

Autoimmune diseases are an important field for the development of bone marrow transplantation, or hematopoietic stem cell transplantation. In Europe alone, almost 3000 procedures have been registered so far. The Brazilian Society for Bone Marrow Transplantation (Sociedade Brasileira de Transplantes de Medula Óssea) organized consensus meetings for the Autoimmune Diseases Group, to review the available literature on hematopoietic stem cell transplantation for autoimmune diseases, aiming to gather data that support the procedure for these patients. Three autoimmune diseases for which there are evidence-based indications for hematopoietic stem cell transplantation are multiple sclerosis, systemic sclerosis and Crohn's disease. The professional stem cell transplant societies in America, Europe and Brazil (Sociedade Brasileira de Transplantes de Medula Óssea) currently consider hematopoietic stem cell transplantation as a therapeutic modality for these three autoimmune diseases. This article reviews the evidence available.
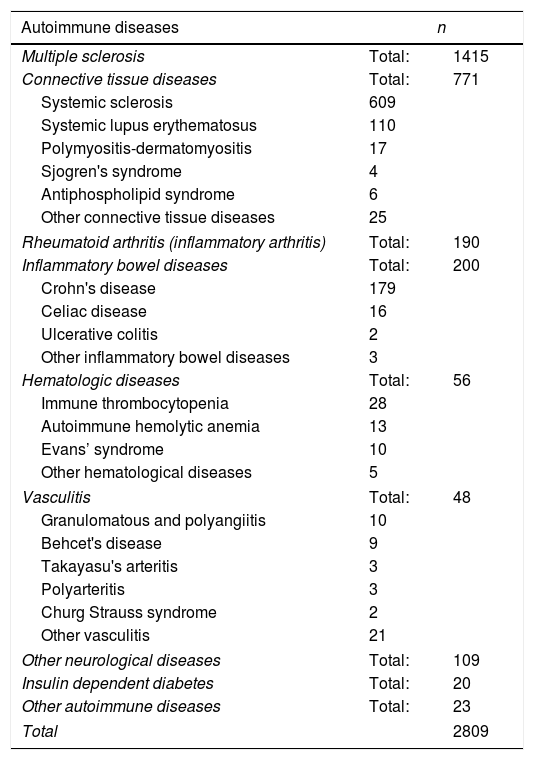
Autoimmune diseases have become an important field for the development of hematopoietic stem cell transplantation (HSCT). The European Society for Blood and Marrow Transplantation (EBMT) recently published an update of transplant indications for autoimmune diseases, with a total of 2809 cases registered at that point. The cases are summarized in Table 1.1
Hematopoietic stem cell transplants for autoimmune diseases according to the European Society for Blood and Marrow Transplantation (EBMT).1
| Autoimmune diseases | n | |
|---|---|---|
| Multiple sclerosis | Total: | 1415 |
| Connective tissue diseases | Total: | 771 |
| Systemic sclerosis | 609 | |
| Systemic lupus erythematosus | 110 | |
| Polymyositis-dermatomyositis | 17 | |
| Sjogren's syndrome | 4 | |
| Antiphospholipid syndrome | 6 | |
| Other connective tissue diseases | 25 | |
| Rheumatoid arthritis (inflammatory arthritis) | Total: | 190 |
| Inflammatory bowel diseases | Total: | 200 |
| Crohn's disease | 179 | |
| Celiac disease | 16 | |
| Ulcerative colitis | 2 | |
| Other inflammatory bowel diseases | 3 | |
| Hematologic diseases | Total: | 56 |
| Immune thrombocytopenia | 28 | |
| Autoimmune hemolytic anemia | 13 | |
| Evans’ syndrome | 10 | |
| Other hematological diseases | 5 | |
| Vasculitis | Total: | 48 |
| Granulomatous and polyangiitis | 10 | |
| Behcet's disease | 9 | |
| Takayasu's arteritis | 3 | |
| Polyarteritis | 3 | |
| Churg Strauss syndrome | 2 | |
| Other vasculitis | 21 | |
| Other neurological diseases | Total: | 109 |
| Insulin dependent diabetes | Total: | 20 |
| Other autoimmune diseases | Total: | 23 |
| Total | 2809 | |
Although autologous HSCT (AHSCT) has been used worldwide to treat autoimmune diseases, with slightly different approaches among centers, the main strategy remains similar. Briefly, the procedure consists of a first phase, when autologous hematopoietic stem cells are harvested and cryopreserved, and a second phase, including conditioning regimen and stem cell infusion. Patients undergo mobilization of hematopoietic stem cells from the bone marrow to peripheral blood through a combination of drugs including filgrastim (a granulocyte colony stimulating factor, G-CSF), followed by cell harvesting by leukapheresis and cryopreservation. Most transplant centers use 2–4g/m2 cyclophosphamide and granulocyte colony-stimulating factor (G-CSF) for subsequent collection of hematopoietic progenitor cells.2–13 The scheme allows for collection of more cells than the use of G-CSF as a single agent, and very few events of mobilization failure are described. Additionally, the administered cyclophosphamide promotes initial control of disease activity, contributing to the therapeutic effect of the transplant procedure.10,11,13
At the second phase of HSCT, patients receive immunoablative doses of a lymphoablative conditioning regimen that may include chemotherapeutic agents, immunotherapeutic agents and/or irradiation, followed by autologous cell infusion. A period of aplasia follows, after which there is engraftment and reconstitution of a tolerant and no longer self-reactive immune system.10,14 The purpose of HSCT in autoimmune diseases is to promote immune depletion, eliminate autoreactive lymphocytes, and to reprogramme the immune system, leading to the reestablishment of immune tolerance and, thereby, prolonged disease control.15
The Brazilian Society for Bone Marrow Transplantation (Sociedade Brasileira de Transplantes de Medula Óssea, SBMTO) organized consensus meetings for the Autoimmune Diseases Group, to review the available literature on HSCT for autoimmune diseases, aiming to gather evidence that support the procedure for these patients. Three of the most important indications for HSCT, sufficiently evidence-based, are multiple sclerosis (MS), systemic sclerosis (SSc) and Crohn's disease. As the following sections show, the American Society for Transplantation and Cellular Therapy (ASTCT), the European Society (EBMT), and the Brazilian SBMTO currently consider HSCT as part of the already consolidated treatment procedures for these three autoimmune diseases, outside research trial settings.
