
In this study, we evaluated the influence of the transcript type on hematological and clinical parameters, as well as the event-free survival of 50 patients in the Chronic myeloid leukemia chronic phase.
MethodsWe reviewed the medical records of 55 patients with Chronic myeloid leukemia. The eligibility criteria were based on the availability of hematological and clinical baseline data in the medical records. Data on BCR-ABL transcripts were obtained from medical records.
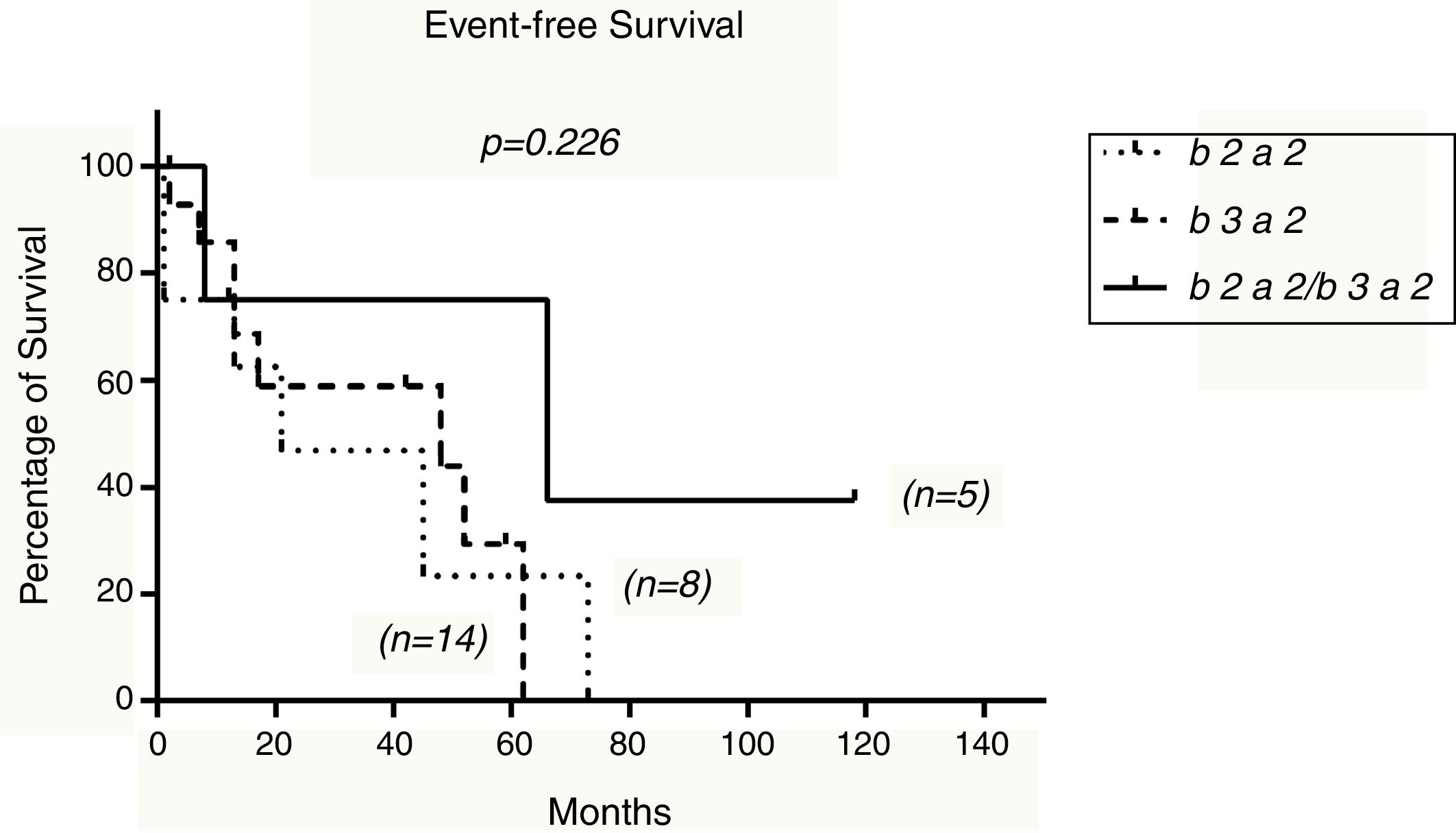
ResultsEighteen patients (36%) had the b2a2 transcript, 24 (48%) had b3a2 and 8 (16%) had b2a2/b3a2. The median platelet count for transcripts b2a2, b3a2 and b2a2/b3a2 was 320.65×103/L, 396×103/L, and 327.05×103/L, respectively (p=0.896). We could not find any differences in relation to the other hematological parameters, when compared to the transcript type. Comparison between spleen and liver size and type of transcript did not differ inside the groups (p=0.395 and p=0.647, respectively) and the association between risk scores and transcript type did not show statistical significance (p>0.05). The 21-month probability for event-free survival was 21%, 48% and 66% for the transcripts b2a2, b3a2 and b2a2/b3a2 respectively (p=0.226)
ConclusionWe conclude that the expression BCR-ABL transcripts have no influence on hematological, clinical and event-free survival parameters of patients in the Chronic myeloid leukemia chronic phase.
