
Sickle cell anemia (SCA) is a common genetic blood disorder, affecting millions worldwide. According to current evidence, individuals with SCA have more than 300 times greater risk to develop bacterial meningitis (BM) than the general population. Herein we have described the characteristics of a series of BM cases in SCA patients in Salvador, Brazil, during 13 years of hospital-based surveillance. Data on clinical presentation, laboratory parameters and outcomes were collected retrospectively by reviewing medical records. From 1999 to 2011, ten SCA patients were identified among the 2511 cases of BM (10/2511; 0.40%). These patients were more likely to be male (90%) and to be younger (median age 8.5 years). The causative agents were Streptococcus pneumoniae (n=5) and Haemophilus influenzae (n=1). The most frequent pneumococcal serotypes were 23F (2 cases), 14, 18F, 23B (one case each). Common medical complications were stroke (n=3); heart failure (n=2), respiratory problems (n=2), renal dysfunctions (n=2) and leg ulcers (n=1). This study highlights the importance of S. pneumoniae as a causative agent of meningitis in individuals with SCA and shows the diversity of comorbidities associated with this condition.
Sickle cell anemia (SCA) is the most frequent hemoglobinopathy worldwide, affecting approximately 20–25 million people.1 Estimates suggest that 250,000 children with SCA are born annually throughout the world. SCA is particularly common among those whose ancestors came from sub-Saharan Africa and Spanish-speaking regions in the Western Hemisphere (South America, the Caribbean, and Central America). In Brazil, SCA is one of the most prevalent hereditary diseases, with approximately 3500 new cases annually.2,3
SCA causes a debilitating systemic syndrome characterized by chronic anemia, acute chest syndrome, stroke, splenic and renal dysfunction, acute painful episodes, and susceptibility to bacterial infections.4,5,6,7 Bacterial diseases usually complicate the course of SCA, meningitis being one of the most life-threatening.
Bacterial meningitis (BM) is a serious public health problem. This infection is severe and poses an increased risk of mortality and sequelae. In Brazil, 6352 BM cases were recorded in 2013, and the three primary causative pathogens were Neisseria meningitides, Streptococcus pneumoniae and Haemophilus influenzae. These agents were responsible for 63% of deaths among 1175 cases of BM.8
The routine vaccination against H. influenzae (Hib) and the introduction of the 10-valent pneumococcal conjugate vaccine (PCV10), associated with the prophylactic oral penicillin, have contributed to the decrease of bacteremia and BM in patients with SCA.9 However, these patients remain at an increased risk of developing BM.
Epidemiological data regarding the patterns of infection, lethality and clinical course of illness are scarce in the scientific literature for this risk group. Therefore, the purpose of the present investigation is to describe a series of BM cases in patients with SCA at a referral infectious diseases hospital over 13 years of active surveillance.
MethodsStudy setting and diagnosis of bacterial meningitisAn active surveillance system for BM was established at Hospital Couto Maia (HCM), a referral institution for infectious diseases. This medical facility provides public healthcare for residents from the Metropolitan Region of Salvador, Brazil (2,921,087 inhabitants in 2015).10
According to recommendations from the Secretary of State for Health, all suspected cases of meningitis in the region are submitted to diagnostic procedures, including lumbar puncture and cerebrospinal fluid examination, as well as isolation precaution protocols.
A case of BM was defined as follows: 1) clinical presentation of meningitis, characterized by fever, meningismus, and altered mental status; 2) an abnormal cerebrospinal fluid examination, and/or; 3) positive cerebrospinal fluid or blood culture for any bacteria.
For cases in which Gram stain and culture techniques were negative, the criteria to define BM was the following: glucose concentration less than 40mg/L, and/or protein concentration more than 50mg/dL, and/or a white cell count over 100 cells per mm3, and neutrophil percentage over 50%.
Case definition, study design and data collectionA case was defined as a patient with confirmed SCA, who had BM and was hospitalized at HCM from 1999 to 2011. We set up a retrospective cohort study. The research team reviewed medical records using a standardized questionnaire to collect demographic information, clinical presentation, and outcome characteristics.
