


Hemophilia is a coagulopathy caused by a deficiency in coagulation factors VIII (hemophilia A) or IX (hemophilia B). It is a chronic disease and, hence, impairs the quality of life (Qol) of the patients. This study aimed to evaluate the Qol of patients with hemophilia using the WHOQOL-bref and the Haemo-A-Qol instruments, its relation to the clinical condition and its sociodemographic variables.
MethodsThis is a cross-sectional, epidemiological study, comprising 17 patients with hemophilia, registered at the hemocenter, who met the eligibility criteria. Data were collected using three questionnaires: a semi-structured clinical evaluation form, the WHOQOL-bref and the Haem-A-Qol.
ResultsThe average age was 30 years old, and most participants declared themselves to be single (58.82%), without children (64.70%) and employed (58.82%). Hemophilia A was observed in 14 patients and the most severe form of the disease was more prevalent (64.70%). The average score of Qol, estimated by the WHOQOL-bref questionnaire was 74.3; being “social relations” the domain with the highest average. The Haem-A-Qol measured an average of 36.2 and the domain with the highest result was “Family Planning”.
ConclusionHemophilia had a higher negative impact upon the physical, sports and leisure features in the sample subjects. The analysis of the questionnaires did not reveal statistical agreement between them. Based on this, the Haem-A-Qol is considered the most recommended to evaluate the Qol, as it addresses factors more specifically related to the disease. No statistical significance was observed between the scores of Qol, as for the presence of comorbidities, gravity of the hemophilia and positive serology for infections.
Hemophilia is a coagulopathy in which there is a deficiency of factors VIII (hemophilia A) or IX (hemophilia B) of the coagulation. It is a congenital and genetic disease of recessive inheritance, linked to the X chromosome, resulting from mutations of the genes that codify factors VIII or IX of the coagulation.1 It happens almost exclusively in males, and the worldwide incidence is estimated at approximately 1/10,000 men born alive.3 Hemophilia A is the most frequent, being responsible for approximately 85% of the cases, while hemophilia B is responsible for the remaining cases.2,3 The main clinical symptoms are characterized by bleeding, occurring especially in regions where an impact occurred, such as joints (hemarthrosis), muscles, bones and central nervous system (bruises).3
Hemophilia is classified as mild, moderate or severe, according to the variation of two parameters: the antigenic level (Ag) or the coagulant activity (C) of the deficient coagulation factor, with the values <0.01 UI/mL and/or <1%, from 0.01 to 0.05 UI/mL and/or from 1 to 5%, and >0.05 to <0.04 UI/mL and/or >5% to <40%, respectively.4
The treatment of this condition consists in the replacement of the deficient coagulation factors by prophylaxis and a multidisciplinary follow-up.5 The therapeutic option is defined considering the gravity of the disease, patient age, occurrence of hemarthrosis and development of inhibitors against the administered coagulation factor.6 Hemophilia has a great impact upon the quality of life of its carriers because of its chronicity, symptomatology and complications.
The World Health Organization (WHO) defines quality of life (Qol) as “the awareness of the individual of its position in life in the context of the culture and system of values in which he/she lives and in relation to his/her objectives, expectations, standards and concerns”.7 Hence, the importance of evaluating the Qol in patients with hemophilia is clear. Indicators of Qol could assist in clinical decision-making, considering the gravity of the symptomatologic manifestations, the possible complications of the treatment and the relationship between these symptoms and the daily life of the patient.7 In addition, it allows for the demonstration of the effectiveness of the implementation of multidisciplinary teams in the disease prognosis.8
The quality of life related to the health (QOLRH) may be influenced by factors such as the disease and its treatment, the manner in which the person copes with his/her problem and the access to care.9 In the case of hemophilia, the factors which stand out are: restrictions to physical activities, the concern about hemorrhages that may be life-threatening, the development of arthropathy, the need for orthopedic procedures and infectious diseases, vectorized by blood or hemoderivatives.10,11 However, few studies using validated questionnaires to evaluate the QOLRH have been performed. In Brazil, a small number of studies were performed, some of them using generic questionnaires, such as the WHOQOL-bref12 and the SF-36.9 Other studies have used specific questionnaires for patients with hemophilia.13–16
To better define the quality of life of patients with hemophilia, the WHOQOL-bref and Haemo-A-Qol instruments have been applied, and their relation to the clinical condition and its sociodemographic variables has been evaluated. In addition to evaluating the agreement between the two questionnaires and correlating the Qol scores, this considers the presence or absence of comorbidities and the gravity of the disease.