Multiple sclerosisMultiple sclerosis (MS) is a demyelinating chronic inflammatory disease of the central nervous system that mainly affects young adults, and has heterogeneous clinical and pathological characteristics resulting from different pathways of tissue injury.16 Inflammation, demyelination, and axonal degeneration are the main pathological mechanisms that cause clinical manifestations.17 However, the cause of MS is unknown18,19 and it is considered an incurable disease. The most widely accepted theory is that MS begins as an autoimmune inflammatory reaction mediated by autoreactive lymphocytes.16,20 Microglia activation and chronic neurodegeneration occur later. Regardless of the immune pattern of early demyelination, analyzes of active lesions over time suggest that there is a single immuno-effector mechanism in each person.21
MS begins at the median age of 23.5 years, and mean age of 30 years.22 Mortality among patients with MS is not much different from the general population, but neurological deficits progress in all patients. It is expected that in 15 years from diagnosis, 50% of patients will need help walking, and after 25 years, most cannot walk anymore.23,24
MS symptoms are non-specific and may include paresthesias and paresis due to transverse myelitis, ataxia due to cerebellar injury, tremor, monocular visual loss due to optic neuritis, double vision due to brainstem dysfunction, fatigue and sphincter changes. If there is a relapse episode, the functional disability scale score used in neurological examination increases, indicating worsening. During remission, the patient remains stable within his or her disability score. Numerous scales have been described to evaluate MS, the most used being the Expanded Disability Status Scale (EDSS), described by Kurtzke.25
MS is classified in three clinical types, which receive different treatment approaches. The first is the relapsing remitting type (RRMS), resulting from inflammatory multifocal lesions that cause clinical recurrence and activity of detectable lesions on magnetic resonance imaging (increase or appearance of new lesions on hyperintense T2 or increase of gadolinium on T1 lesions). It manifests with episodic relapses followed by partial or total recovery from dysfunction, interspersed with remission periods of at least 30 days.23,24
After an average time of 10–15 years, the episodes become less frequent, followed by less evident recovery, with accumulation of sequelae and gradual worsening of the neurological picture that is typical of the secondary progressive form (SPMS). This is characterized by neurodegeneration, but may still have superimposed inflammatory activity.23,24
The third clinical type of MS, the primary progressive MS (PPMS), occur in about 10–15% of patients, at the mean age onset of approximately 40 years, and occurs equally in males and females. It is characterized by progressive accumulation of disability from disease onset. Can occur occasional plateaus, minor and temporary improvements but after all continues progressing. The diagnosis is made based only on patient's history. This “malignant form” or “aggressive form” of MS, is characterized by rapidly progressive course, leading to significant disability, or even death, in multiple neurologic systems in a relatively short time after disease onset.23,24
The worsening of symptoms is highly heterogeneous among patients with MS. The extent of inflammatory activity affects MS prognosis substantially. Because of that, the goal of treatment approaches is the absence of disease activity clinically or at magnetic resonance imaging and the improvement of disability or of the EDSS score. This is called “no evidence of disease activity” (NEDA).26
Conventional therapeutic approaches for multiple sclerosisAs of December 2017, the US Food and Drug Administration (FDA) has approved 15 drugs considered as capable of modifying MS course: 5 interferon-beta preparations; two glatiramer acetate preparations; the monoclonal antibodies natalizumab, alemtuzumab, daclizumab and ocrelizumab (the first B-cell targeted therapy); the chemotherapeutic agent mitoxantrone; and small molecule oral agents fingolimod, dimethyl fumarate and teriflunomide. Dalfampridine (aminoperidine) has been approved as a therapy to treat and improve gait speed.21 However, none of these are curative therapies. They are partially effective in reducing relapse rates and disease progression. Furthermore, all disease-modifying therapies present safety concerns, with the risk increasing over time. Better treatment strategies are required for patients with relapsing MS, for those who present inflammatory activity despite the treatment used and for those with treatment side effects.27
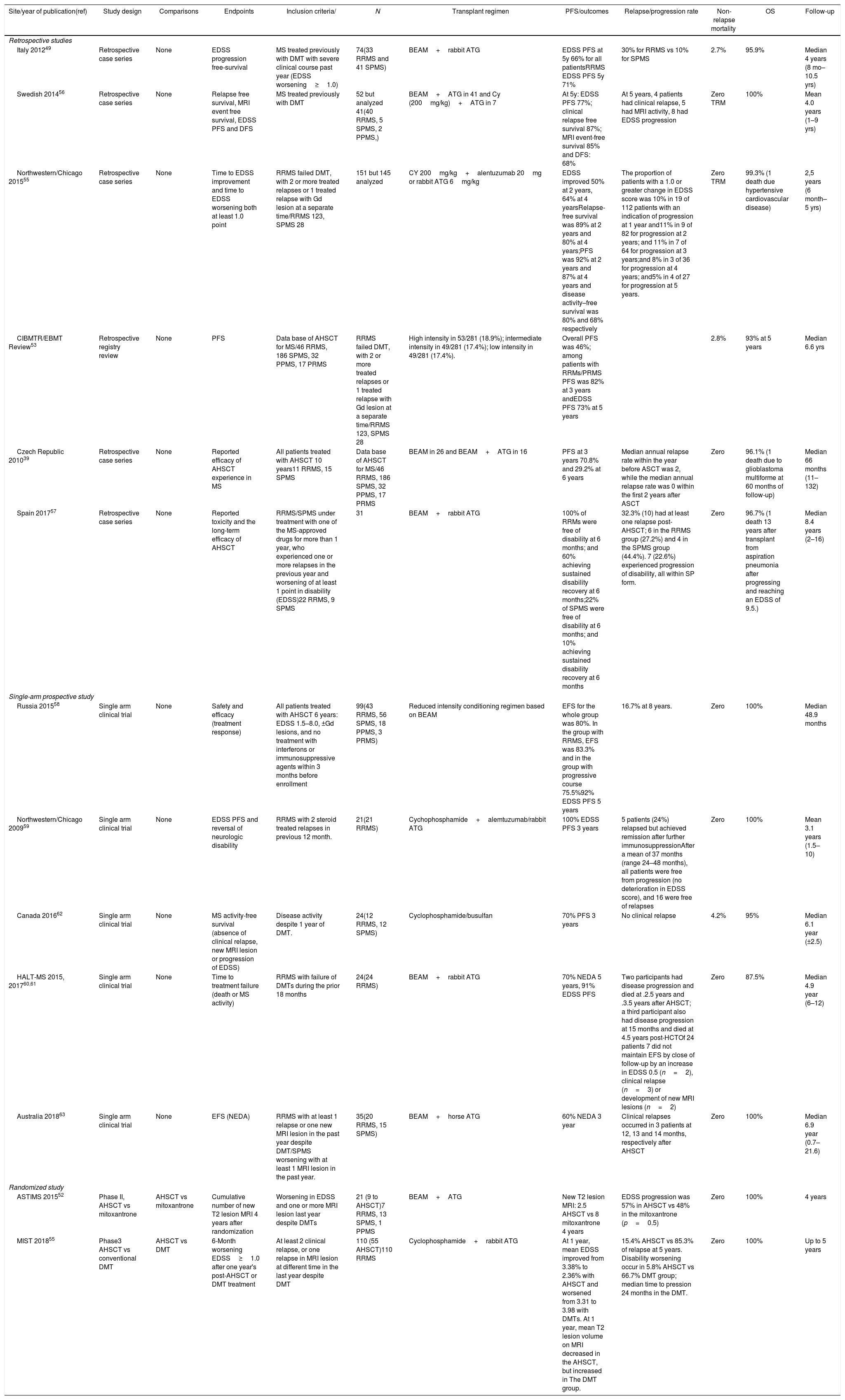
Transplant in multiple sclerosisSince the mid-1990s, with the first studies on animal models with subsequent clinical application, autologous transplantation (AHSCT) has been an important tool in inducing an “immunotolerant” immune reconstitution.2,3 Thousands of transplants for treating MS have been performed worldwide, with more than 700 evaluated in studies.6,28–46 Some studies showed progression-free survival of more than five years,39,43 with superior neurological improvement in patients with relapsing-remission type and in those with inflammatory activity observed on magnetic resonance imaging.43,47,48Table 2 shows the results of the main studies focused on the use of HSCT to treat MS: there are 8 retrospective studies and 6 single-arm clinical trials on AHSCT for MS, and only 2 randomized clinical trials focusing on the comparison of AHSCT versus disease-modifying therapies for MS. There are also 3 meta-analysis and systematic reviews and one position paper.6,9,10,39,49–57
Results of studies on multiple sclerosis disease.
