of 2005 to 2014. The age-specific incidence rate was calculated by dividing the total number of new primary hematologic malignancy cases diagnosed in the study period by the at-risk population for each age-group and multiplied by 100,000 of the population. The World Standard Population (WHO 2000 - 2025) was used for direct standardization to calculate ASIRs per 100,000 of the population. The ASIRs were calculated according to the Cancer Incidence in Five Continents series, published by the International Agency for Research on Cancer and the International Association of Cancer Registries.4
Ethical approvalThe study was approved by the respective research ethics committees of the participating institutions. Patient identifiers were anonymized prior to the data analysis.
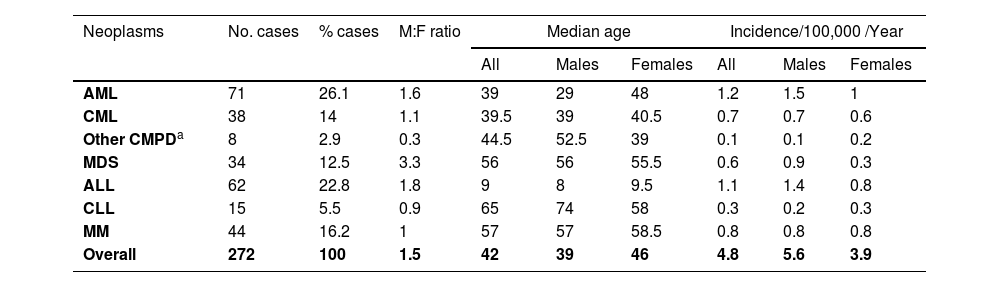
ResultsDemographic characteristics of the study population and the crude incidence rates of primary hematologic malignanciesA total of 272 new primary hematologic malignancy cases were diagnosed during the 10-year period of which 161 (59.2%) were males and 111 (40.8%) were females. The median age of the study population was 42 years (95% CI 38 - 48). The median age of males and females were 39 years (95% CI 34 - 49) and 46 years (95% CI 41 - 52), respectively (Table 1). There was no statistically significant difference between the median ages of males and females in the study population. Acute myeloid leukemia (AML) was the most frequently reported hematologic malignancy in our study (26.1%), with a median age of incidence of 39 years. Acute lymphoblastic leukemia (ALL) was the second most common reported type (22.8%, median age 9 years), followed by multiple myeloma (MM) (16.2%, median age 57 years), chronic myeloid leukemia (CML) (14%, median age 39.5 years), myelodysplastic syndrome (MDS) (12.5%, median age 56 years) and chronic lymphocytic leukemia (CLL) (5.5%, median age 65 years) in reducing order of frequency (Table 1). In addition, eight cases of other chronic myeloproliferative disorders (CMPD) were reported, including primary myelofibrosis (n = 3), essential thrombocythemia (n = 3) and polycythemia vera (n = 2). Finally, two cases of hairy cell leukemia were seen: a 25-year-old female and a 42-year-old male.
Demographic characteristics of the study population and the crude incidence rates of primary hematologic malignancies by sub-type among Bahrainis (2005 - 2014).
| Neoplasms | No. cases | % cases | M:F ratio | Median age | Incidence/100,000 /Year | ||||
|---|---|---|---|---|---|---|---|---|---|
| All | Males | Females | All | Males | Females | ||||
| AML | 71 | 26.1 | 1.6 | 39 | 29 | 48 | 1.2 | 1.5 | 1 |
| CML | 38 | 14 | 1.1 | 39.5 | 39 | 40.5 | 0.7 | 0.7 | 0.6 |
| Other CMPDa | 8 | 2.9 | 0.3 | 44.5 | 52.5 | 39 | 0.1 | 0.1 | 0.2 |
| MDS | 34 | 12.5 | 3.3 | 56 | 56 | 55.5 | 0.6 | 0.9 | 0.3 |
| ALL | 62 | 22.8 | 1.8 | 9 | 8 | 9.5 | 1.1 | 1.4 | 0.8 |
| CLL | 15 | 5.5 | 0.9 | 65 | 74 | 58 | 0.3 | 0.2 | 0.3 |
| MM | 44 | 16.2 | 1 | 57 | 57 | 58.5 | 0.8 | 0.8 | 0.8 |
| Overall | 272 | 100 | 1.5 | 42 | 39 | 46 | 4.8 | 5.6 | 3.9 |
ALL: acute lymphocytic leukemia; AML: acute myeloid leukemia; CLL chronic lymphocytic leukemia; CML: chronic myeloid leukemia; CMPD: chronic myeloproliferative disorders; MDS: myelodysplastic syndromes; MM: multiple myeloma.