MethodsThis is an observational study, with a cross-sectional design performed at the Hemominas Foundation — Núcleo Regional de Divinópolis in Divinópolis, Minas Gerais, Brazil.
Patients with hemophilia registered at the Divinópolis regional unit, who met the following eligibility criteria were included: literate males, aged 18 or older, who showed confirmatory laboratory tests for hemophilia and who were under treatment at the Divinopolis unit. They were invited to join the study through telephone contacts and home visits. Data were collected using the specific questionnaire Haem-A-Qol, with express authorization from the Hemo-QolGroup, the WHO generic questionnaire WHOQOL-bref and by using a clinical record created to collect clinical and sociodemographic data, via interviews and medical records search.
The general questionnaire to evaluate the quality of life, the WHOQOL-bref, is comprised of 26 questions, two questions on the general quality of life (GQOL) and the remaining 24 with 5 options of answers, comprising 4 domains: physical, psychological, social relations and environment.
The GQOL of the WHOQOL-bref questionnaire is obtained from the average of the first two questions scores. The first (Q1) evaluates the quality of life in a general spectrum and the second (Q2), the satisfaction of the individual with his/her health. The Qol is evaluated by transforming the score into a scale varying from 0 to 100, in which the higher the score, the better the Qol index.17
The specific questionnaire Haem-A-Qol is comprised of 46 items, divided into 10 domains (physical health, feeling, self-awareness, leisure and sports, work and school, dealing, treatment, future, family planning and relationship/sexuality18) and the Qol is evaluated transforming the score of each category into scales ranging from 0 to 100, with 0 as the best index and 100, the worst.14,15 This questionnaire was translated to the Portuguese language and validated transculturally.19,20
Results obtained were analyzed by the SPSS (Version 19). All selected individuals (17) were divided into two groups according to the gravity of the disease, categorized as mild/moderate or severe. The comparison was made using the non-parametric test of Mann–Whitney U. Normality was tested by the Kolmogorov–Smirnov test. The significance level was established at <0.05. To establish internal consistency, the reliability analysis was performed by determining Cronbach’s alpha. Furthermore, to evaluate the agreement between the instruments, the Bland–Altman’s method was used, with a dispersion chart showing the difference between the two variables and the average of the same (Figures 1 and 2).