Chronic myelogenous leukemia (CML) is characterized by the presence of a reciprocal and balanced translocation, the t(9;22) (q34;q11), which originates the Ph chromosome. The BCR-ABL chimeric gene formation, that encodes a BCR-ABL protein with constitutive tyrosine kinase activity, is the main result of this translocation.1 This hybrid gene commonly results from the BCR gene cleavage in the major breakpoint cluster region (M-BCR) with the fusion of the ABL gene at the exon 2 (a2) level. The BCR gene breakdown in the M-BCR may occur after exon 13 (e13 or b2) or after exon 14 (e14 or b3), thereby generating the BCR-ABL gene, which can form b2a2 or b3a2 mRNA molecules after transcription. Around 5–10% of the patients may also present alternative splicing events that allow simultaneous expression of the transcripts b2a2 and b3a2.2–5
The prognostic significance of these transcripts has been investigated over time; however, their real contribution has not been established. Many studies suggest that hematological and clinical parameters can be influenced by the transcriptional variant type that is expressed.6–8 Studies in this field have shown controversial results in terms of platelet counts: although most studies have failed to demonstrate any significant correlation, others have demonstrated higher platelet counts in patients with the b3a2 transcript.6,9–11
A considerably smaller number of studies attempted to demonstrate transcript influence on the event-free survival outcome of patients expressing different transcripts. Although no significant results were found, a previous study found that patients with the b2a2 transcript showed a lower event-free survival (EFS) trend.10,12
In this study, we evaluated the relevance of hematological and clinical parameters, as well as possible survival outcomes in CML-chronic phase patients expressing different types of BCR-ABL transcripts.
Materials and methodsPatientsThe medical records of 55 patients with CML treated at Walter Cantídeo University Hospital (HUWC) between November 2000 and November 2015 were included in this study, performed under approval by the Federal University of Ceará Research Ethics Committee. The eligibility criteria were based on the availability of hematological and clinical baseline data in the medical records. Patients expressing the transcripts e13a2 (b2a2), e14a2 (b3a2) or co-expressing both e13a2 (b2a2) and e14a2 (b3a2) transcripts were included in the analysis. Patients younger than 18 years, pregnant women, and those in the accelerated and blast phases at diagnosis were excluded. Overall, the patients were submitted to an initial cytoreductive therapy with oral hydroxyurea (HU). After therapy with HU, patients were treated with first-generation tyrosine kinase inhibitors (ITKs) and when necessary, second-generation ITKs were used. Data on BCR-ABL transcripts were obtained from medical records, not necessarily at the diagnosis.
Statistical analysisThe Kruskal–Wallis test or one-way ANOVA was used for the analysis of quantitative variables of the three groups, while the χ2 test was performed for categorical variables. The probability of EFS was estimated by the Kaplan–Maier method and compared by the log-rank test. The EFS was measured from the diagnosis date until the date when the event was observed. Events considered for EFS analysis were loss of hematological, cytogenetic, and molecular response, presence of neutropenia or thrombocytopenia, clonal evolution, disease progression to accelerated or blast phases and treatment failure. Values of p<0.05 were considered significant.