The overall average crude annual incidence rate of these malignancies for the study period was 4.8/105. The corresponding rates were 5.6 in males and 3.9 in females (Table 1). Considering specific categories of primary hematologic malignancies, the crude incidence rate of AML was the highest (1.2/105). This was followed by ALL, with a crude incidence rate of 1.1/105. The crude incidence rates for MM, CML and MDS were 0.8, 0.7 and 0.6 per 100,000 of the population, respectively. CLL was observed to have the lowest crude incidence rate (0.3/105), excluding other CMPD and hairy cell leukemia. The crude incidence rates were higher in males than in females for AML, ALL and MDS, whereas the rates, as well as the male/female ratios, were approximately equivalent in CML, CLL and MM (Table 1).
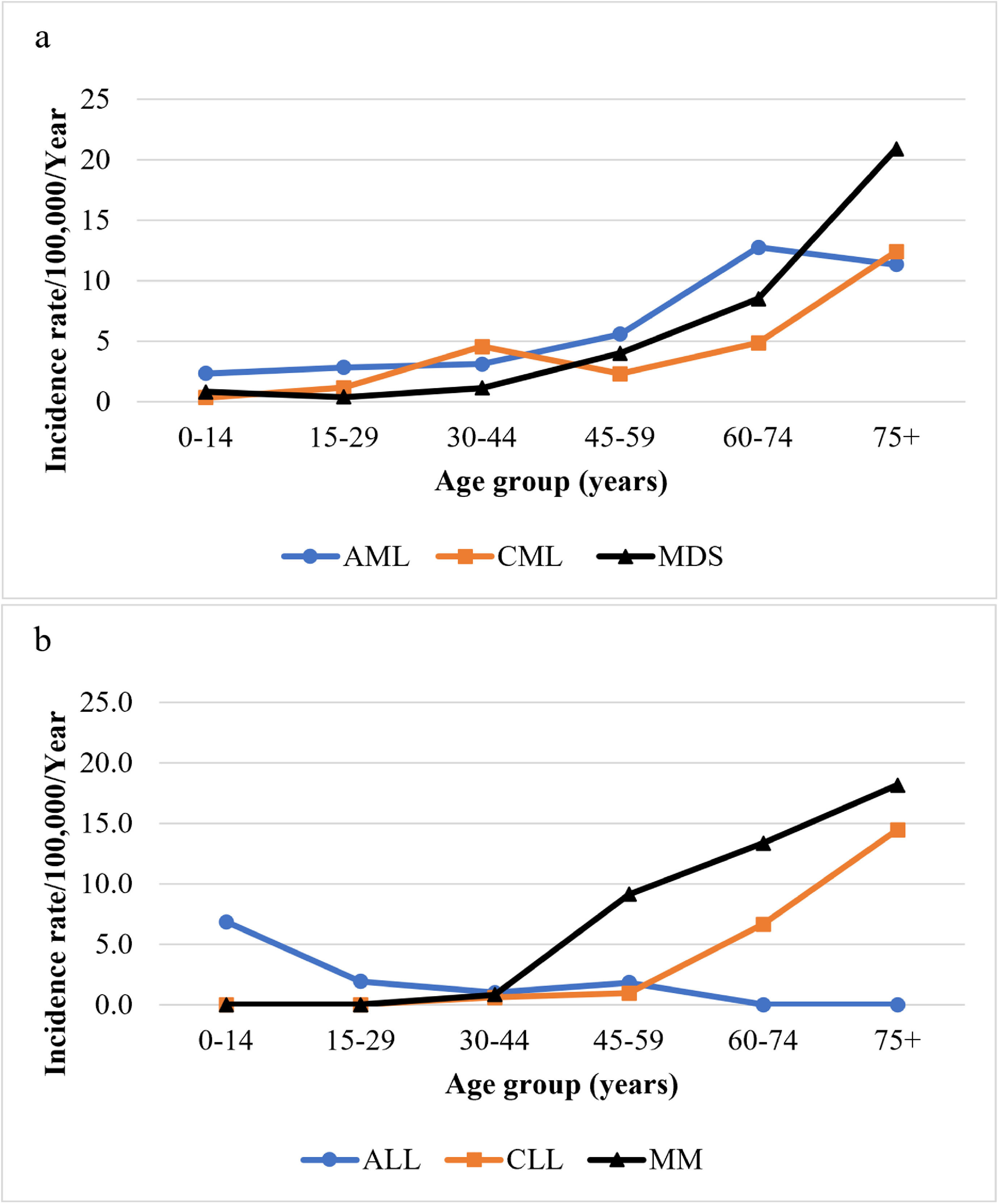
Age-specific incidence rates of primary hematologic malignanciesThe age-specific annual incidence rates per 100,000 of the population by age group for primary myeloid and lymphoid malignancies are illustrated in Figure 1a and b, respectively. The incidence of AML showed a peak at 60 to 74 years (12.8). The CML incidence rate was 4.6 at 30 to 44 years, declining at 45 to 59 years before increasing gradually, reaching 12.4 at 75+ years. The MDS rates increased sharply after the age of 59, reaching a maximum at 75+ years (20.9). The ALL was more common in childhood, with an incidence rate of 6.9 in the age group of 0 to 14 years (0 - 4 years: 3.13, 5 - 9 years: 2, 10 - 14 years: 1.72), whereas the CLL rose steeply from age 45-59 reaching a maximum at 75+ years (14.5). The age-specific incidence rates of MM rose steeply from age 30 to 44, reaching a peak at 75+ years (18.2).