The present study was submitted and approved by the Ethics Committee in Research in Human Beings at the Universidade Federal de São João del Rei — Campus Centro-Oeste (CEP CCO), statement number 818.093 and by the Ethics Committee and Research at the Hemominas Foundation, located in Belo Horizonte, Minas Gerais, Brazil, statement number 1.053.743.
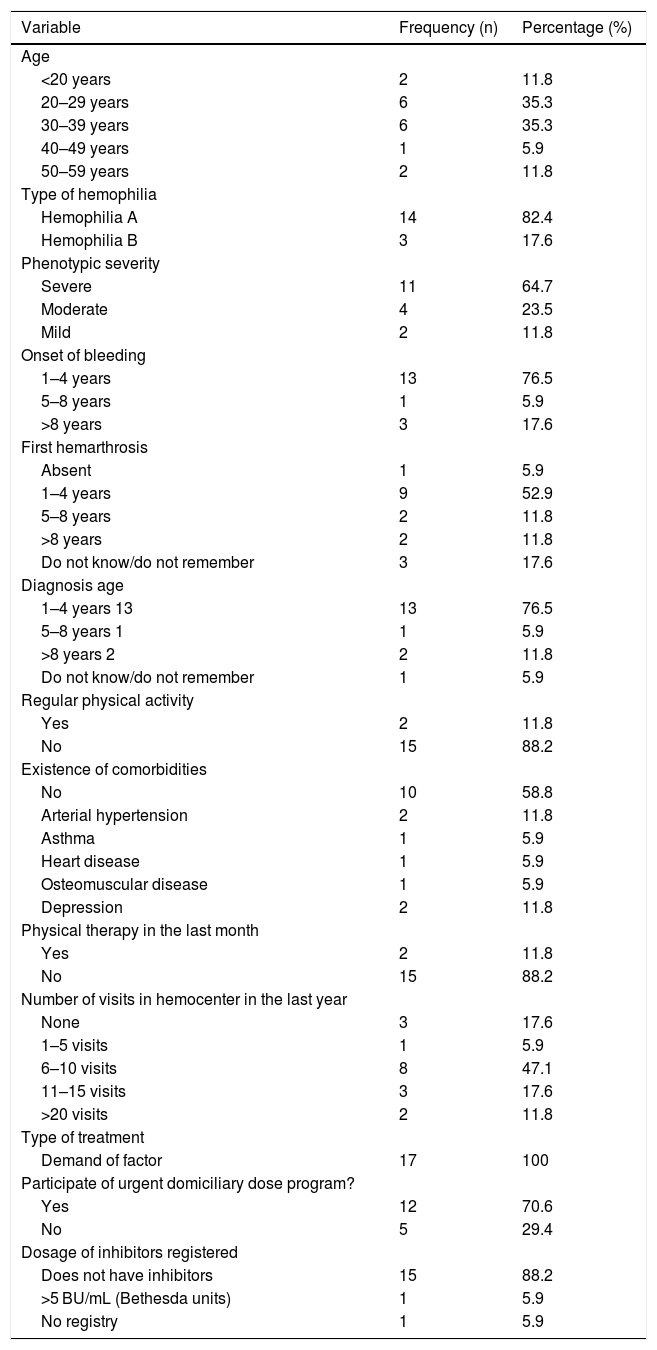
ResultsFrom the 19 eligible patients, 17 were interviewed, from August to October of 2015, representing 94.4% of the total. Two patients were not interviewed, as they were not found. The most frequent age group was 26–35 years old (35.6%), and the majority of patients declared themselves to be white (64.7%), single (58.8%), not having children (64.7%), employed (58.8%), having an average household income between one and two Brazilian minimum wages and not receiving any government financial help (52.9%). The patient clinical aspects are presented in Table 1A.
Socioeconomic, demographic and clinical characteristics of patients with Hemophilia treated at the Regional Blood Center of Divinopolis.
| Variable | Frequency (n) | Percentage (%) |
|---|---|---|
| Age | ||
| <20 years | 2 | 11.8 |
| 20–29 years | 6 | 35.3 |
| 30–39 years | 6 | 35.3 |
| 40–49 years | 1 | 5.9 |
| 50–59 years | 2 | 11.8 |
| Type of hemophilia | ||
| Hemophilia A | 14 | 82.4 |
| Hemophilia B | 3 | 17.6 |
| Phenotypic severity | ||
| Severe | 11 | 64.7 |
| Moderate | 4 | 23.5 |
| Mild | 2 | 11.8 |
| Onset of bleeding | ||
| 1–4 years | 13 | 76.5 |
| 5–8 years | 1 | 5.9 |
| >8 years | 3 | 17.6 |
| First hemarthrosis | ||
| Absent | 1 | 5.9 |
| 1–4 years | 9 | 52.9 |
| 5–8 years | 2 | 11.8 |
| >8 years | 2 | 11.8 |
| Do not know/do not remember | 3 | 17.6 |
| Diagnosis age | ||
| 1–4 years 13 | 13 | 76.5 |
| 5–8 years 1 | 1 | 5.9 |
| >8 years 2 | 2 | 11.8 |
| Do not know/do not remember | 1 | 5.9 |
| Regular physical activity | ||
| Yes | 2 | 11.8 |
| No | 15 | 88.2 |
| Existence of comorbidities | ||
| No | 10 | 58.8 |
| Arterial hypertension | 2 | 11.8 |
| Asthma | 1 | 5.9 |
| Heart disease | 1 | 5.9 |
| Osteomuscular disease | 1 | 5.9 |
| Depression | 2 | 11.8 |
| Physical therapy in the last month | ||
| Yes | 2 | 11.8 |
| No | 15 | 88.2 |
| Number of visits in hemocenter in the last year | ||
| None | 3 | 17.6 |
| 1–5 visits | 1 | 5.9 |
| 6–10 visits | 8 | 47.1 |
| 11–15 visits | 3 | 17.6 |
| >20 visits | 2 | 11.8 |
| Type of treatment | ||
| Demand of factor | 17 | 100 |
| Participate of urgent domiciliary dose program? | ||
| Yes | 12 | 70.6 |
| No | 5 | 29.4 |
| Dosage of inhibitors registered | ||
| Does not have inhibitors | 15 | 88.2 |
| >5 BU/mL (Bethesda units) | 1 | 5.9 |
| No registry | 1 | 5.9 |
However, it was not possible to evaluate the correlation between the quality of life and joint impairments, as a specific questionnaire for assessing joint impairments, such as the Hemophilia Joint Health Score (HJHS) was not applied in this study21; only the incidence of the first hemarthrosis by age was investigated.