Laboratory methodsFollowing laboratory guidelines, routine tests for CSF analysis were performed, including leukocyte count, glucose, protein and Gram stain and culture. The latex agglutination test for bacterial antigen detection was conducted according to kit availability and/or medical request. Pneumococcal isolates were serotyped by the Centers for Disease Control and Prevention (CDC), using the capsular swelling method with type-specific antiserum.
Hematological analyses were carried out using an electronic cell counter (Sismex XE-2100D). Sickle cell was identified through sickling and solubility tests.
Statistical analysisA database was built using the Epi-Info version 3.5.1 (CDC, Atlanta, GA, USA), and later used to screen patients with meningitis who had reported SCA. The statistical analyses were performed with R software (version 3.2.3 - http://www.r-project.org). The categorical and continuous variables are presented as number and proportion, median and range, respectively.
EthicsPatients were enrolled in the study according to informed consent procedures approved by the Institutional Review Boards of the Oswaldo Cruz Foundation, Brazilian Ministry of Health and the Hospital Couto Maia.
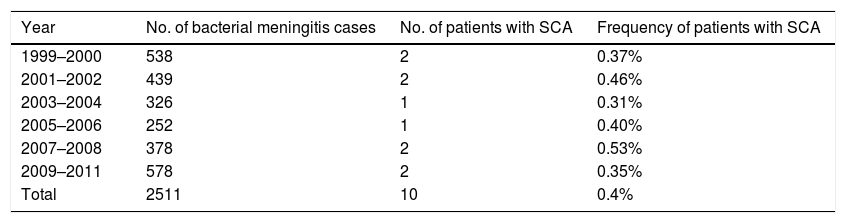
ResultsThe frequency of patients with SCA among BM casesFrom 1999 to 2011, the surveillance system consecutively identified 2511 cases of BM, ten of which were patients diagnosed with SCA. The frequency of patients with SCA among BM cases during these 13 years was 0.40% (Table 1).
Frequency of patients with diagnosis of SCA among bacterial meningitis cases identified in Salvador in the period of.1999–2011.
| Year | No. of bacterial meningitis cases | No. of patients with SCA | Frequency of patients with SCA |
|---|---|---|---|
| 1999–2000 | 538 | 2 | 0.37% |
| 2001–2002 | 439 | 2 | 0.46% |
| 2003–2004 | 326 | 1 | 0.31% |
| 2005–2006 | 252 | 1 | 0.40% |
| 2007–2008 | 378 | 2 | 0.53% |
| 2009–2011 | 578 | 2 | 0.35% |
| Total | 2511 | 10 | 0.4% |
Overall, most of the patients were likely to be male (9/10) and to be younger (median age 8.5 years). On average, the duration of symptoms was two days and the length of the hospital stay was 13.5 days. Two patients (20%) were admitted to an intensive care unit (ICU), and five (50%) received a blood transfusion.
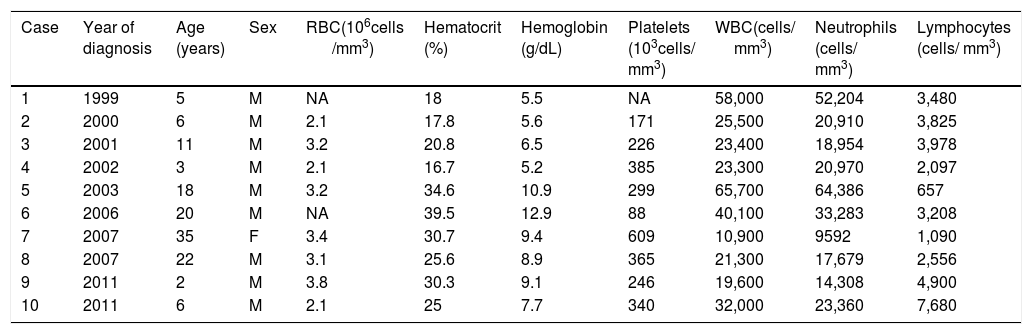
Regarding hematological analysis at admission, the red blood cell (RBC) count ranged from 2.1 to 3.8×106cells/mm3, with reticulocytes accounting for 16.7% to 39.5%. The hemoglobin level ranged from 5.5 to 12.9g/dl and the platelet count, from 88 to 609×103 cells/mm3. In addition, the white blood cell (WBC) count ranged from 10,900 to 65,700 cells/mm3 with 9592 to 64,386 neutrophils/mm3 (Table 2).