 and primary lymphoid (b) malignancies among Bahrainis (2005 - 2014). ALL: acute lymphocytic leukemia; AML: acute myeloid leukemia; Incidence rate: age-specific incidence rate; CLL: chronic lymphocytic leukemia; CML: chronic myeloid leukemia; MDS: myelodysplastic syndromes; MM: multiple myeloma.")
Age-specific incidence rates per 100,000 per year for primary myeloid (a) and primary lymphoid (b) malignancies among Bahrainis (2005 - 2014).
ALL: acute lymphocytic leukemia; AML: acute myeloid leukemia; Incidence rate: age-specific incidence rate; CLL: chronic lymphocytic leukemia; CML: chronic myeloid leukemia; MDS: myelodysplastic syndromes; MM: multiple myeloma.
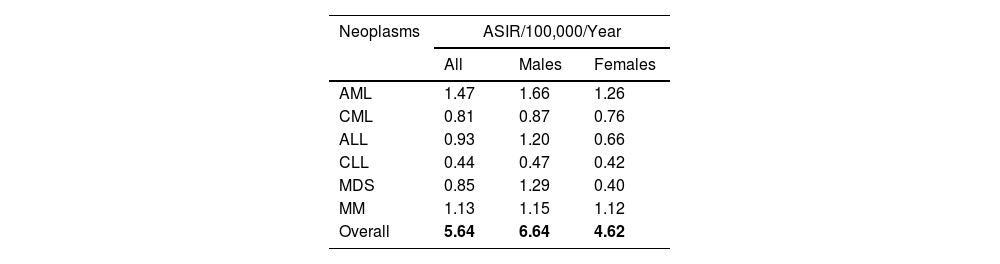
The ASIRs (world) per 100,000 of the population per year of primary hematologic malignancies were calculated for males, females and both sexes to overcome the age effect and allow comparisons between different populations (Table 2). The overall ASIRs for both sexes were 1.47,1.13, 0.93, 0.85, 0.81 and 0.44 for AML, MM, ALL, MDS, CML and CLL, respectively. When incidences in males and females were compared, notable male predominance was observed in MDS and ALL with male/female ratios of 3.2 and 1.8, respectively.
Age-standardized incidence rates (world) for primary hematologic malignancies by sub-type among Bahrainis (2005 - 2014).
| Neoplasms | ASIR/100,000/Year | ||
|---|---|---|---|
| All | Males | Females | |
| AML | 1.47 | 1.66 | 1.26 |
| CML | 0.81 | 0.87 | 0.76 |
| ALL | 0.93 | 1.20 | 0.66 |
| CLL | 0.44 | 0.47 | 0.42 |
| MDS | 0.85 | 1.29 | 0.40 |
| MM | 1.13 | 1.15 | 1.12 |
| Overall | 5.64 | 6.64 | 4.62 |
ALL: acute lymphocytic leukemia; AML: acute myeloid leukemia; ASIR: age-standardized incidence rate; CLL: chronic lymphocytic leukemia; CML: chronic myeloid leukemia; MDS: myelodysplastic syndromes; MM: multiple myeloma.