| Site/year of publication(ref) | Study design | Comparisons | Endpoints | Inclusion criteria/ | N | Transplant regimen | PFS/outcomes | Relapse/progression rate | Non-relapse mortality | OS | Follow-up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Retrospective studies | |||||||||||
| Italy 201249 | Retrospective case series | None | EDSS progression free-survival | MS treated previously with DMT with severe clinical course past year (EDSS worsening≥1.0) | 74(33 RRMS and 41 SPMS) | BEAM+rabbit ATG | EDSS PFS at 5y 66% for all patientsRRMS EDSS PFS 5y 71% | 30% for RRMS vs 10% for SPMS | 2.7% | 95.9% | Median 4 years (8 mo–10.5 yrs) |
| Swedish 201456 | Retrospective case series | None | Relapse free survival, MRI event free survival, EDSS PFS and DFS | MS treated previously with DMT | 52 but analyzed 41(40 RRMS, 5 SPMS, 2 PPMS,) | BEAM+ATG in 41 and Cy (200mg/kg)+ATG in 7 | At 5y: EDSS PFS 77%; clinical relapse free survival 87%; MRI event-free survival 85% and DFS: 68% | At 5 years, 4 patients had clinical relapse, 5 had MRI activity, 8 had EDSS progression | Zero TRM | 100% | Mean 4.0 years (1–9 yrs) |
| Northwestern/Chicago 201555 | Retrospective case series | None | Time to EDSS improvement and time to EDSS worsening both at least 1.0 point | RRMS failed DMT, with 2 or more treated relapses or 1 treated relapse with Gd lesion at a separate time/RRMS 123, SPMS 28 | 151 but 145 analyzed | CY 200mg/kg+alentuzumab 20mg or rabbit ATG 6mg/kg | EDSS improved 50% at 2 years, 64% at 4 yearsRelapse-free survival was 89% at 2 years and 80% at 4 years;PFS was 92% at 2 years and 87% at 4 years and disease activity–free survival was 80% and 68% respectively | The proportion of patients with a 1.0 or greater change in EDSS score was 10% in 19 of 112 patients with an indication of progression at 1 year and11% in 9 of 82 for progression at 2 years; and 11% in 7 of 64 for progression at 3 years;and 8% in 3 of 36 for progression at 4 years; and5% in 4 of 27 for progression at 5 years. | Zero TRM | 99.3% (1 death due hypertensive cardiovascular disease) | 2,5 years (6 month–5 yrs) |
| CIBMTR/EBMT Review53 | Retrospective registry review | None | PFS | Data base of AHSCT for MS/46 RRMS, 186 SPMS, 32 PPMS, 17 PRMS | RRMS failed DMT, with 2 or more treated relapses or 1 treated relapse with Gd lesion at a separate time/RRMS 123, SPMS 28 | High intensity in 53/281 (18.9%); intermediate intensity in 49/281 (17.4%); low intensity in 49/281 (17.4%). | Overall PFS was 46%; among patients with RRMs/PRMS PFS was 82% at 3 years andEDSS PFS 73% at 5 years | 2.8% | 93% at 5 years | Median 6.6 yrs | |
| Czech Republic 201039 | Retrospective case series | None | Reported efficacy of AHSCT experience in MS | All patients treated with AHSCT 10 years11 RRMS, 15 SPMS | Data base of AHSCT for MS/46 RRMS, 186 SPMS, 32 PPMS, 17 PRMS | BEAM in 26 and BEAM+ATG in 16 | PFS at 3 years 70.8% and 29.2% at 6 years | Median annual relapse rate within the year before ASCT was 2, while the median annual relapse rate was 0 within the first 2 years after ASCT | Zero | 96.1% (1 death due to glioblastoma multiforme at 60 months of follow-up) | Median 66 months (11–132) |
| Spain 201757 | Retrospective case series | None | Reported toxicity and the long-term efficacy of AHSCT | RRMS/SPMS under treatment with one of the MS-approved drugs for more than 1 year, who experienced one or more relapses in the previous year and worsening of at least 1 point in disability (EDSS)22 RRMS, 9 SPMS | 31 | BEAM+rabbit ATG | 100% of RRMs were free of disability at 6 months; and 60% achieving sustained disability recovery at 6 months;22% of SPMS were free of disability at 6 months; and 10% achieving sustained disability recovery at 6 months | 32.3% (10) had at least one relapse post-AHSCT; 6 in the RRMS group (27.2%) and 4 in the SPMS group (44.4%). 7 (22.6%) experienced progression of disability, all within SP form. | Zero | 96.7% (1 death 13 years after transplant from aspiration pneumonia after progressing and reaching an EDSS of 9.5.) | Median 8.4 years (2–16) |
| Single-arm prospective study | |||||||||||
| Russia 201558 | Single arm clinical trial | None | Safety and efficacy (treatment response) | All patients treated with AHSCT 6 years: EDSS 1.5–8.0, ±Gd lesions, and no treatment with interferons or immunosuppressive agents within 3 months before enrollment | 99(43 RRMS, 56 SPMS, 18 PPMS, 3 PRMS) | Reduced intensity conditioning regimen based on BEAM | EFS for the whole group was 80%. In the group with RRMS, EFS was 83.3% and in the group with progressive course 75.5%92% EDSS PFS 5 years | 16.7% at 8 years. | Zero | 100% | Median 48.9 months |
| Northwestern/Chicago 200959 | Single arm clinical trial | None | EDSS PFS and reversal of neurologic disability | RRMS with 2 steroid treated relapses in previous 12 month. | 21(21 RRMS) | Cychophosphamide+alemtuzumab/rabbit ATG | 100% EDSS PFS 3 years | 5 patients (24%) relapsed but achieved remission after further immunosuppressionAfter a mean of 37 months (range 24–48 months), all patients were free from progression (no deterioration in EDSS score), and 16 were free of relapses | Zero | 100% | Mean 3.1 years (1.5–10) |
| Canada 201662 | Single arm clinical trial | None | MS activity-free survival (absence of clinical relapse, new MRI lesion or progression of EDSS) | Disease activity despite 1 year of DMT. | 24(12 RRMS, 12 SPMS) | Cyclophosphamide/busulfan | 70% PFS 3 years | No clinical relapse | 4.2% | 95% | Median 6.1 year (±2.5) |
| HALT-MS 2015, 201760,61 | Single arm clinical trial | None | Time to treatment failure (death or MS activity) | RRMS with failure of DMTs during the prior 18 months | 24(24 RRMS) | BEAM+rabbit ATG | 70% NEDA 5 years, 91% EDSS PFS | Two participants had disease progression and died at .2.5 years and .3.5 years after AHSCT; a third participant also had disease progression at 15 months and died at 4.5 years post-HCTOf 24 patients 7 did not maintain EFS by close of follow-up by an increase in EDSS 0.5 (n=2), clinical relapse (n=3) or development of new MRI lesions (n=2) | Zero | 87.5% | Median 4.9 year (6–12) |
| Australia 201863 | Single arm clinical trial | None | EFS (NEDA) | RRMS with at least 1 relapse or one new MRI lesion in the past year despite DMT/SPMS worsening with at least 1 MRI lesion in the past year. | 35(20 RRMS, 15 SPMS) | BEAM+horse ATG | 60% NEDA 3 year | Clinical relapses occurred in 3 patients at 12, 13 and 14 months, respectively after AHSCT | Zero | 100% | Median 6.9 year (0.7–21.6) |
| Randomized study | |||||||||||
| ASTIMS 201552 | Phase II, AHSCT vs mitoxantrone | AHSCT vs mitoxantrone | Cumulative number of new T2 lesion MRI 4 years after randomization | Worsening in EDSS and one or more MRI lesion last year despite DMTs | 21 (9 to AHSCT)7 RRMS, 13 SPMS, 1 PPMS | BEAM+ATG | New T2 lesion MRI: 2.5 AHSCT vs 8 mitoxantrone 4 years | EDSS progression was 57% in AHSCT vs 48% in the mitoxantrone (p=0.5) | Zero | 100% | 4 years |
| MIST 201855 | Phase3 AHSCT vs conventional DMT | AHSCT vs DMT | 6-Month worsening EDSS≥1.0 after one year's post-AHSCT or DMT treatment | At least 2 clinical relapse, or one relapse in MRI lesion at different time in the last year despite DMT | 110 (55 AHSCT)110 RRMS | Cyclophosphamide+rabbit ATG | At 1 year, mean EDSS improved from 3.38% to 2.36% with AHSCT and worsened from 3.31 to 3.98 with DMTs. At 1 year, mean T2 lesion volume on MRI decreased in the AHSCT, but increased in The DMT group. | 15.4% AHSCT vs 85.3% of relapse at 5 years. Disability worsening occur in 5.8% AHSCT vs 66.7% DMT group; median time to pression 24 months in the DMT. | Zero | 100% | Up to 5 years |
N: number of enrolled subjects; PFS: progression-free survival; OS: overall survival; EDSS: Expanded Disability Status Scale; TRM: transplant-related mortality; FU: follow-up; AHSCT: autologous hematopoietic stem cell transplantation; SPMS: secondary progressive MS; PPMS: primary progressive MS; PRMS: progressive relapsing; DMT: disease modifying treatment; NEDA: no evidence of disease activity (absence of relapse, disability worsening on the EDSS or MRI lesion activity); MRI: magnetic resonance imaging; Gd: gadolinium-enhanced lesion on MRI.
These studies together support the efficacy of AHSCT in patients with relapsing form of MS. Although they differed in design, population, conditioning protocol and only two were randomized with a control group, many patients experience disease activity control for a long time. The largest retrospective study was a review from the CIBMTR/EBMT register in 2017 that analyzed 281 patients.53 Overall progression-free survival rate was 46%; among patients with RRMS or PRMS, progression-free survival rates were 82% at 3 years and 73% at 5 years; OS at 5 years was 93%. Factors associated with neurologic progression post AHCT was older age, progressive versus relapsing form of MS and more than two previous disease modifying therapies (DMTs).
All the single-arm35,58–63 clinical trials demonstrated high efficacy of AHSCT for RRMS or PRMS. The first reported was by Burt et al., with 21 patients with RRMS conditioned with cyclophosphamide plus rabbit ATG/alemtuzumab, showing a EDSS progression free survival at 3 years of 100% and EDSS improvements ≥1 in 81% and no change in 9.5%, OS of 100%.59 Recently Moore at al. reported 35 patients with RRMS and SPMS in a phase 2 study conditioned with BEAM and horse ATG showing a MS activity-free survival of 82% at one year 65% at 2 years and 60% at 3 years; looking at RRMS only the MS activity-free survival was 90% at one year and 70% at 3 years.63
Only two randomized controlled trials are available: in the ASTIMS study, Mancardy et al. compared AHSCT versus mitoxantrone; 9 out 21 were randomized to AHSCT.52 They were conditioned with BEAM plus rabbit ATG. Over 4 years, the median number of new T2-weighted MRI lesions was 2.5 in the AHSCT versus 8 in the mitoxantrone group (p=0.00016) and none of those who received AHSCT had new gadolinium-enhanced MRI lesions, but 56% of those on mitoxantrone had at least 1 MRI lesion (p=0.029); EDSS progression was 57% in AHSCT vs 48% in the mitoxantrone group (p=0.50). The phase 3 MIST trial55 compared the efficacy of AHSCT versus DMTs. The conditioning was non-myeloablative, with cyclophosphamide plus rabbit ATG and 110 patients were randomized 1:1. With a follow-up of up to 5 years, disability worsening occurred in 5.8% AHSCT versus 66.7% of DMT group. At 1 year, relapse occurred in 2% in the AHSCT and 68.2% in the DMT group 9; with p<0.001 and at 5 years, relapse occurred in 15.4% AHSCT vs 85.2% DMT group; no deaths or grade 4 toxicities related to transplantation were reported.