Demographic and hematological characteristics of each patient with a diagnosis of SCA and bacterial meningitis.
| Case | Year of diagnosis | Age (years) | Sex | RBC(106cells /mm3) | Hematocrit (%) | Hemoglobin (g/dL) | Platelets (103cells/ mm3) | WBC(cells/ mm3) | Neutrophils (cells/ mm3) | Lymphocytes (cells/ mm3) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1999 | 5 | M | NA | 18 | 5.5 | NA | 58,000 | 52,204 | 3,480 |
| 2 | 2000 | 6 | M | 2.1 | 17.8 | 5.6 | 171 | 25,500 | 20,910 | 3,825 |
| 3 | 2001 | 11 | M | 3.2 | 20.8 | 6.5 | 226 | 23,400 | 18,954 | 3,978 |
| 4 | 2002 | 3 | M | 2.1 | 16.7 | 5.2 | 385 | 23,300 | 20,970 | 2,097 |
| 5 | 2003 | 18 | M | 3.2 | 34.6 | 10.9 | 299 | 65,700 | 64,386 | 657 |
| 6 | 2006 | 20 | M | NA | 39.5 | 12.9 | 88 | 40,100 | 33,283 | 3,208 |
| 7 | 2007 | 35 | F | 3.4 | 30.7 | 9.4 | 609 | 10,900 | 9592 | 1,090 |
| 8 | 2007 | 22 | M | 3.1 | 25.6 | 8.9 | 365 | 21,300 | 17,679 | 2,556 |
| 9 | 2011 | 2 | M | 3.8 | 30.3 | 9.1 | 246 | 19,600 | 14,308 | 4,900 |
| 10 | 2011 | 6 | M | 2.1 | 25 | 7.7 | 340 | 32,000 | 23,360 | 7,680 |
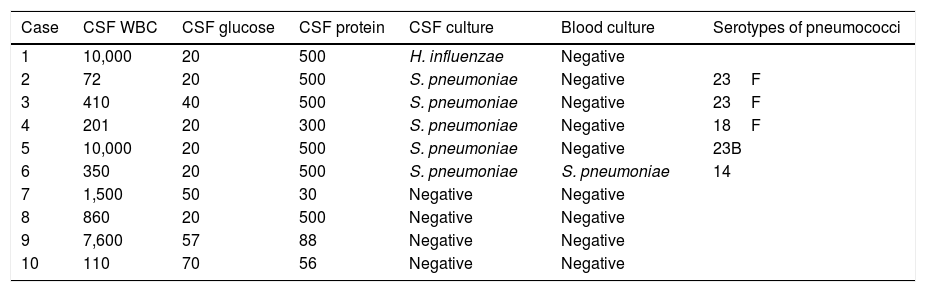
Concerning CSF parameters, the WBC count ranged from 72 to 10,000cells/mm3, the glucose level, from 20 to 70mg/dl and protein, from 30 to 500mg/dl. CSF cultures and Gram stain were positive in six cases (60%), and one had a positive blood culture. The bacteria H. influenzae was the causative agent in one case (10%), and S. pneumoniae in five cases (50%). The pneumococcal serotypes identified were 23F (two cases) and 14, 18F, 23B (one case each) (Table 3). Four patients did not have the etiologic agent of meningitis defined, three of whom had previously used antibiotics, such as cephalothin, ceftriaxone, and clindamycin.