In the present study, the variation in the crude incidence, median age of diagnosis, age-specific incidence and ASIRs of the various types of hematologic malignancies broadly followed patterns described worldwide. However, there were notable variations in some specific characteristics of these neoplasms, compared to other geographic regions, as described below.
LeukemiaFrequencies of sub-typesThe AML comprised almost a quarter of all cases and was the most common primary hematologic malignancy reported in our study, followed by ALL and CML. The CLL contributed a small minority of cases. There is very limited incidence data on specific leukemia types in the Middle East region. According to one report, ALL was the most commonly reported type of leukemia (26%), followed by AML (20%) during the period of 1998 to 2007.5 Similar distributions are reported in Asian countries.6 In sharp contrast, CLL is one of the most commonly reported primary hematologic malignancies in Western developed countries. Remarkably, in the UK, it comprised as much as half of all cases of leukemia in 2015 and was by far the most common leukemia type.7 In the US, CLL constituted 27% of all leukemia cases.8 In both countries, AML comprises one-third of all the leukemia cases.7,8 The crude-incidence rates and the ASIRs of AML and ALL were found to be higher in males than in females and are consistent with those of previous reports. 7,9-11
Age relationshipsIn AML, the median ages of patients vary widely across different countries: 30 to 35 years in South Asia and 39 years in our patients, compared to 67 years in the US.6 Similarly, several studies consistently show that CML patients in Asia are younger, compared to their Western counterparts.6 A large study of CML patients in India during the period of 2002 to 2008 reported median ages of 36 to 40 years in different income groups.12 This is comparable to our data (median age 39.5 years). In contrast, the median age of CML patients in the US is around 66 years 13 and in Europe, between 57 and 60 years.14 The finding of a later age of incidence in higher income groups may be true in India, but this cannot be generalized to other regions, such as Bahrain, where other factors are likely responsible for the lower age at diagnosis. A similar, but less prominent age difference between the two regions, was also observed in CLL, in which median ages are around 60 years in the developing countries and around 70 years in developed Western countries.6,15 In contrast, in ALL, median ages in Bangladesh and India are higher (27 and 23 years, respectively) compared to the US (11 years).6,16 In both the present and previously reported studies from our center, a very low median age in ALL is consistently seen (9 and 6 years, respectively).1 The peak incidence of ALL in very young children (< 5 years in age) was observed in our study, as well as in Kuwait, and could be a regional phenomenon.17