Statistical tests were conducted to measure the correlation between quality of life and the existence of comorbidities, as well as the hemophilia severity and infectious serologic results. However, there was no significant difference between the measured parameters.
Patients received between 6 and 10 visits from the hemocenter in the last year (47.1%). All patients received treatment by demand of factor, 12 (70.6%) were part of the Urgent Domiciliary Dose program (DDU) and 15 (88.2%) had a negative dosage for inhibitors, according to laboratory tests. These data are presented in Table 1A.
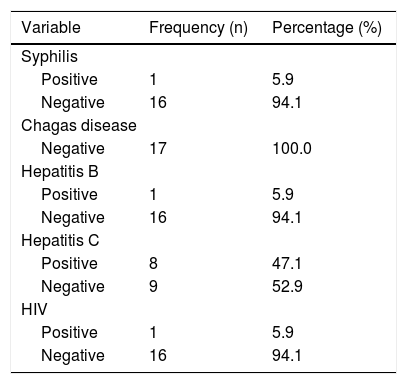
In relation to the serologic tests of the patients (Table 1B), all of them showed negative serology for Chagas disease. Serology for hepatitis C showed the highest positivity, with 8 cases (47.1%) and serologies for syphilis, hepatitis B and HIV showed 1 positive result each (5.9%).
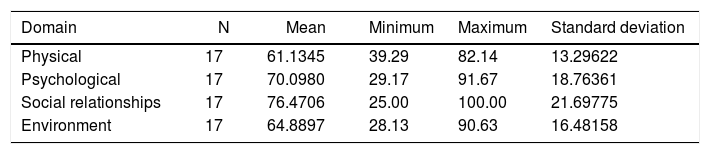
In the WHOQOL-bref questionnaire, the general quality of life was of 74, and the highest average score was obtained in the “Social Relations” domain, with an average of 76; the lowest was the “Physical” domain, with an average of 61.1 Table 2A shows average scores of the instruments evaluated in each domain.
The questionnaire Haem-A-Qol yielded an average score of 36.15 points and Cronbach’s alpha equaled 0.859. Among all ten areas evaluated, “Family Planning” yielded the best evaluation, followed by “Relationship and Sexuality”, with averages of 10.0 and 14.7, respectively. In contrast, the “Sports and Leisure” and “Physical Health” domains yielded the worst scores (averages of 66.35 and 47.94, respectively). Other domains had averages between 26.47 and 38.23. The “Coping” domain yielded the highest variability of answers, with a minimum score of 0.0 and a maximum, of 100.0. These results are shown in Table 2B.
Mean scores and internal consistency for dimensions of the Haem-A-Qol of patients with Hemophilia treated at the Regional Blood Center of Divinópolis.