Laboratory characteristics of CSF of each patient with diagnosis of SCA and bacterial meningitis.
| Case | CSF WBC | CSF glucose | CSF protein | CSF culture | Blood culture | Serotypes of pneumococci |
|---|---|---|---|---|---|---|
| 1 | 10,000 | 20 | 500 | H. influenzae | Negative | |
| 2 | 72 | 20 | 500 | S. pneumoniae | Negative | 23F |
| 3 | 410 | 40 | 500 | S. pneumoniae | Negative | 23F |
| 4 | 201 | 20 | 300 | S. pneumoniae | Negative | 18F |
| 5 | 10,000 | 20 | 500 | S. pneumoniae | Negative | 23B |
| 6 | 350 | 20 | 500 | S. pneumoniae | S. pneumoniae | 14 |
| 7 | 1,500 | 50 | 30 | Negative | Negative | |
| 8 | 860 | 20 | 500 | Negative | Negative | |
| 9 | 7,600 | 57 | 88 | Negative | Negative | |
| 10 | 110 | 70 | 56 | Negative | Negative |
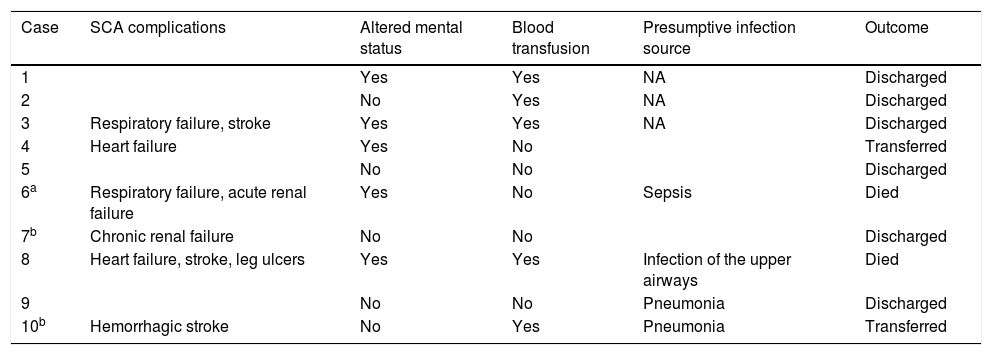
In regard to clinical symptoms, 50% of the patients presented altered mental status at admission, and 40% had pneumonia.
One 3-year-old patient was transferred to another hospital owing to heart failure, and another 6-year-old patient had hypertension and was medicated with dihydralazine. Furthermore, these two patients have also undergone prophylactic penicillin therapy.
Two patients died (20%), and both of them had meningitis caused by S. pneumoniae. One of them was 20 years old and had other underlying diseases, namely hepatitis B, acute renal failure, and respiratory failure. The other one was 22 years old and had heart failure and leg ulcers.
In this cohort, we have identified only one female patient. She had complications, a few of which were chronic renal failure and hypertension, but she survived.
Three patients had a medical history of stroke; two of them were children of 6 and 11 years old, respectively and one was a 22-year-old adult. The youngest child had a hemorrhagic stroke episode (Table 4).
Clinical characteristics and outcome of each patient with diagnosis of SCA and bacterial meningitis.
| Case | SCA complications | Altered mental status | Blood transfusion | Presumptive infection source | Outcome |
|---|---|---|---|---|---|
| 1 | Yes | Yes | NA | Discharged | |
| 2 | No | Yes | NA | Discharged | |
| 3 | Respiratory failure, stroke | Yes | Yes | NA | Discharged |
| 4 | Heart failure | Yes | No | Transferred | |
| 5 | No | No | Discharged | ||
| 6a | Respiratory failure, acute renal failure | Yes | No | Sepsis | Died |
| 7b | Chronic renal failure | No | No | Discharged | |
| 8 | Heart failure, stroke, leg ulcers | Yes | Yes | Infection of the upper airways | Died |
| 9 | No | No | Pneumonia | Discharged | |
| 10b | Hemorrhagic stroke | No | Yes | Pneumonia | Transferred |
NA: not available.