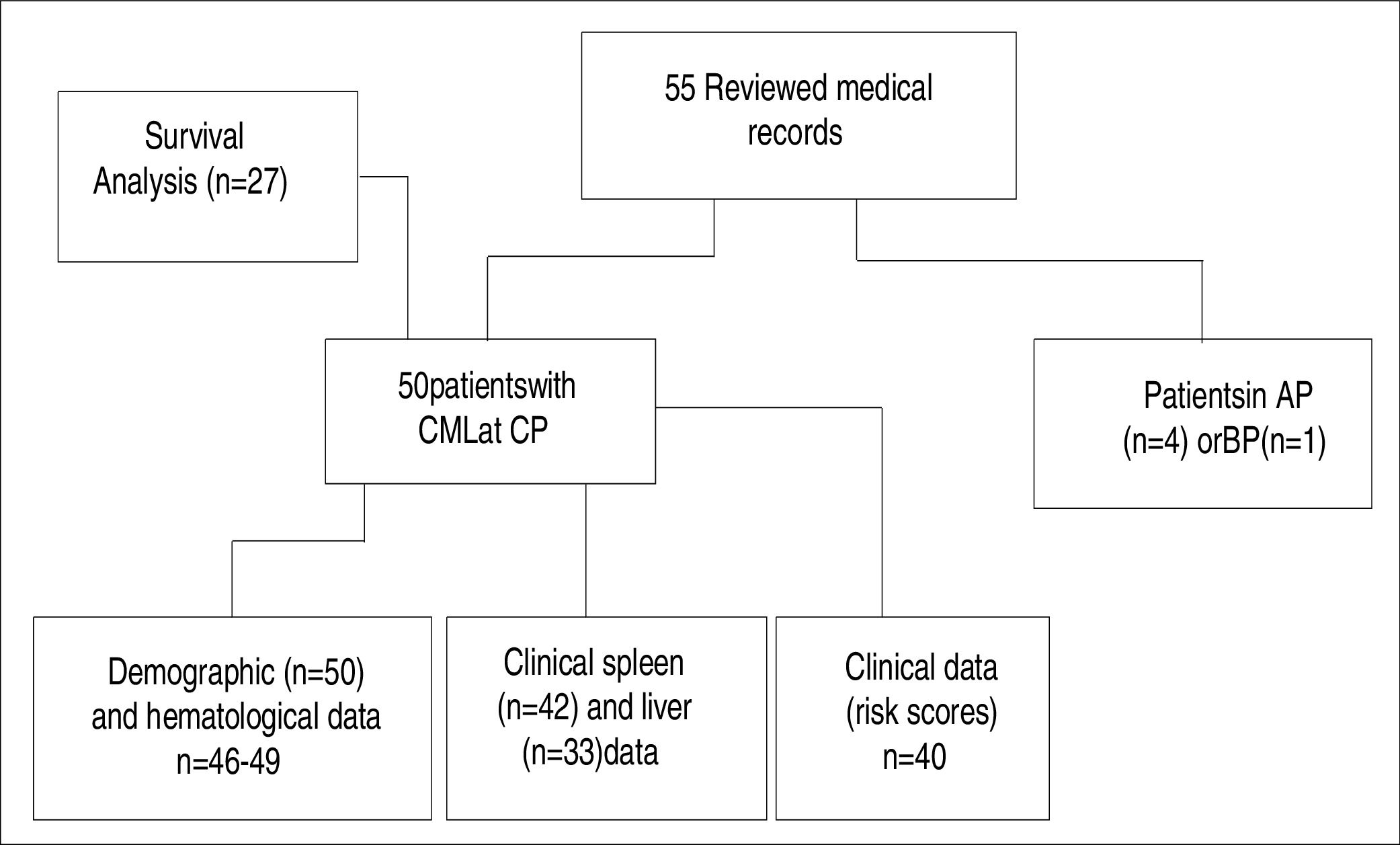
ResultsPatient distribution for the demographic, hematological, clinical, and survival analysis was performed according to data availability and eligibility criteria (Figure 1). Fifty-five records of CML patients with clinical, hematological, and molecular diagnosis were reviewed. Of the 55 patients, 50 (90.9%) were diagnosed in the chronic phase of the disease and included in the analysis. Four patients (7.2%) were diagnosed in the accelerated phase and 1 (1.9%) in the blast phase and thus were excluded from the analysis. Of the 50 patients, 22 (43%) were females and 28 (56%) were males. The mean age at diagnosis was 42.8±14.2 years (ranging from 18 to 71). Eighteen patients (36%) had the b2a2 transcript, 24 (48%) had b3a2 and 8 (16%) had b2a2/b3a2.