A meta-analysis of AHSCT for MS evaluated the safety and efficacy of transplant. Led by Somani at al., it evaluated 15 studies including more than 764 transplanted patients. A proportion of NEDA (no evidence of disease activity) was found in 2 years in 83% and in 5 years 67%; the transplant-related mortality was estimated in 2.3%, the rate of EDDS progression was 17.1% at 2 years and 23.3% at 5 years.54 Another interesting study done by Sormani et al.64 evaluated a comparison of NEDA status in studies of AHSCT (n=66) with various conventional e high-efficacy MS DMTs (n=216). The use of AHSCT led to NEDA rates of 78–83% at 2 years and 60–68% at 5 years. On the other hand, DMTs lead to reported NEDA rates of 13–46% at 2 years.
Transplant-related mortality (TRM) has improved over the past 20 years.14,54 The initial reports described TRM as high as 9.5% (37, revised in 65), which later decreased to 1.3%, according to EBMT data.6,9 The incorporation of less myeloablative regimens, center experience and center accreditation have contributed to the improved outcomes.8,59,65–68
Recently the American Society of Bone Marrow Transplantation50 has conducted a comprehensive literature review, including many of the papers already discussed here, and recommended autologous HSCT as “standard of care, clinical evidence available” for treatment-refractory relapsing MS.
Guidelines for transplantation in multiple sclerosisConsidering the results presented above, HSCT can be considered for patients with relapsing-remitting form of MS, with EDSS less than 6, who have not responded to conventional treatment or progressive MS with superimposed activity. Especially if disease activity continues despite treatment with high-efficacy DMTs and worsening disability. The treatment for other MS types should follow the guidelines proposed by SBMTO previously,69 shown in Box 1 and Box 2, and using the same reduced-intensity conditioning with cyclophosphamide (200mg/kg) and rabbit anti-thymocyte (4.5mg/kg). Intensive vigilance should be maintained for short and long-term post-transplant complications, especially fever, deep vein thrombosis, pulmonary embolism, urinary tract infections, falls, metabolic syndrome and coronary disease.65,70
Indications for autologousa hematopoietic stem cell transplantation (HSCT) in multiple sclerosis (MS).
| Patients under 60 years old who are not responsive to the current first line standard therapy and who present EDDS between 3 and 6 |
| Patients with inflammatory activity in the forms:- relapsing-remitting: IB;- secondary progressive with inflammatory activity (clinical and imaging): IIB;- primary progressive with inflammatory activity (clinical and imaging): IIB |
| Patients with the “malignant” form of multiple sclerosis who developed severe disability in the previous year: IIB |
EDSS: Expanded Disability Status Scale.
a Allogeneic HSCT is not recommended for any category of MS.
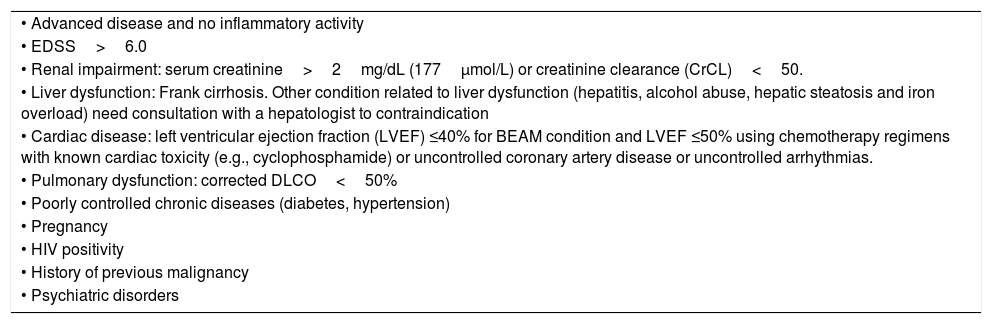
Contraindications to hematopoietic stem cell transplantation in multiple sclerosis.
| • Advanced disease and no inflammatory activity |
| • EDSS>6.0 |
| • Renal impairment: serum creatinine>2mg/dL (177μmol/L) or creatinine clearance (CrCL)<50. |
| • Liver dysfunction: Frank cirrhosis. Other condition related to liver dysfunction (hepatitis, alcohol abuse, hepatic steatosis and iron overload) need consultation with a hepatologist to contraindication |
| • Cardiac disease: left ventricular ejection fraction (LVEF) ≤40% for BEAM condition and LVEF ≤50% using chemotherapy regimens with known cardiac toxicity (e.g., cyclophosphamide) or uncontrolled coronary artery disease or uncontrolled arrhythmias. |
| • Pulmonary dysfunction: corrected DLCO<50% |
| • Poorly controlled chronic diseases (diabetes, hypertension) |
| • Pregnancy |
| • HIV positivity |
| • History of previous malignancy |
| • Psychiatric disorders |
EDSS: Expanded Disability Status Scale.
Systemic sclerosis (SSc) is a chronic autoimmune disease characterized by fibrosis of the skin and internal organs, and vasculopathy.71,72 The disease usually begins with vascular hyperreactivity and endothelial activation, which, associated with inflammatory phenomena, promotes progressive tissue damage and fibrosis.73 The etiology, still not completely understood, includes a susceptible genetic background associated with environmental stimuli, which promote immune dysregulation and, as a consequence, injury to tissues.71,73
Patients with severe and progressive forms of SSc have reduced quality of life and mortality rates that can reach 50% in five years and 70% in 10 years.74 Cardiopulmonary dysfunction is the leading cause of death, especially in patients with interstitial lung disease and pulmonary hypertension.71 A meta-analysis has shown that the mortality of patients with SSc has not decreased in the past 40 years, despite new available treatment options.75
Clinical presentationSkin involvement is a hallmark of SSc, and its extent enables clinical classification into three subtypes: limited, diffuse and sine scleroderma (without cutaneous involvement). The extent of skin involvement correlates with disease presentation and severity. Patients with the diffuse form of SSc suffer from interstitial lung disease, cardiac and renal involvement more frequently.72 This subtype tends to progress faster and with greater severity, morbidity and mortality than other forms of the disease.72,76,77 On the other hand, limited systemic sclerosis patients tend to present pulmonary hypertension as a life-threatening manifestation.
Conventional therapeutic approachesThe management of patients with systemic sclerosis (SSc) includes pharmacological and non-pharmacological approaches.78 Hand and extremity warming and protection against trauma, dietary and postural measures to reduce gastroesophageal reflux and treatment of skin and digital ulcers are recommended for most patients, given the high frequency of these manifestations.78
Conventional drug treatment is quite limited and ineffective in controlling the progression of the disease. There are no drugs that treat SSc globally, and therapeutic strategies are often organ or manifestation-directed. Currently, international rheumatology societies have developed recommendations for the treatment of patients with SSc, always according to individual manifestations.78,79 Randomized clinical studies have investigated synthetic and biological immunomodulatory agents, showing modest benefits and no repercussions on disease-related mortality, with exception of angiotensin-converting enzyme (ACE) inhibitors, which in the past significantly decreased the mortality of patients with scleroderma renal crises.59,78
Interstitial lung disease is a severe manifestation of SSc and the leading cause of death in this disease. The available treatments have modest and short-lived success rates on the control of interstitial lung disease.71,78–81 Best outcomes are described for cyclophosphamide and mycophenolate mofetil, with short-term benefit when compared with placebo.82,83 More recently, rituximab, tocilizumab, nintedanib and pirfenidone, among other therapeutic agents, have been investigated with promising results, yet to be confirmed.84–87 Isolated diffuse skin involvement, when severe and progressive, is also associated with high mortality rates and poor quality of life, with outcomes comparable to those of patients with visceral involvement.86 Thus, systemic immunosuppression is recommended for selected cases.87
Hematopoietic stem cell transplantationIn the past years 20 years, AHSCT has been indicated as treatment for patients with severe and rapidly progressive SSc.10 According to data from international transplant registries, the number of transplanted patients per year has progressively increased, reflecting the good outcomes of this therapeutic approach.14
The most recently adopted indication criteria for transplantation are the following10,88,89:
- •
An established diagnosis of systemic sclerosis, according to the 2013 ACR/EULAR classification criteria90.