A 20-year-old boy (case 6), who had presented BM symptoms for two days, was admitted to the ICU. At the moment of admission, the patient developed respiratory failure, acute renal failure, and altered mental status. His initial hemogram (CBC) showed thrombocytopenia, leukocytosis, and hemoconcentration. Blood and CSF culture were positive for S. pneumoniae serotype 14. The patient died after four days of hospitalization.
DiscussionBM, as well as other infectious diseases, frequently complicates the course of patients with SCA and contributes to high case fatality ratios. Understanding the factors involved in the development of meningitis in this risk group is of great importance to prevent infections and improve prognosis.
This series of ten SCA cases corresponds to 0.4% of all BM cases recorded from 1999 to 2011 at Hospital Couto Maia. The frequency observed here was remarkably lower than in previous reports. As an illustration, Williams and colleagues have estimated 8.6% SCA cases among BM episodes (20 patients with SCA/232 BM cases) in Kenyan children in a retrospective cohort and case-control study.11
There can be a number of reasons why this low frequency was observed in our setting. Firstly, it may result from the type of study, since in retrospective cohort losses might occur. Another possible reason is the introduction of the Hib vaccine and PCV7 vaccine in Brazil in 1999 and 2003, respectively.
Most of our patients were likely to be male (90%) and to be younger (median age 8.5 years, range 2–35 years). The population described herein was considerably older than those reported in other investigations.11,12
We observed lower values of RBC, hemoglobin concentrations and hematocrit in almost all patients with SCA. This phenomenon might be explained by the rate of chronic hemolysis associated with SCA. Similar results were obtained by Akinbami et al. in Lagos, Nigeria, among patients with SCA in steady state.13
In the present study, the WBC and neutrophil count was generally higher in SCA patients. This finding is consistent with other studies, and it is normally triggered by the process of increased demargination of intravascular neutrophils, accelerated release from the bone marrow and reduction in the rate at which neutrophils leave the blood. Regarding the platelet count, almost all patients had typical values except two, one of whom had thrombocytopenia and the other, thrombocytosis.
Among the ten cases described herein, only one case of H. influenzae meningitis was registered. Interestingly, this episode happened in 1999, during the pre-vaccine period in Brazil for the Hib-vaccine. The introduction of the Hib-vaccine led to a dramatic reduction in the incidence rate of H. influenzae meningitis of 40–95% in the post-vaccine period, compared to the pre-vaccine period.14 Reports from HCM surveillance also have shown a sharp decrease from 2.39 to 0.06 cases per 100,000 inhabitants (98%) of H. influenzae meningitis in this setting.15 We suppose that for this reason, no case of H. influenzae meningitis was recorded in the post-vaccine period.
In the present evaluation, the frequency of pneumococcal meningitis among patients with SCA was 50% (5/10). This rate is lower than the ones previously reported in other settings. For instance, Gill and colleagues estimated the incidence of pneumococcal meningitis at 90.9% (10 /11) in a cohort of infants with SCA.12
This finding might have happened on account of the general reduction in pneumococcal meningitis over the past decade in Salvador.16,17 The small proportion of cases of pneumococcal meningitis could also stem from the previous antibiotic use. In the present evaluation, three patients have undergone empirical antibiotic therapy. In all these cases, the causative agents were not identified using conventional culture techniques. This finding is not surprising since it is widely accepted that the presence of antimicrobial residues may affect the recovery of bacteria in biological samples.