The age-specific incidence rate trends of CLL, AML and CML are consistent with previous studies, in which leukemia incidence rates were found to increase dramatically with age.11,13,18,19 The age-specific incidence rates in CLL rise steeply from around age 45 to 59 years and the highest rates are in the 75+ age group. In the US and the UK, similar trends were observed.20,21 In the UK, the age-specific incidence rates reveal that in AML the rates rise gradually from 50 to 54 years.20 In the US, age-specific rates in males and females combined, were < 3/105 in age groups < 50 years, rising steeply thereafter with a peak of 24/105 at 80 to 84 years.21 In our population, rates are consistently higher in younger patients. Also, the curve shows the upward trend earlier from 30 to 44 years, but is less steep than in the US, reaching a peak of 12.8 at 60 to 74 years, i.e., almost half of the US rate (Figure 1). In CML, a steep rise in the age-specific rates after 74 years observed in our study is very similar to that in the West. In the US, rates almost doubled from 5.6 in the 70 to 74 years age group to 10.2 per 100,000 at > 85 years during the period of 2007 to 2011.21 The data from the UK shows similar trends, but with lower rates in general.20 In contrast to the general age trend in our study, the ALL incidence peaked in children 0 to 14 years of age and this is a well-known phenomenon.22 Within this age group, the age-specific incidence rate was the highest in children 0 to 4 years old. Similar trends were reported in the US and the UK.20,21
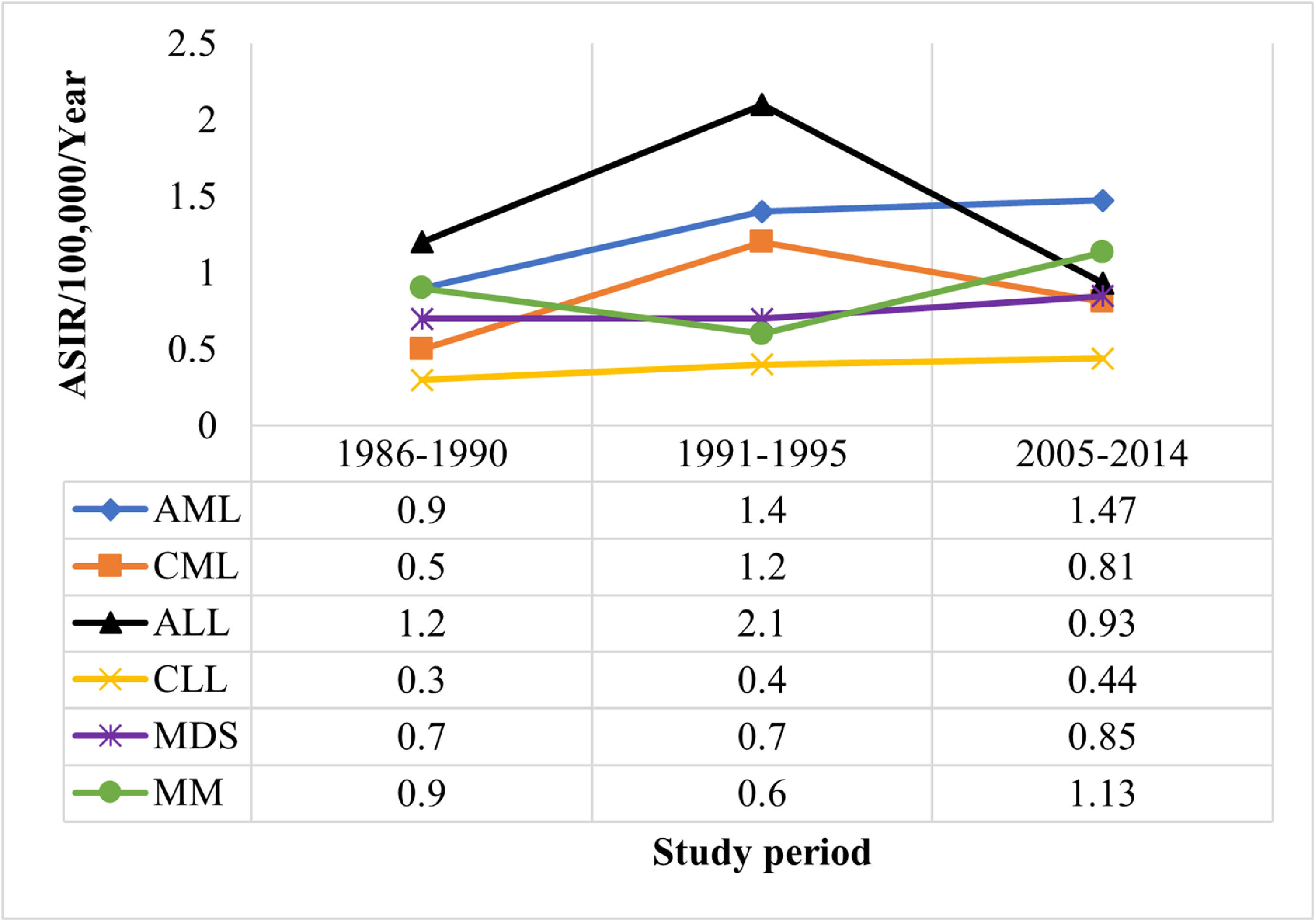
The ASIRs of leukemia were compared to published data of 1986 to 1990 and 1991 to 1995 in Bahrain (Figure 2).1 We observed decreasing trends of CML and ALL, compared to the 1991 to 1995 data, whereas no obvious changes in the trends of the ASIRs were observed for AML and CLL. Despite small case numbers, these observations in our study mirrored world trends. In ALL and CML, the ASIRs decreased in most countries between 1990 to 2017.23 The worldwide ASIRs of CML vary from 0.1 in sub-Saharan Africa to 1.78 in Western Europe and 0.81 in Korea and this suggests a direct relationship between the socio-demographic index and incidence.19,24 Although the AML ASIRs increased from the period (1986 - 1990) to (1991 - 1995), it plateaued after that (2005 - 2014). On one hand, the global trends of AML showed an increase in the ASIRs (from 1.35 to 1.54) between 1990 and 2017 in most countries, especially in Latin America, East Asia and Southeast Asia.23 On the other hand, decreasing trends in AML were reported in some countries in the Middle East and Europe.23 In the US, a rapid increase in the incidence rates of AML, especially in the period after 2011, was reported and it was positively correlated with the accelerated aging of the population.25
 per 100,000 of the population per year for primary hematological malignancies among Bahrainis, compared to data of 1986 to 1990 and 1991 to 1995 in Bahrain. ALL: acute lymphocytic leukemia; AML: acute myeloid leukemia; ASIR: age-standardized incidence rate; CLL: chronic lymphocytic leukemia; CML: chronic myeloid leukemia; MDS: myelodysplastic syndromes; MM: multiple myeloma.")