- •
Patients with diffuse form of the disease, with a minimum modified Rodnan's score of 16, and worsening by at least 25% in the last 6 months, under immunosuppressive treatment.
- •
Patients with interstitial lung involvement with a decline in predicted forced vital capacity (FVC) or carbon monoxide (CO) diffusion percentages greater than 10% in the preceding 6 months, while under immunosuppressive treatment.
The exclusion criteria for HSCT to consider based on available studies are the following10,88,89:
- •
Age over 60 years;
- •
Current pregnancy;
- •
Inability to practice effective contraception;
- •
Inability to accept infertility as a possible consequence after transplantation;
- •
Severe psychiatric disorder;
- •
Current acute or chronic infection;
- •
Previous malignancy, except localized and treated cervical and thyroid cancer;
- •
Major organ dysfunction, as follows:
- •
Liver – increased alanine aminotransferase (ALT) or aspartate aminotransferase (AST), over three times the normal range; or increased serum bilirubin levels, over three times the normal range, except when Gilbert's syndrome present;
- •
Kidneys – creatinine clearance below 40ml/min; or creatinine levels above 2mg/dL;
- •
Lungs – forced vital capacity or hemoglobin-adjusted CO diffusion below 40% of predicted;
- •
Heart – left ventricular ejection fraction below 50%, constrictive pericarditis, ventricular arrhythmias, extensive myocardial fibrosis, systolic pulmonary artery pressure greater than 40mmHg or mean pulmonary artery pressure greater than 25mmHg, evidence of ventricular diastolic dysfunction, septal dyssynergia.
- •
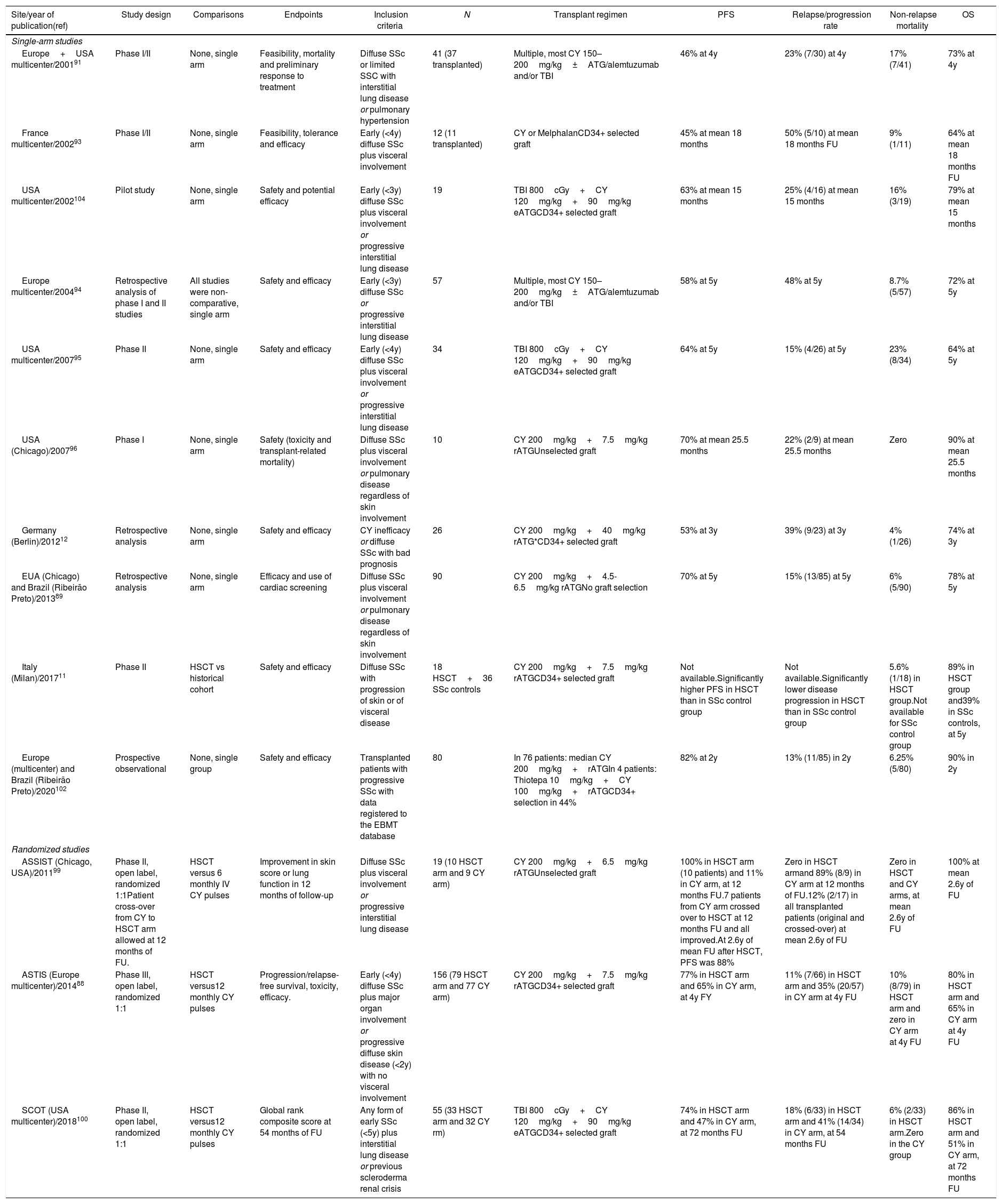
Historically, the initial studies were important to establish recommendations and guide currently adopted procedures. Phase I/II studies showed that autologous HSCT (AHSCT) improves skin involvement and at least stabilizes the pulmonary condition (Table 3).11,12,91–96 These studies also evidenced the importance of a proper heart assessment as a strategy to decrease transplant-related mortality. Cardiac dysfunctions that occur during transplantation accounted for many of the transplant-related deaths described in the initial studies.97 Currently, there are detailed cardiac assessment recommendations,98 aimed at identifying patients with previous cardiac lesions and, therefore, at a higher risk of cardiotoxicity.
Results of studies on systemic sclerosis disease.