Among the five cases of pneumococcal meningitis, only one was lethal. The patient who died was 22 years old and had meningitis caused by S. pneumoniae serotype 14. This finding is consistent with previous reports, since serotype 14 is considered to be one of the leading causes of death in this setting.18 The fatality rate of pneumococcal meningitis was 20% (1/5). This result is similar to those of Gill et al., who reported two deaths (20%) due to S. pneumoniae in ten children with SCA.12
Current evidence suggests that the survival of young children with SCA has improved and the pattern of mortality has changed over the past decades. A case in point is the investigation conducted by Quinn and colleagues. The authors have examined the Dallas Newborn Cohort in order to provide contemporary survival data for children with SCA. The research demonstrates that all deaths occurred in patients who were 18 years or older.19 In our study, there were two deaths overall, and both patients were over 18 years old. This result might be a consequence of newborn screening, prophylactic penicillin therapy and effective vaccination programs against Hib and S. pneumoniae during early childhood.
Despite the changing pattern of mortality, published sources indicate that individuals with SCA still have a high risk of pneumococcal infections. This might happen due to genetic changes among bacteria, the emergence of non-vaccine serotypes and other mutations affecting antibiotic resistance.
The pneumococcal serotypes identified in the five cases reported here were 23F (n=2), 14 (n=1), 18F (n=1), 23B (n=1). The 23F and 18F are vaccine serotypes, but the serotypes 18F and 23B are not included in the PCV10 or PPV23 vaccines. These results are similar to those of McCavit et al. The authors have identified seven cases of invasive pneumococcal disease caused by non-vaccine serotypes in patients with SCA since the development of the PVC7 in the USA.20
Likewise, Santoro et al. described one case of pneumococcal meningitis caused by the non-vaccine serotype 23B in an African American boy with SCD.21 In addition, pneumococcal meningitis by non-vaccine serotype 18F was detected in a 14-year-old patient with SCA, who later died.22
BM in SCA patients can be due to several variables, a few of which are inadequate vaccination, limited immune response to vaccines and decreased use of penicillin prophylaxis.23 In the present investigation, data regarding immunization status was not available to verify the effectiveness of pneumococcal vaccines.
BM is a significant cause of morbidity in patients with SCA. Nonetheless, few studies focus on describing medical complications associated with this risk group. In the present evaluation, three patients had a medical history of stroke, one of whom was a 6-year-old child who had a hemorrhagic stroke and motor sequelae. This result contradicts those presented by Ohene-Frempong and colleagues, who found that hemorrhagic stroke occurred more frequently in adults.24 Moreover, other complications were identified, namely renal, respiratory and cardiac failure, leg ulcers, hepatitis B and hypertension.
This study has some limitations that should be acknowledged. First, in a retrospective cohort study, loss of information often occurs. To avoid missing or incomplete data, we double-checked the medical records. In addition, data referring to immunization status were not available in the medical records and was therefore not included in this investigation. Unfortunately, it was not possible to contact patients or their legal guardians to obtain this data. Finally, the study describes patients with sickle cell anemia, a risk group for bacterial infections in general. Those patients usually undergo prophylactic antibiotic therapy, which may affect the performance of classical microbiological tests, such as Gram stain and culture techniques. This can limit the etiological identification of BM, as indeed occurred in four of the ten cases reported here. Molecular methods, such as real-time PCR, are not affected by the antibiotic presence and might be advisable in this scenario.
This investigation provides valuable information on risk factors for BM in patients with SCA. In summary, we found that the frequency of patients with SCA among cases of BM was low in Salvador, Bahia. Patients with this condition were more likely to be male, to be younger and to have developed meningitis by S. pneumoniae. This study also cautions for the importance of pneumococcal vaccination in daily practice. The fatality rate for pneumococcal meningitis was worrisome in our setting, reaching 20%. The possibility of improving the outcomes of these patients by prevention is extremely important.
FundingResearch Support Foundation for the State of Bahia (FAPESB-PP-SUS0001/2009), National Council for Scientific and Technological Development (CNPq – 400005/2013-1).
Conflict of interestNone.
We would like to thank the patients and their families. We are also grateful to the team at the Clinical Laboratory and administrative staff at Hospital Couto Maia. We are especially grateful to Marcelo Teles Bastos Ribeiro and Ronaldo José Ribeiro Santos for their immense support in running this surveillance network.