Age-standardized incidence rate (world) per 100,000 of the population per year for primary hematological malignancies among Bahrainis, compared to data of 1986 to 1990 and 1991 to 1995 in Bahrain.
ALL: acute lymphocytic leukemia; AML: acute myeloid leukemia; ASIR: age-standardized incidence rate; CLL: chronic lymphocytic leukemia; CML: chronic myeloid leukemia; MDS: myelodysplastic syndromes; MM: multiple myeloma.
The MDS were the fifth most common primary hematologic malignancy in Bahrain in our study. The male predominance of MDS was reported in most populations.4,26,27 The MDS are known to predominate in the elderly with a median age at diagnosis in the US of 76 years.27 In our study, relatively younger age groups were affected (median age at diagnosis was 56 years old), which is comparable to reports from Bangladesh (57 years) and Morocco (62 years). 6,28 The age-specific incidence rates for MDS increased with age, which is a well-known fact.26,27
The ASIR reported in our study is lower than those in the US and Germany (4.9), but more comparable to Eastern countries (e.g., Korea 1.1).19,21,26 In addition, we found that the ASIR of MDS is 3.2 times higher in males, compared to females. The male predominance was reported in the US (ASIR 1.8 times higher in males).21 The overall ASIR per 100,000 per year for MDS in our study (0.85) suggests an increasing trend, compared to the previous report in Bahrain (0.7) (Figure 2).1 Increasing trends of MDS over time were reported in the US and Europe and this might be attributed to the improved diagnosis and reporting of these malignancies. 27,29
Multiple myelomaThe MM was the third most common primary hematologic malignancy in our study. The crude annual incidence rate of 0.8 per 100,000 is comparable to that in other GCC countries, but much lower than the rates reported in the (6.3) and the UK (6.3).4,7,30 We found that males and females were equally affected and this is consistent with reports in the US and Saudi Arabia.4,8 However, higher male-to-female ratios are observed in other countries, such as the UK (ratio 1.43), Morocco (ratio 1.2) and Kuwait (ratio 1.8).4,7,28
The median age at diagnosis of our patients (57 years) is similar to the data reported in Asian countries.6 A higher median age at diagnosis is reported in the West (the UK and the USA: 68 - 73 years).7,31,32 The age-specific incidence rates of MM increased with age and this is a well-known trend.28,30,31
The annual ASIR of MM in our study is 1.8 times higher than in 1991 to 1995 at the same center (1.1 versus 0.6 per 105) (Figure 2). This apparent rise in the incidence of MM is consistent with the global trend that witnessed an increase of 126% during the period of 1990 to 2016 and may be attributed to the increase in the aging population and improvement in detection rates.33 However, our ASIRs are much lower than the global rates (2.1/105 in 2016) and reported ASIRs in Western Europe, North America and Australia, but comparable to rates in North Africa, the Middle-East and Asian countries.21,33
ConclusionsThis study describes the pattern and distribution of primary hematologic malignancies in the bone marrow in Bahrain. These neoplasms varied in the crude incidence, median age of diagnosis, age-specific incidence and ASIRs. AML was the most common reported primary hematologic malignancy, followed by ALL; whereas CLL was the least common type.
Consistent with previously published reports, male predominance was observed in AML, ALL and MDS. The median age of diagnosis for most of these malignancies was comparable to Eastern countries, but lower than what was observed in the West. However, the age-specific incidence rates were consistent with global trends: all incidence rates were found to increase dramatically with age, except for ALL, in which it peaked in the pediatric age group. A decreasing trend of the ASIRs of CML and ALL and increasing trend of the ASIRs of MDS and MM, compared to previous reports, were observed in Bahrain and this is in line with the global trends.
The limitations of our study should be noted. First, the limited number of hematologic malignancy cases in our study is due to Bahrain's small population. Second, our study was not based on cancer registry data; however, SMC was the only referral diagnostic oncology center for all hematologic malignancies in Bahrain during the study period. Therefore, the data are reliably pertinent to the population. Further studies are needed to understand the epidemiology and identify risk factors of these neoplasms for implementing tailored preventive strategies in this part of the world.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The contribution of Dr. Urmil Prabha Brahmi in collation and documentation of data is acknowledged.