| Dimension | N | Mean | Minimum | Maximum | Standard deviation | Cronbach’s alpha coefficient |
|---|---|---|---|---|---|---|
| Physical health | 17 | 47.9412 | 15.00 | 90.00 | 20.39139 | 0.802 |
| Feeling | 17 | 34.5588 | 0.00 | 75.00 | 23.29306 | 0.723 |
| View of yourself | 17 | 38.2353 | 10.00 | 70.00 | 17.76066 | 0.166 |
| Leisure and sports | 16 | 66.3542 | 10.00 | 95.00 | 23.34300 | 0.367 |
| Work and school | 13 | 33.0128 | 0.00 | 62.50 | 21.07235 | 0.742 |
| Dealing | 17 | 26.4706 | 0.00 | 100.00 | 26.06004 | 0.855 |
| Treatment | 17 | 32.4842 | 9.38 | 56.25 | 12.05619 | 0.111 |
| Future | 17 | 35.8824 | 0.00 | 70.00 | 21.00858 | 0.478 |
| Family planning | 15 | 10.0000 | 0.00 | 50.00 | 15.81139 | 0.838 |
| Relationships/sexuality | 17 | 14.7059 | 0.00 | 75.00 | 24.56733 | 0.925 |
| Total | 17 | 36.1504 | 21.20 | 62.50 | 12.69743 | 0.859 |
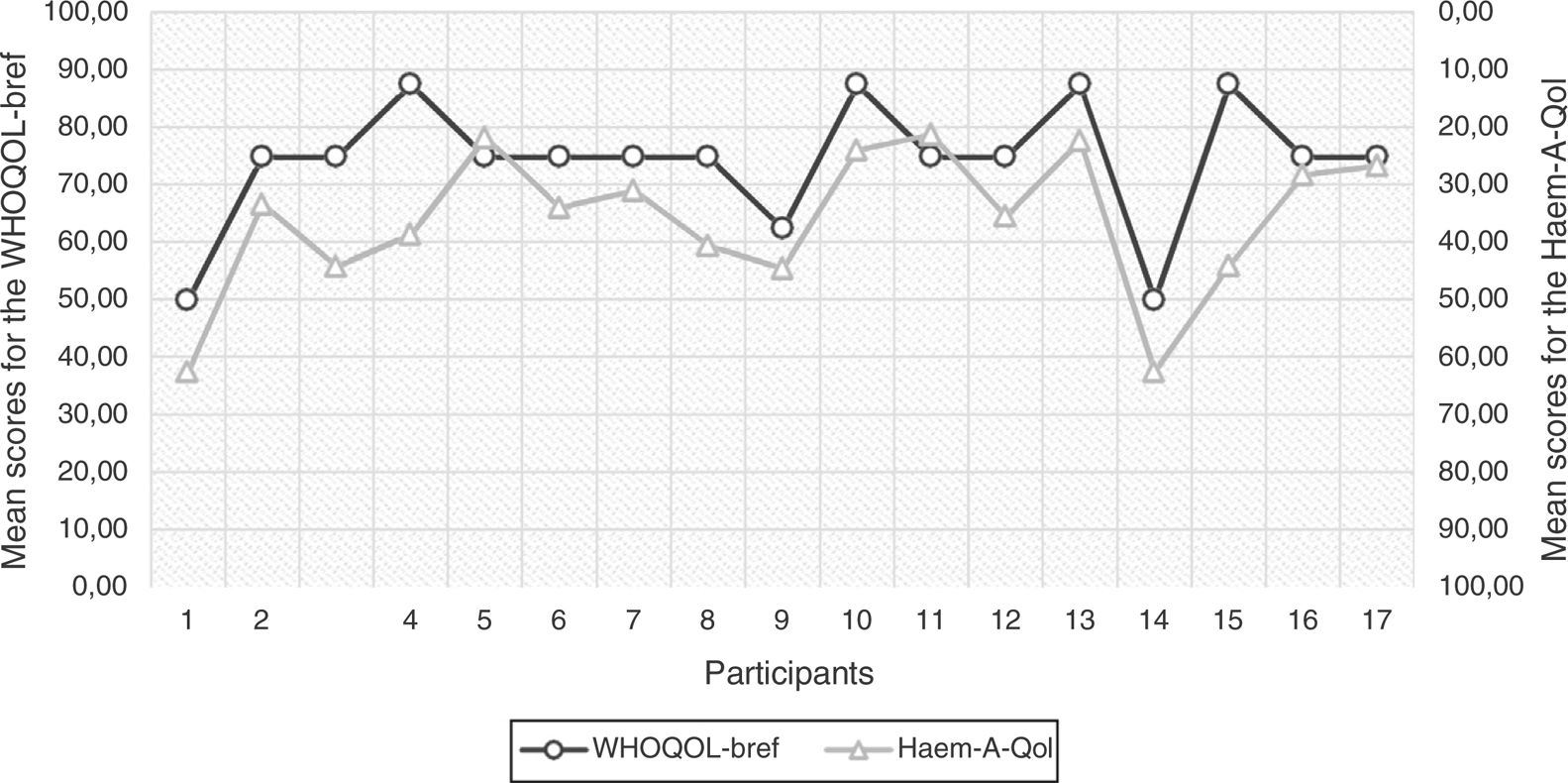
The general scores of the Qol obtained with the instruments WHOQOL-bref and Haem-A-Qol per individual are presented in Chart 1. In this chart, there is an inversion of the scale of the questionnaire Haem-A-Qol to allow for a comparison between the values. By analyzing this chart, a difference in the scores among the instruments for each individual can be clearly perceived.