| Site/year of publication(ref) | Study design | Comparisons | Endpoints | Inclusion criteria | N | Transplant regimen | PFS | Relapse/progression rate | Non-relapse mortality | OS |
|---|---|---|---|---|---|---|---|---|---|---|
| Single-arm studies | ||||||||||
| Europe+USA multicenter/200191 | Phase I/II | None, single arm | Feasibility, mortality and preliminary response to treatment | Diffuse SSc or limited SSC with interstitial lung disease or pulmonary hypertension | 41 (37 transplanted) | Multiple, most CY 150–200mg/kg±ATG/alemtuzumab and/or TBI | 46% at 4y | 23% (7/30) at 4y | 17% (7/41) | 73% at 4y |
| France multicenter/200293 | Phase I/II | None, single arm | Feasibility, tolerance and efficacy | Early (<4y) diffuse SSc plus visceral involvement | 12 (11 transplanted) | CY or MelphalanCD34+ selected graft | 45% at mean 18 months | 50% (5/10) at mean 18 months FU | 9% (1/11) | 64% at mean 18 months FU |
| USA multicenter/2002104 | Pilot study | None, single arm | Safety and potential efficacy | Early (<3y) diffuse SSc plus visceral involvement or progressive interstitial lung disease | 19 | TBI 800cGy+CY 120mg/kg+90mg/kg eATGCD34+ selected graft | 63% at mean 15 months | 25% (4/16) at mean 15 months | 16% (3/19) | 79% at mean 15 months |
| Europe multicenter/200494 | Retrospective analysis of phase I and II studies | All studies were non-comparative, single arm | Safety and efficacy | Early (<3y) diffuse SSc or progressive interstitial lung disease | 57 | Multiple, most CY 150–200mg/kg±ATG/alemtuzumab and/or TBI | 58% at 5y | 48% at 5y | 8.7% (5/57) | 72% at 5y |
| USA multicenter/200795 | Phase II | None, single arm | Safety and efficacy | Early (<4y) diffuse SSc plus visceral involvement or progressive interstitial lung disease | 34 | TBI 800cGy+CY 120mg/kg+90mg/kg eATGCD34+ selected graft | 64% at 5y | 15% (4/26) at 5y | 23% (8/34) | 64% at 5y |
| USA (Chicago)/200796 | Phase I | None, single arm | Safety (toxicity and transplant-related mortality) | Diffuse SSc plus visceral involvement or pulmonary disease regardless of skin involvement | 10 | CY 200mg/kg+7.5mg/kg rATGUnselected graft | 70% at mean 25.5 months | 22% (2/9) at mean 25.5 months | Zero | 90% at mean 25.5 months |
| Germany (Berlin)/201212 | Retrospective analysis | None, single arm | Safety and efficacy | CY inefficacy or diffuse SSc with bad prognosis | 26 | CY 200mg/kg+40mg/kg rATG*CD34+ selected graft | 53% at 3y | 39% (9/23) at 3y | 4% (1/26) | 74% at 3y |
| EUA (Chicago) and Brazil (Ribeirão Preto)/201389 | Retrospective analysis | None, single arm | Efficacy and use of cardiac screening | Diffuse SSc plus visceral involvement or pulmonary disease regardless of skin involvement | 90 | CY 200mg/kg+4.5-6.5mg/kg rATGNo graft selection | 70% at 5y | 15% (13/85) at 5y | 6% (5/90) | 78% at 5y |
| Italy (Milan)/201711 | Phase II | HSCT vs historical cohort | Safety and efficacy | Diffuse SSc with progression of skin or of visceral disease | 18 HSCT+36 SSc controls | CY 200mg/kg+7.5mg/kg rATGCD34+ selected graft | Not available.Significantly higher PFS in HSCT than in SSc control group | Not available.Significantly lower disease progression in HSCT than in SSc control group | 5.6% (1/18) in HSCT group.Not available for SSc control group | 89% in HSCT group and39% in SSc controls, at 5y |
| Europe (multicenter) and Brazil (Ribeirão Preto)/2020102 | Prospective observational | None, single group | Safety and efficacy | Transplanted patients with progressive SSc with data registered to the EBMT database | 80 | In 76 patients: median CY 200mg/kg+rATGIn 4 patients: Thiotepa 10mg/kg+CY 100mg/kg+rATGCD34+ selection in 44% | 82% at 2y | 13% (11/85) in 2y | 6.25% (5/80) | 90% in 2y |
| Randomized studies | ||||||||||
| ASSIST (Chicago, USA)/201199 | Phase II, open label, randomized 1:1Patient cross-over from CY to HSCT arm allowed at 12 months of FU. | HSCT versus 6 monthly IV CY pulses | Improvement in skin score or lung function in 12 months of follow-up | Diffuse SSc plus visceral involvement or progressive interstitial lung disease | 19 (10 HSCT arm and 9 CY arm) | CY 200mg/kg+6.5mg/kg rATGUnselected graft | 100% in HSCT arm (10 patients) and 11% in CY arm, at 12 months FU.7 patients from CY arm crossed over to HSCT at 12 months FU and all improved.At 2.6y of mean FU after HSCT, PFS was 88% | Zero in HSCT armand 89% (8/9) in CY arm at 12 months of FU.12% (2/17) in all transplanted patients (original and crossed-over) at mean 2.6y of FU | Zero in HSCT and CY arms, at mean 2.6y of FU | 100% at mean 2.6y of FU |
| ASTIS (Europe multicenter)/201488 | Phase III, open label, randomized 1:1 | HSCT versus12 monthly CY pulses | Progression/relapse-free survival, toxicity, efficacy. | Early (<4y) diffuse SSc plus major organ involvement or progressive diffuse skin disease (<2y) with no visceral involvement | 156 (79 HSCT arm and 77 CY arm) | CY 200mg/kg+7.5mg/kg rATGCD34+ selected graft | 77% in HSCT arm and 65% in CY arm, at 4y FY | 11% (7/66) in HSCT arm and 35% (20/57) in CY arm at 4y FU | 10% (8/79) in HSCT arm and zero in CY arm at 4y FU | 80% in HSCT arm and 65% in CY arm at 4y FU |
| SCOT (USA multicenter)/2018100 | Phase II, open label, randomized 1:1 | HSCT versus12 monthly CY pulses | Global rank composite score at 54 months of FU | Any form of early SSc (<5y) plus interstitial lung disease or previous scleroderma renal crisis | 55 (33 HSCT arm and 32 CY rm) | TBI 800cGy+CY 120mg/kg+90mg/kg eATGCD34+ selected graft | 74% in HSCT arm and 47% in CY arm, at 72 months FU | 18% (6/33) in HSCT arm and 41% (14/34) in CY arm, at 54 months FU | 6% (2/33) in HSCT arm.Zero in the CY group | 86% in HSCT arm and 51% in CY arm, at 72 months FU |
PFS: progression-free survival; OS: overall survival; N: number of enrolled subjects; USA: United States of America; y: years; SSc: systemic sclerosis; TBI: total body irradiation; IV CY: intravenous cyclophosphamide; eATG: equine anti-thymoglobulin; rATG: rabbit anti-thymoglobulin; FU: follow-up; HSCT: hematopoietic stem cell transplantation; rATG*: this center used ATG-Fresenius (Neovii-Biotech, Germany).
The three randomized studies more recently published show that HSCT surpasses conventional treatment in SSc patients, promoting longer overall survival, longer disease-free survival and higher quality of life (Table 3).88,99,100 These results are essential to convince the community about the efficacy of HSCT. In fact, since 2017, AHSCT has been recommended by the European League Against Rheumatism (EULAR) guidelines, for patients with SSc at risk of organ failure.78
Treatment protocols have been refined and incorporated into the routine of several transplant centers. However, a few points of debate still remain. There is still no consensus among centers whether to adopt graft selection or to use non-selected grafts. While CD34+ graft selection may prevent reinfusion of autoreactive cells during transplant and potential disease reactivation, it adds costs to the procedure and increases the risk of contamination and cell death. A retrospective study from the European Blood and Marrow Transplant Group (EBMT) compared SSc patients transplanted with or without graft selection, showing similar clinical outcomes.101 Although not statistically significant, patients who received unselected grafts tended to have better overall and disease-free survival than patients treated with selected grafts. More recently, a second prospective observational study from the EBMT reported, conversely, higher disease improvement rates after HSCT with CD34+ graft selection, although there was no impact on the progression-free survival.102 A third, smaller, recent study has also shown better outcomes in patients transplanted with selected versus non-selected grafts (Table 3).103 In summary, the question shall not be settled without a prospective randomized trial.
Most transplant centers adopt non-myeloablative conditioning regimens, however a group of North American multicenter investigators, from 26 transplant sites, has consistently reported their experience with myeloablative protocols including full body irradiation.95,104 In this scenario, the most recently published randomized trial (SCOT trial) has shown good results in the myeloablative transplant group (Table 3).100
The experience with allogeneic transplantation for systemic sclerosis is limited to isolated case reports.14,105,106 Therefore, clinical evidence is insufficient to recommend this treatment modality for patients with SSc.
Guidelines for transplantation in systemic sclerosisThe three randomized studies already published provide solid evidence to recommend autologous hematopoietic stem cell transplantation for severe and progressive cases of systemic sclerosis. According to the Oxford Center for Evidence-Based Medicine's evidence table,107 we consider the evidence to have Grade A and Level 1B. Patients should be thoroughly evaluated for heart dysfunction and fibrosis before transplantation and the procedure should be performed in centers with experience in managing patients with systemic sclerosis during transplantation.