; chronic phase (CP); accelerated phase (AP); blast phase (BP).")
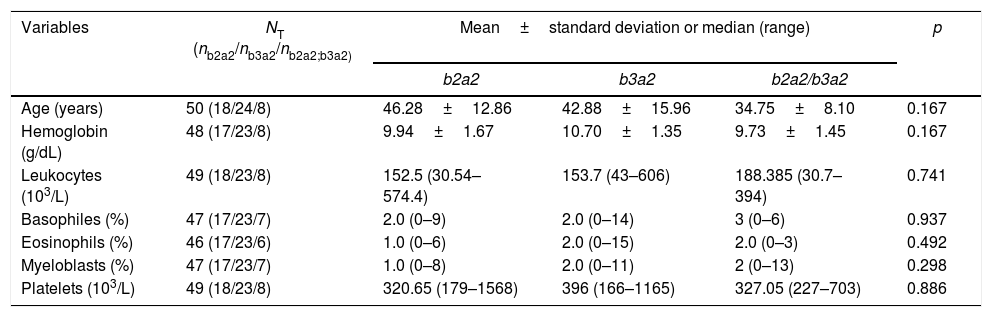
The comparative analysis between the demographic and hematological data with the different BCR-ABL transcripts is shown in Table 1. Patients with the b2a2/b3a2 transcript showed the lowest mean age; however, there was no statistical difference when they were compared with the patients who were carriers of transcripts b2a2 and b3a2 (p=0.167). Statistical analysis showed that platelet counts did not change with the type of transcript, and the median of 320.65×103/L, 396×103/L, 327.05×103/L corresponded respectively to transcripts b2a2, b3a2 and b2a2/b3a2 (p=0.896). As with platelets, the other hematological data did not show any statistical difference (p>0.05), when compared with the type of transcript (Table 1).
Demographic and hematological characteristics of the patients according to the type of transcript.
| Variables | NT (nb2a2/nb3a2/nb2a2;b3a2) | Mean±standard deviation or median (range) | p | ||
|---|---|---|---|---|---|
| b2a2 | b3a2 | b2a2/b3a2 | |||
| Age (years) | 50 (18/24/8) | 46.28±12.86 | 42.88±15.96 | 34.75±8.10 | 0.167 |
| Hemoglobin (g/dL) | 48 (17/23/8) | 9.94±1.67 | 10.70±1.35 | 9.73±1.45 | 0.167 |
| Leukocytes (103/L) | 49 (18/23/8) | 152.5 (30.54–574.4) | 153.7 (43–606) | 188.385 (30.7–394) | 0.741 |
| Basophiles (%) | 47 (17/23/7) | 2.0 (0–9) | 2.0 (0–14) | 3 (0–6) | 0.937 |
| Eosinophils (%) | 46 (17/23/6) | 1.0 (0–6) | 2.0 (0–15) | 2.0 (0–3) | 0.492 |
| Myeloblasts (%) | 47 (17/23/7) | 1.0 (0–8) | 2.0 (0–11) | 2 (0–13) | 0.298 |
| Platelets (103/L) | 49 (18/23/8) | 320.65 (179–1568) | 396 (166–1165) | 327.05 (227–703) | 0.886 |
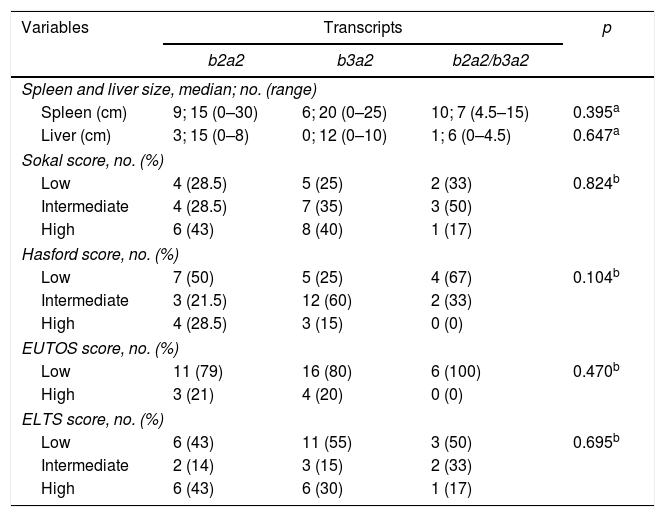
Comparison of transcript types with clinical characteristics (hepatosplenomegaly and risk scores) are summarized in Table 2. The Kruskal–Wallis test revealed that spleen and liver size did not differ between the different types of transcripts (p=0.395 and p==0.647, respectively). The association between risk scores and type of transcript did not show any statistical significance (p>0.05).