In this manner, the agreement between the instruments was assessed by building a Bland-Altman’s plot chart (Chart 2) and no agreement between the questionnaires was verified, the upper limit, lower limit and bias values being 28.48, –7.65 and 10.41, respectively.
Scores for Qol were correlated with the presence or absence of comorbidities, gravity of the hemophilia and positive serology for infectious contagious diseases, although the results did not show statistical significance.
DiscussionOur results showed that the studied population was comprised, mainly by young adults, comparable to the data of Brazilian Ministry of Health in 2015.2 About half (52.9%) of the interviewed patients declared they did not receive financial support from the government, a result similar to that found by Ferreira14 in another study, which also studied patients with hemophilia, the majority of whom were young adults. From the researched sample, ten patients (58.8%) reported to have nine or more years of study, and seven (41.2%) reported to be unemployed at the time of the interview. Having finished middle school and being included in the labor market were factors that may have corroborated with the higher percentage of financial independence among the individuals.
In relation to the gravity of the disease, eleven interviewees (64.7%) presented the severe form (Hemophilia A and B). In the Profile of the Hereditary Coagulopathies in Brazil,2 provided by the Brazilian Ministry of Health, the prevalence of severe hemophilia is around 36.09% of the patients with hemophilia A and 29.71% of the patients with hemophilia B.
Even though mostly comprised by individuals with the “severe” classification, 11 patients (64.7%) checked “good” in the general health assessment, asked in Q1 of the instrument WHOQOL-bref. It is believed that such a perspective is due to several factors, among them the treatment and follow-up carried out by the hematologic unit, healthy habits, such as non-smoking (88.2%) and the absence of comorbidities (58.8%). However, the high prevalence of sedentary lifestyles (11.8% of patients with exercise habits), commonly known to be harmful to the health, along with the absence of physiotherapeutic follow-up (88.2%), found in this study may have negatively influenced it and contributed to the result of only two individuals (11.8%) having considered their general health as “very good”.
According to our results, 76.5% of the patients started having bleeding prior to 4 years old, and 52.9% of them had their first hemarthrosis between 1 and 4 years old. It is noteworthy that the high prevalence of hemarthrosis in the study population may be due to the late diagnosis of these patients or even to the poor control of the disease in these cases. However, it should be considered for this analysis that data collection to measure the incidence of hemarthrosis did not originate from the medical records, but rather from the patient reports, which raises the question of whether such data could be overestimated, as they contain subjective information.
Such a fact should trigger the search for information to understand the disease, the quicker access to treatment and, possibly and the lower exposure of these individuals to inappropriate treatments and blood transfusions.
Among the infectious diseases transmissible by blood and hemoderivatives, hepatitis C showed the highest percentage of positive serology, with 8 cases (47.1%). This frequency of hepatitis C is considered high, given the estimated prevalence of hepatitis C in Brazil, lower than 1% and about 34.6% in the general hemophilic population.19 This fact may be partially attributable to blood transfusions, performed in 70.6% of the patients in the study.
The average score for GQOL from the WHOQOL-bref questionnaire was 74.3%, while in a study performed by Nunes et al.12 with the same instrument the value observed was 68.75 (standard scale: from 0 to 100, WHOQOL-bref). Both studies were similar regarding their cohorts, as the sample was likely to present the same complications of the disease and received the same type of standardized treatment by the Hemominas Foundation, which may justify the proximity of values yielded by the GQOL. Results were also similar to ours in a separate analysis of the four domains, and the highest variation found was in the Social Relations domain, with 70.6 in that study and 76.5 points in our study.