Crohn's diseaseCrohn's disease is a chronic relapse-remitting inflammatory bowel disorder that can affect any site of the digestive tract.108 Currently, Crohn's is a global disease, with increasing worldwide incidence and prevalence.109 In Brazil, the prevalence of Crohn's disease varies according to the region of the country, from 12.8/100,000 in the Northeastern area, to 14.1 and 24.3/100,000 in the states of Espírito Santo and São Paulo, respectively.110–112
The disease is immunologically mediated and heterogeneous among the affected patients. The imbalanced and dysregulated immunity of the intestinal mucosa provides an inappropriate response against original intestinal flora or luminal antigens. These responses are responsible for the symptoms and the intestinal lesions observed in Crohn's disease. Disturbances in the intestinal mucosa occur in patients genetically predisposed and exposed to environmental triggers.113
The mucosal disturbance may be linked to abnormalities in the toll-like recognition receptors (TLRs), which play an essential role in the pathogenesis of numerous autoimmune diseases. The perturbation of the TLR signaling pathway in intestinal macrophages has been associated with tolerance breakdown in autoimmune diseases.114 Patients with Crohn's disease present defects in the innate immune pathway, and inadequate T cell responses to pathogenic mutations in the nucleotide-binding oligomerization domain 2 (NOD2) and autophagy-related protein 16-1 (ATG16L1) genes that impair bacterial sensing and clearing.108 Imbalances between natural (nTreg) and induced regulatory T-cells (iTreg), and effector T-helper (Th) cells (Th1/Th17) that defend the mucosa from bacteria, fungi and viruses are associated with Crohn's disease.108,115 The Genoma Wide Association Study Project identified 71 susceptibility loci on 17 chromosomes and regions related to inflammatory bowel disease, renamed IBD1 to IBD9.116
The age at diagnosis, disease location and behavior along the gastrointestinal tract are defined according to Montreal classification.117 The cardinal symptoms of Crohn's disease include abdominal pain, diarrhea, hematochezia, bloody stools, fatigue, weight loss, fever, recurrent fistulas, and extraintestinal manifestations.118 Extraintestinal manifestations are common, such as arthropathy (both axial and peripheral), ocular involvement (uveitis, scleritis, and episcleritis), dermatological (including pyoderma gangrenosum and erythema nodosum), nephrolithiasis, hepatobiliary involvement (primary sclerosing cholangitis), cholelithiasis, venous or arterial thromboembolism, and other associated immune-mediated diseases.119
The majority of patients (80%) present small bowel involvement, 1/3 only ileitis, 1/3 ileocolonic involvement and in 1/3, Crohn's disease is restricted to the colon and rectum. In a North American cohort, 30% of patients presented perianal disease, while in Europe this complication was detected in only 9% of patients.120 Oral and gastroduodenal involvement is estimated in approximately 10% of Crohn's disease patients.120 Fistulas are common: enteric, cutaneous, vesical, vaginal, anal, or rectal. Complications in the involved organs, such as abdominal masses and abscesses, are frequent, with perianal fistulizing disease in up to one-quarter of the patients.119 At diagnosis, most (71%) patients present a non-stricturing and non-penetrating profile of disease, but 21% have a stricturing and 8% a penetrating behavior.120
Surgery due to intestinal inflammation or related complications, such as stenosis, fistulas or perforations, occurs in 13% of patients in the first year of diagnosis, and 22% in five years of follow-up. The 10-year cumulative risk of major abdominal surgery is of approximately 55%.108,109,119,120
Diagnosis of Crohn's disease is based on the combination of a history of chronic intestinal inflammation symptoms and colonoscopy, magnetic resonance enterography and histopathological findings.119 Routine laboratory studies include complete blood count, basic metabolic panel, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), liver function tests, iron distribution studies, vitamin B12 and D levels, β2 microglobulin and an immunologic panel study.121
Ileocolonoscopy and biopsy are considered gold standard tools for diagnosis of Crohn's disease. When visualizing the ileum, right, transverse and left colon, abnormalities in the rectum mucosa and lesions are observed as cobblestones, with nodularity, edema, superficial or deep ulcerations, friability, or stenosis. The Crohn's Disease Endoscopy Severity Index (CDEIS) and the Simple Endoscopy Score for Crohn's disease (SES-CD) were developed and validated to evaluate the compromised intestinal surface, and to characterize the severity of the involvement.122,123 All lesions should be biopsied for histological study. Upper endoscopy should only be performed in patients with upper gastrointestinal signs and symptoms and wireless capsule endoscopy may be an option for patients without intestinal strictures.119 Magnetic resonance enterography is a suitable method for the diagnosis, as the location, extension, disease activity, presence of obstructions, fistulas, and severity of inflammatory lesions of Crohn's disease need to be determined.124
Disease activity is measured by scores, such as the Crohn's Disease Activity Index (CDAI), and the Harvey Bradshaw index (HBi).125,126 A CDAI below 150 is defined as disease remission. A HBi below five defines remission, 5–7 mildly active disease, 8–16 moderately active disease and higher than 16, severe disease.
Treatment aims to stabilize Crohn's disease, reduce symptoms, and heal intestinal lesions. Anti-inflammatory drugs, immunosuppressive agents, corticosteroids, and biological agents are prescribed alone or in combination. Drugs are usually administered in a stepwise sequence, named “up and down” treatment. In more severe cases, early indication of biological agents associated with immunosuppressants remain controversial and debated.108
Hematopoietic stem cell therapyHematopoietic stem cell transplantation (HSCT) has emerged as a potential treatment for Crohn's disease due to the chronicity of the disease and lack of further therapeutic options in refractory patients. Additionally, since 1993, there are several case reports in the literature of Crohn's disease patients with concomitant leukemia or lymphoma who improved from the former when transplanted for the latter.127–132
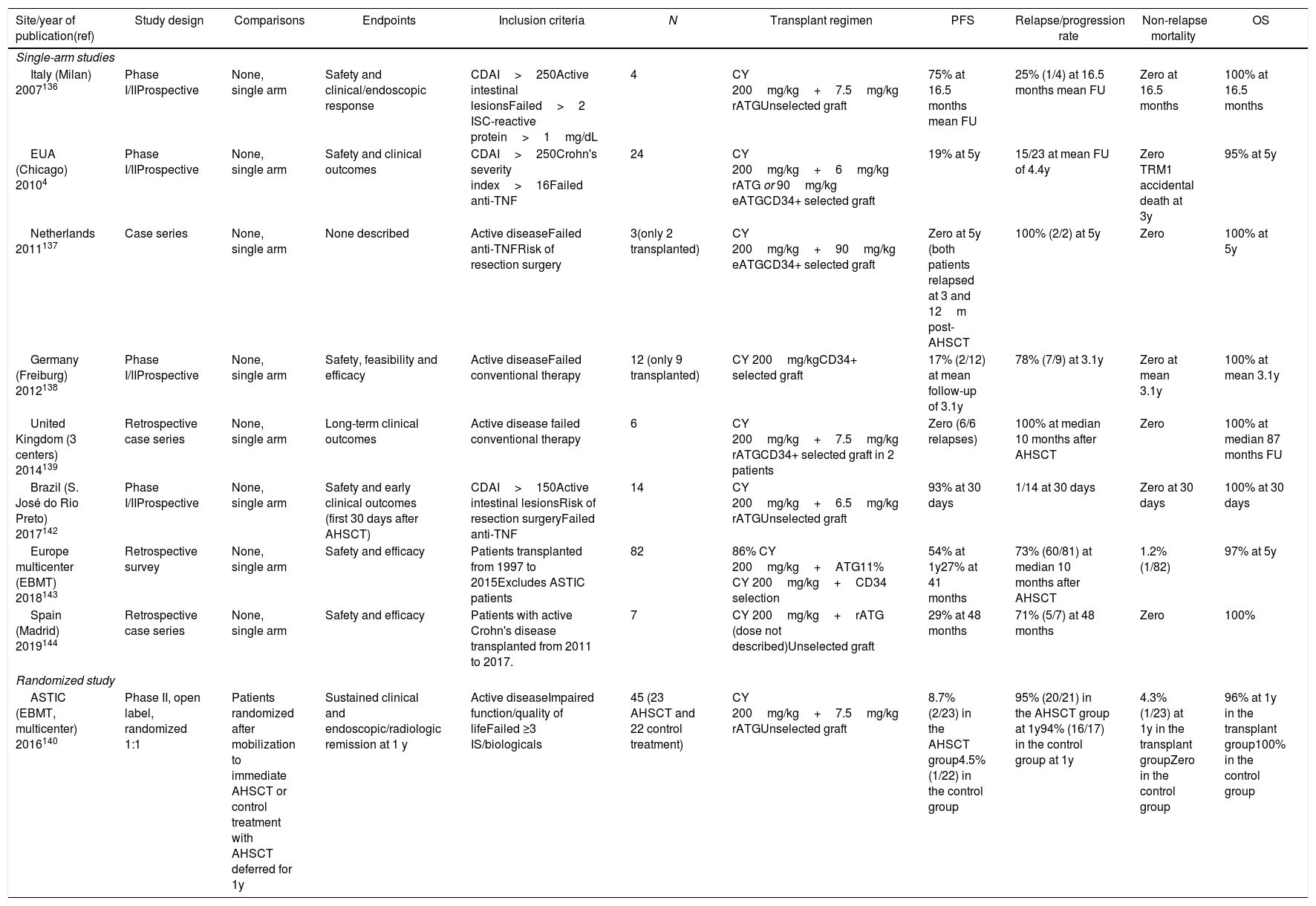
In 2003, investigators from the Northwestern University (Chicago, USA) published their successful experience with the first two patients treated with AHSCT for Crohn's disease as primary indication.133,134 A subsequent update from the same investigators described dramatic clinical remissions in 11 from a total of 12 transplanted patients, in 18 months of follow-up.135 In 2010, a last update described the long-term follow-up of 24 Crohn's disease patients transplanted in Chicago, showing high rates of disease progression over a five-year follow-up (Table 4).4
Results of Crohn's disease study outcomes.