Clinical characteristics of the patients according to the type of transcript. Absolute number (no.).
| Variables | Transcripts | p | ||
|---|---|---|---|---|
| b2a2 | b3a2 | b2a2/b3a2 | ||
| Spleen and liver size, median; no. (range) | ||||
| Spleen (cm) | 9; 15 (0–30) | 6; 20 (0–25) | 10; 7 (4.5–15) | 0.395a |
| Liver (cm) | 3; 15 (0–8) | 0; 12 (0–10) | 1; 6 (0–4.5) | 0.647a |
| Sokal score, no. (%) | ||||
| Low | 4 (28.5) | 5 (25) | 2 (33) | 0.824b |
| Intermediate | 4 (28.5) | 7 (35) | 3 (50) | |
| High | 6 (43) | 8 (40) | 1 (17) | |
| Hasford score, no. (%) | ||||
| Low | 7 (50) | 5 (25) | 4 (67) | 0.104b |
| Intermediate | 3 (21.5) | 12 (60) | 2 (33) | |
| High | 4 (28.5) | 3 (15) | 0 (0) | |
| EUTOS score, no. (%) | ||||
| Low | 11 (79) | 16 (80) | 6 (100) | 0.470b |
| High | 3 (21) | 4 (20) | 0 (0) | |
| ELTS score, no. (%) | ||||
| Low | 6 (43) | 11 (55) | 3 (50) | 0.695b |
| Intermediate | 2 (14) | 3 (15) | 2 (33) | |
| High | 6 (43) | 6 (30) | 1 (17) | |
Spleen size: centimeters below left costal margin; liver size: centimeters below the right coast margin.
The EFS analysis for the transcriptional variants of BCR-ABL is shown in Figure 2. The 21-month probability for EFS was 21%, 48% and 66% for the transcripts b2a2, b3a2 and b2a2/b3a2, respectively (p=0.226).
Discussion
In the present study, the b3a2 was the most frequently found transcript in patients in the chronic phase of CML. In addition, the type of BCR-ABL transcript had no influence on the hematological and clinical parameters, nor on the survival outcome of these patients.
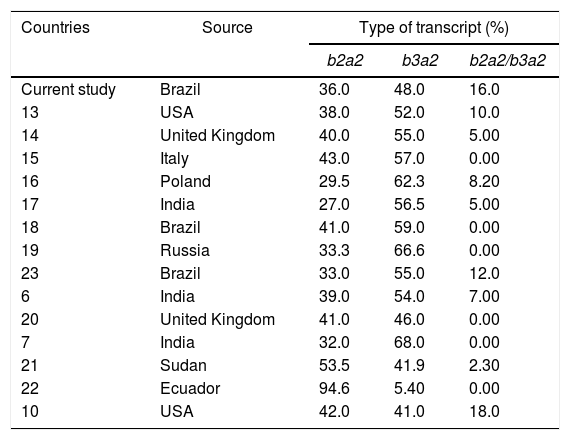
The frequency of BCR-ABL gene transcripts in different countries is shown in Table 3. As in most previous studies, our data showed a higher frequency of the b3a2 transcript, but other studies have also reported, less frequently, a higher incidence of the b2a2 transcript. The different frequencies found could be explained by an inadequate selection of samples or due to genetic components associated with the ethnicity of the target population.