From the analysis of the average score of the four domains comprising the questionnaire WHOQOL-bref in this study, the score for Social Relations stands out with the highest score, indicating that personal relations, as well as social support, are factors of higher positive impact upon the Qol of the patients with hemophilia, as observed in a study by Vrabic et al.22 However, the lowest average score occurred in the physical domain, leading to the conclusion that the facets that make up such a domain, for example, pain and discomfort, medication dependence, mobility and energy, have a strong negative interference on the Qol. It is important to highlight that no patients in this study used the lyophilized factor prophylactically. This therapeutic approach would be associated to an enhanced Qol, as evidenced by an American study23 on athletes with hemophilia, observing the benefit of prophylaxis associated with sports, work activities and leisure.
The instrument Haem-A-Qol used in this study reached a high index of reliability. The internal consistency of the questionnaire items was measured by calculating Cronbach’s alpha, rendering a value of 0.859 for the Qol. This value was higher than that observed in the Ferreira study.14
The average score yielded by the specific questionnaire was 36.15, a result that corroborates the average obtained in a study in Juiz de Fora,14 Minas Gerais, Brazil, of 35.33 points. It is worthwhile to highlight similarities between the studies, such as cohort features (age, marital status, education level and household income) and the service offered by the Hemominas Foundation, which may have contributed to this result.
In agreement with studies by Ferreira et al.14 and Mercan et al.,24 the domain with the highest score was Sports and Leisure, probably due to the high prevalence of arthropathies (94.1%), the high impact of the disease on the physical activities and the fear and belief of incompatibility between the disease and sports.
The domain with the lowest average score was Family Planning. This may be understood as the most affected group being patients who were 26–35 years old, and the idea of building a family not being completely solid. It may also be inferred that the follow-up at the hematologic unit itself allowed for more enlightenment regarding the disease, its implications, restrictions and treatment, showing patients that it was possible to constitute a family. The domain Treatment presented an average score of 32.48, similar to the value found by Ferreira,14 which was 35.47, and distant from that obtained by a Turkish study,24 which was 54,8. Ferreira et al.14 correlates his better result to the specialized service of the hematologic unit and higher access to the concentration of factors in his study. Our results corroborate this hypothesis, although the treatment was mostly provided on demand and, in our case, not prophylactically, showing what previous experience at the Hemocenter has done before, that access to the coagulation factor and understanding of the disease itself may have contributed to these results, which emphasizes the importance of the treatment in the Qol.
Through the analysis of agreement between the instruments, using Bland–Altman’s plot chart, no agreement between the questionnaires25 was observed, which allows for the conclusion that these instruments may not possess equivalent results, concerning the Qol. It is expected from the Haem-A-Qol an average score of Qol worse than that measured by the WHOQOL-bref, once the former allows for the evaluation of the facets and specific domains of the disease, such as the presence of arthropathies and bleedings, observed in the majority of our patients. However, another author concluded in a systematic review26 of the health‐related quality of life questionnaires for individuals with hemophilia, that there are still not enough data supporting the application of specific instruments in detriment to generics, pointing to a lack of validation and consistency of those instruments classified as "specific" as the main reasons for such similarities.
Despite the expectation of a worse score of Qol in patients with severe hemophilia and in those with positive serology for infectious diseases, no statistically significant difference was evidenced between the groups, possibly due to a small sample size.
ConclusionHemophilia had a higher negative impact upon physical aspects, sports and leisure in the patients of the sample. The study cohort was mainly comprised of young, single adults, aged between 26 and 35 years old. The analysis of the questionnaires did not reveal statistical agreement between them. Based on this, the Haem-A-Qol is considered the most indicated to evaluate the quality of life of patients with hemophilia, once the questionnaire approaches factors more specifically related to the disease. No statistical significance between the scores of Qol were observed, when linked to the presence or absence of comorbidities, gravity of the hemophilia and positive serology for contagious diseases. Lastly, results of Qol of both questionnaires show values similar to those found in other studies in the literature using the same instruments of data.
Conflicts of interestThe authors declare no conflicts of interest.