| Site/year of publication(ref) | Study design | Comparisons | Endpoints | Inclusion criteria | N | Transplant regimen | PFS | Relapse/progression rate | Non-relapse mortality | OS |
|---|---|---|---|---|---|---|---|---|---|---|
| Single-arm studies | ||||||||||
| Italy (Milan) 2007136 | Phase I/IIProspective | None, single arm | Safety and clinical/endoscopic response | CDAI>250Active intestinal lesionsFailed>2 ISC-reactive protein>1mg/dL | 4 | CY 200mg/kg+7.5mg/kg rATGUnselected graft | 75% at 16.5 months mean FU | 25% (1/4) at 16.5 months mean FU | Zero at 16.5 months | 100% at 16.5 months |
| EUA (Chicago) 20104 | Phase I/IIProspective | None, single arm | Safety and clinical outcomes | CDAI>250Crohn's severity index>16Failed anti-TNF | 24 | CY 200mg/kg+6mg/kg rATG or 90mg/kg eATGCD34+ selected graft | 19% at 5y | 15/23 at mean FU of 4.4y | Zero TRM1 accidental death at 3y | 95% at 5y |
| Netherlands 2011137 | Case series | None, single arm | None described | Active diseaseFailed anti-TNFRisk of resection surgery | 3(only 2 transplanted) | CY 200mg/kg+90mg/kg eATGCD34+ selected graft | Zero at 5y (both patients relapsed at 3 and 12m post-AHSCT | 100% (2/2) at 5y | Zero | 100% at 5y |
| Germany (Freiburg) 2012138 | Phase I/IIProspective | None, single arm | Safety, feasibility and efficacy | Active diseaseFailed conventional therapy | 12 (only 9 transplanted) | CY 200mg/kgCD34+ selected graft | 17% (2/12) at mean follow-up of 3.1y | 78% (7/9) at 3.1y | Zero at mean 3.1y | 100% at mean 3.1y |
| United Kingdom (3 centers) 2014139 | Retrospective case series | None, single arm | Long-term clinical outcomes | Active disease failed conventional therapy | 6 | CY 200mg/kg+7.5mg/kg rATGCD34+ selected graft in 2 patients | Zero (6/6 relapses) | 100% at median 10 months after AHSCT | Zero | 100% at median 87 months FU |
| Brazil (S. José do Rio Preto) 2017142 | Phase I/IIProspective | None, single arm | Safety and early clinical outcomes (first 30 days after AHSCT) | CDAI>150Active intestinal lesionsRisk of resection surgeryFailed anti-TNF | 14 | CY 200mg/kg+6.5mg/kg rATGUnselected graft | 93% at 30 days | 1/14 at 30 days | Zero at 30 days | 100% at 30 days |
| Europe multicenter (EBMT) 2018143 | Retrospective survey | None, single arm | Safety and efficacy | Patients transplanted from 1997 to 2015Excludes ASTIC patients | 82 | 86% CY 200mg/kg+ATG11% CY 200mg/kg+CD34 selection | 54% at 1y27% at 41 months | 73% (60/81) at median 10 months after AHSCT | 1.2% (1/82) | 97% at 5y |
| Spain (Madrid) 2019144 | Retrospective case series | None, single arm | Safety and efficacy | Patients with active Crohn's disease transplanted from 2011 to 2017. | 7 | CY 200mg/kg+rATG (dose not described)Unselected graft | 29% at 48 months | 71% (5/7) at 48 months | Zero | 100% |
| Randomized study | ||||||||||
| ASTIC (EBMT, multicenter) 2016140 | Phase II, open label, randomized 1:1 | Patients randomized after mobilization to immediate AHSCT or control treatment with AHSCT deferred for 1y | Sustained clinical and endoscopic/radiologic remission at 1 y | Active diseaseImpaired function/quality of lifeFailed ≥3 IS/biologicals | 45 (23 AHSCT and 22 control treatment) | CY 200mg/kg+7.5mg/kg rATGUnselected graft | 8.7% (2/23) in the AHSCT group4.5% (1/22) in the control group | 95% (20/21) in the AHSCT group at 1y94% (16/17) in the control group at 1y | 4.3% (1/23) at 1y in the transplant groupZero in the control group | 96% at 1y in the transplant group100% in the control group |
PFS: progression-free survival; OS: overall survival; N: number of enrolled subjects; USA: United States of America; y: years; CDAI: Crohn's disease activity index; TRM: transplant-related mortality; IV CY: intravenous cyclophosphamide; eATG: equine anti-thymoglobulin; rATG: rabbit anti-thymoglobulin; FU: follow-up; HSCT: hematopoietic stem cell transplantation; anti-TNF: treatment with anti-tumor necrosis factor monoclonal antibody; IS: immunosuppressors; biologicals: biological agents.
The European centers also reproduced the North-American protocol, with similar outcomes of low toxicity and high rates of short-term disease remission.136 Longer follow-up, however, confirmed the high relapse/progression rates.137–144 A European multicenter randomized study (Autologous Stem Cell Transplantation in Refractory Crohn's Disease, ASTIC) had a very strict study design and ambitious endpoints, and thus failed to show superiority of AHSCT versus mobilization only (Table 4).140 A later reassessment of the same results, with more traditional endpoints, enabled more optimistic conclusions; that AHSCT promotes clinical and endoscopic benefits, despite a high burden of adverse events.145 To date, the EBMT registry reports Crohn's disease as the third most frequent autoimmune disease indication for AHSCT.141
In Brazil, the first report of AHSCT for Crohn's disease was published in 2013.142 To date, at least 57 procedures have been performed in four Brazilian centers (unpublished data). A single institution Brazilian trial enrolled 14 Crohn's disease patients for AHSCT with high rate of disease remissions and improved quality of life at 30 days post-transplantation (Table 4).146 Longer follow-up of the quality of life in these patients, evaluated by the IBDQ (Inflammatory Bowel Disease Questionnaire) and SF-36 (Short Form-36) questionnaires show sustained benefit at four years post-AHSCT (data not published).
The field of AHSCT for Crohn's disease has advanced over time, in parallel to the learning curve in other autoimmune disease indications. Patient selection and disease stratification are important steps that precede AHSCT, and aim to improve safety and post-transplantation outcomes.46,143 Perianal disease, fistulas and intra-abdominal abscesses, as well as presence of ostomies, are not considered absolute exclusion criteria, but increase risks associated to the procedure and should be carefully considered before patient enrollment. Moreover, hematopoietic progenitor cells may be successfully and safely mobilized from the peripheral blood with low (2g/m2) doses of cyclophosphamide.147 Disease reactivation over time is still high (Table 4) and whether CD34+ graft selection has any effect on long-term control remains to be defined.4,136–140,142,143 Finally, there is evidence to suggest that after AHSCT, patients become more responsive to conventional therapy than before the procedure.140,141 These aspects should be explored in future studies.
The new ongoing protocols, ASTIC-Lite (ASTIC-low intensity therapy evaluation, EBMT), and the AutoCrohn2 (São José do Rio Preto, Brazil), include a more refined patient assessment and stratification with accurate clinical, immunological, magnetic resonance and microbiota studies. These studies aim for a better understanding of the therapeutic potential of AHSCT for patients with Crohn's disease.147–149
Guidelines for transplantation in Crohn's diseaseAutologous HSCT has the potential to induce clinical remission and improve quality of life in patients with Crohn's disease with poor prognosis or that are refractory to immunosuppressants or biologic agents. AHSCT is considered safe, but associated with a high number of adverse events, mainly infectious. Therefore, AHSCT for Crohn's disease should be performed by experienced centers, with specialized teams to manage gastrointestinal and infectious complications. Early referral is recommended to optimize clinical outcomes and minimize risks.
ConclusionsScientific evidence supports the clinical use of autologous hematopoietic stem cell transplantation (AHSCT) for multiple sclerosis (MS), systemic sclerosis and Crohn's disease. In systemic sclerosis, AHSCT is indicated due to the severity of the disease and lack of therapeutic options, with effectiveness confirmed by phase III randomized trials. In MS, treatment with AHSCT is supported by 25 years of research, including recent phase III trials comparing transplant to new drugs. In Crohn's disease refractory to treatment with immunosuppressor and biological agents, long-term benefits have been shown after AHSCT, despite low rates of sustained disease remission.
The role of HSCT in these and in other autoimmune diseases is likely to evolve further with increased clinical experience, especially with regards to optimal timing of transplant. It is expected that improvements in design of clinical trials and experimental studies further expand the impact of HSCT in this field.
Conflicts of interestThe authors declare no conflicts of interest.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.