Frequency of transcripts.
| Countries | Source | Type of transcript (%) | ||
|---|---|---|---|---|
| b2a2 | b3a2 | b2a2/b3a2 | ||
| Current study | Brazil | 36.0 | 48.0 | 16.0 |
| 13 | USA | 38.0 | 52.0 | 10.0 |
| 14 | United Kingdom | 40.0 | 55.0 | 5.00 |
| 15 | Italy | 43.0 | 57.0 | 0.00 |
| 16 | Poland | 29.5 | 62.3 | 8.20 |
| 17 | India | 27.0 | 56.5 | 5.00 |
| 18 | Brazil | 41.0 | 59.0 | 0.00 |
| 19 | Russia | 33.3 | 66.6 | 0.00 |
| 23 | Brazil | 33.0 | 55.0 | 12.0 |
| 6 | India | 39.0 | 54.0 | 7.00 |
| 20 | United Kingdom | 41.0 | 46.0 | 0.00 |
| 7 | India | 32.0 | 68.0 | 0.00 |
| 21 | Sudan | 53.5 | 41.9 | 2.30 |
| 22 | Ecuador | 94.6 | 5.40 | 0.00 |
| 10 | USA | 42.0 | 41.0 | 18.0 |
Many studies have evaluated the levels of hemoglobin, leukocytes, basophils, myeloblasts, platelets, spleen size and Sokal score in patients with different transcripts.8,9,11,13,14,15 In the present study, eosinophil counts, liver size, Hasford score, EUTOS score, ELTS score and event-free survival were evaluated.
The analysis of our data was confirmed by previous studies, in which there was no difference in the levels of hemoglobin, leukocytes, basophils and myeloblasts, nor in spleen size, and Sokal score among the types of transcripts.6,8-11,13-15 As for platelet counts, some studies have shown higher values of this parameter in patients expressing the b3a2 transcript.7,10,11 However, our data suggest that platelet counts are independent from the type of transcript expressed, with this finding having been confirmed by other studies.6,8,9,13-14 These discrepancies could be explained by sample selection bias or insufficient sampling.
A study comparing liver size and eosinophil counts with the type of transcript found no difference between the groups, which reinforces our findings that these parameters are not influenced by the transcriptional variants of BCR-ABL.7
In the literature, there is a relatively small number of studies associating risk scores with the type of transcript. These previous studies did not find an association between the Sokal risk, Hasford, EUTOS and ELTS scores and the BCR-ABL transcript type.6,8,10,14,16 In the present study, there was no association between these risk scores and the type of transcript; however, further studies are necessary to verify whether there is an association between these parameters and the type of transcript expressed by the patient.
Besides not influencing the hematological and clinical parameters, the type of transcript does not influence the outcome of EFS. Previous studies have shown no difference in EFS according to the type of transcript, reinforcing the results of our analysis.10,17
A recent study reported that the presence of 25 extra amino acids encoded by the BCR exon 14, which is absent in the e13a2 (b2a2) transcript, promotes structural changes in the SRC (SH1, SH2 and SH3) homology domains and in the DNA binding domain.18 It is believed that these structural changes present in the different transcripts may affect protein tyrosine kinase activity, as it has been demonstrated that this activity is greater in patients with the b2a2 transcript.12 However, we believe that the type of transcript alone is not sufficient to explain differences between the clinical, hematological and EFS parameters. We hypothesize that other factors might alter these parameters, such as the time variable between disease onset and diagnosis, implying in different evolutions and masking the influence of the type of transcript. Moreover, variations in the immune response inherent to each person could affect the evolution of the disease, distorting the contribution of the different BCR-ABL transcripts.
ConclusionsIn summary, we showed that the expression of BCR-ABL transcripts did not influence the hematological, clinical, and EFS parameters in patients with chronic-phase CML. However, further studies are needed to circumvent possible interfering factors and to determine the actual contribution of BCR-ABL transcripts to patient prognosis. If the role of these molecules is confirmed, they can be used to monitor patients with CML in the future.
Conflicts of interestThe authors declare no conflicts of interest.
We thank the Walter Cantidio University Hospital for its support.


